
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-953X
ISSN (Online) : 2788-9548
Altered voice due to vocal cord palsy may be the only manifestation of an underlying serious medical condition. Malignancy (especially lung cancer) and iatrogenic trauma (following thyroid surgery) are the most common causes. The longer intrathoracic course of left recurrent laryngeal nerve (RLN) makes it vulnerable to involvement by numerous conditions mainly of mediastinal origin. Vocal cord palsy due to RLN involvement by mediastinal lymphadenopathy of benign and inflammatory aetiologies is uncommon, but includes pulmonary tuberculosis. Involvement of RLN in mediastinal disease is rare. We describe such a case of mediastinal tuberculous lymphadenitis presenting as right vocal cord palsy diagnosed by computed tomography scan. A-24 years-old female presented with acute history of hoarseness of voice and right neck swelling. Indirect laryngoscopy revealed paramedian position of right true vocal cord. CECT chest confirmed the mediastinal lymphadenopathy. Supraclavicular lymph node cytology came positive for Mycobacterium tuberculosis on CBNAAT. Patient was started on category 1 anti tubercular treatment and is on follow up.
Background
TB lymphadenitis is seen in nearly 35% of extrapulmonary TB which constitutes approximately 15-20% of all TB cases in India [1].Intrathoracic lymphadenopathy (hilar, paratracheal, mediastinal in decreasing order) is rare compared to cervical, supraclavicular, axillary lymph nodal tuberculosis [2]. About 80% of lymph nodal TB is seen in cervical lymph nodes, whereas in 6.6% mediastinal lymph nodes are involved [3]. Tuberculous mediastinal lymphadenopathy rarely causes recurrent laryngeal nerve (RLN) palsy which manifests as hoarseness of voice [4].
Case Presentation
A -24-years- old female, home maker, non-smoker presented with hoarseness of voice for two weeks and painful swelling right side neck for two weeks.(Figure 1) Patient had no history of fever, weight loss, fatigability and loss of apetite. She gave contact history of tuberculosis in family. In the evaluation of hoarseness of voice , video laryngoscopy revealed right true vocal cord in paramedian position with no morphological changes in the cord.(Figure 2) Chest radiograph revealed increased right paratracheal stripe.(Figure 3) CECT neck and chest showed peripherally enhancing lymph nodes in prevascular,pre, paratracheal, pre, subcarinal ,supraclavicular region largest of size 21 mm in SAD in right paratracheal region.(Figure 4,5,6) Sputum for CBNAAT was negative for patient. ESR was elevated .TLC was normal. Diagnostic bronchoscopy revealed no endobronchial lesion. Further diagnostic workup was carried out using USG guided cytology taken from right supraclavicular lymph node and was sent for CBNAAT which came out positive for tuberculosis sensitive to rifampacin. Patient was started on anti tubercular treatment as per national guidelines and is kept on follow up.

Figure 1: External Neck Examination
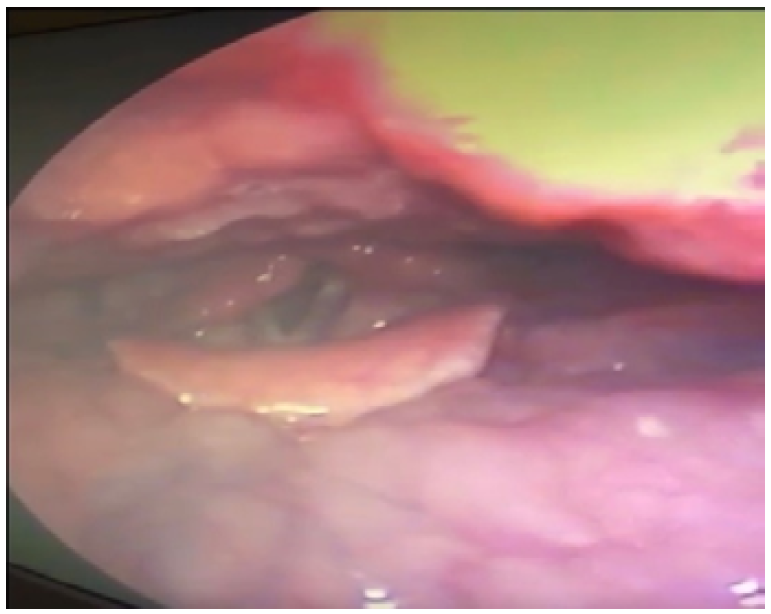
Figure 2: Endoscopic View of the Throat / Larynx (Laryngoscopy)
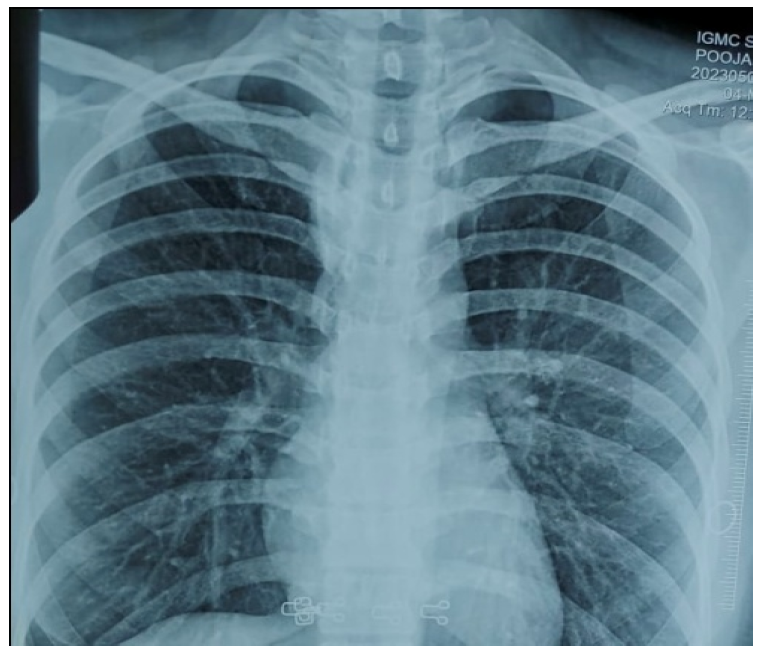
Figure 3: Chest X-Ray
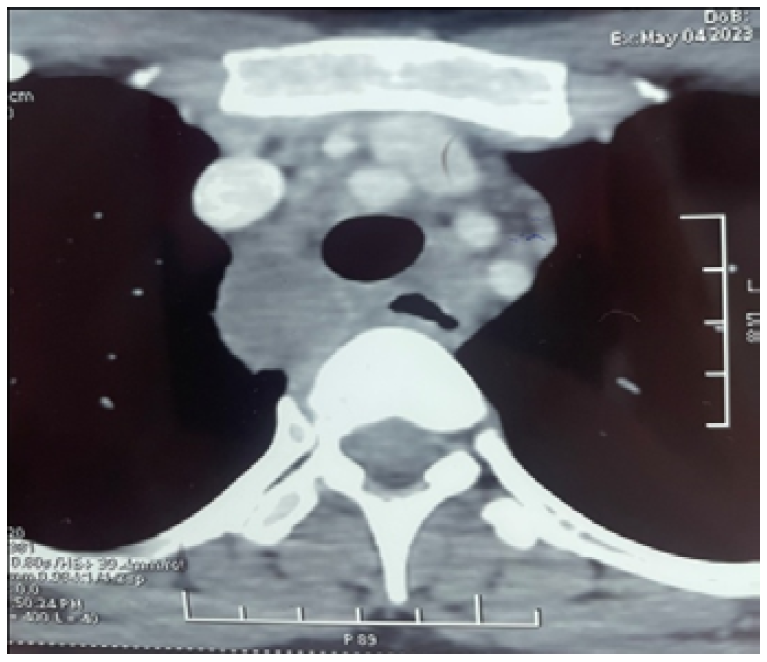
Figure 4: Axial CT Image of the Upper Thorax Showing Mediastinal Structures
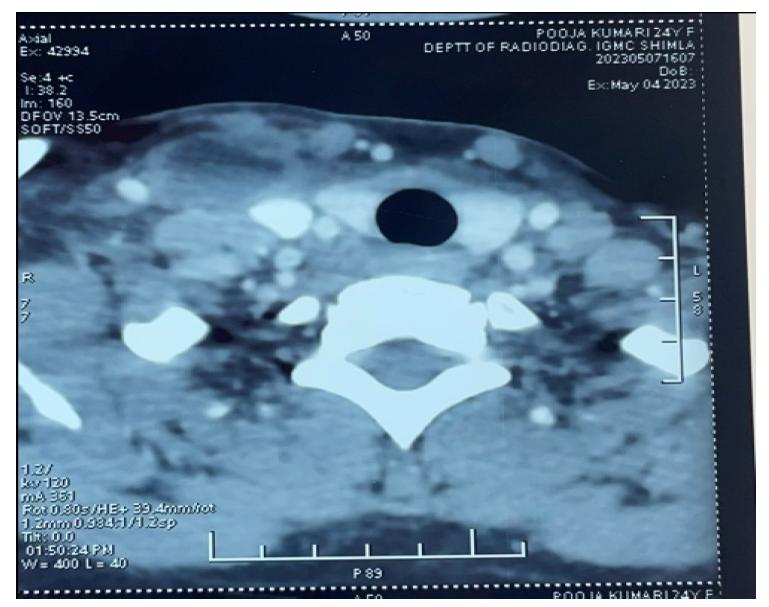
Figure 5: Axial CT Image at Cervical–Thoracic Level Showing Trachea and Surrounding Soft Tissues
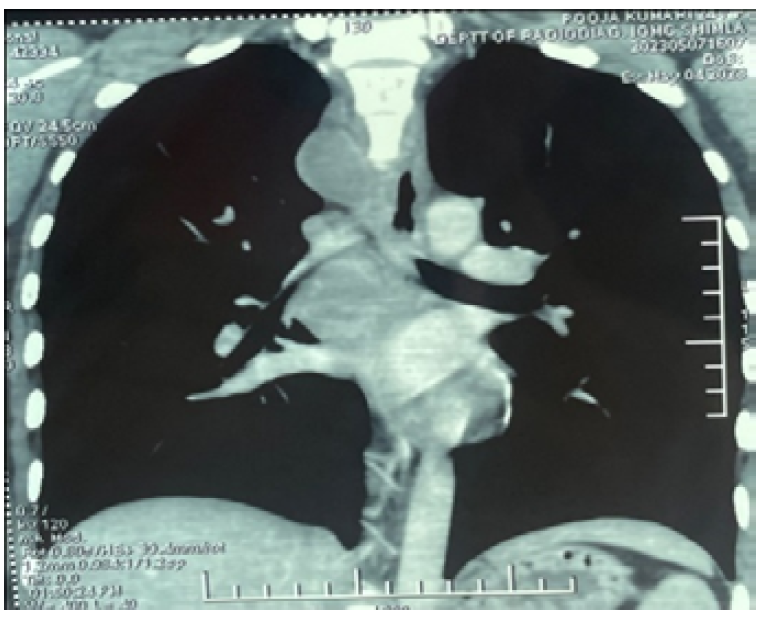
Figure 6: Coronal CT Image of the Thorax Showing Mediastinum and Bilateral Lung Fields
All cases of vocal cord palsy need to be carefully evaluated by clinical examination and investigations. Where no local or neck cause for the paralysis is identified, chest pathology needs to be excluded, first by a plain chest radiograph, and if this is normal by CT scan extending from base of skull to lung apex for a right vocal cord palsy and to the left lung hilum for a left vocal cord palsy [5]. Laryngeal malignancy, trauma, thyroid surgeries are the most common causes of vocal cord palsy [6]. Hoarseness of voice from RLN palsy due to TB mediastinal adenopathy is rarely reported. In countries like India, which is one of the high TB endemic countries, involvement of mediastinal lymph nodes by tuberculosis is frequently seen, but the recurrent laryngeal nerve palsy presenting with hoarseness of voice is a very uncommon presentation [6-7]. Hoarseness of voice in non-traumatic and non-surgical clinical scenarios, like in our patient, usually alerts the clinician to rule out mediastinal lesions which can be malignant or tubercular. In mediastinal tubercular lymphadenopathy, the paralysis of RLN, particularly on left side, can be attributed either to the mass of caseating lymph node affecting the nerve, trapping of the nerve in fibrous tissue or from stretching of the nerve due to retraction of left upper lobe bronchus towards apex [8-9]. Various other pathogenetic mechanisms have been proposed by different authors in left RLN palsy from tuberculous mediastinal adenopathy. Fowler and Hetzel stated that direct spread of infection from perforated lymph node abscess damage the RLN that results in persistent nerve damage [9]. Rafay, in his case report discusses the ‘compression dysfunction hypothesis’ where in enlarged, inflamed TB lymph nodes in the unique location of the aorto-pulmonary window and arch of aorta, in a confined space, predisposes to RLN palsy. Complete recovery of the vocal cord palsy is noted after ATT, justifying this hypothesis [10]. Involvement of right RLN in mediastinal lesion is rare. It can be attributed either to mass effect of caseating lymph node or entrapement of nerve in fibrous tissue.
Tubercular mediastinal lymphadenopathy is an important, reversible cause of isolated vocal cord palsy. The present case report epitomizes that a patient presenting with hoarseness of voice should undergo evaluation for mediastinal lesions, conjointly working up for etiological diagnosis of tuberculosis. Early diagnosis and prompt treatment with ATT will reduce morbidity, sequalae and mortaliy from this treatable disease.
Sharma, S.K. and Mohan, A. “Extrapulmonary tuberculosis.” Indian Journal of Medical Research vol. 120, year 2004, pp. 316–353.
Gupta, P.R. “Difficulties in managing lymph node tuberculosis.” Lung India vol. 21, no. 4, 2004, pp. 50.
Benjelloun, A. et al. “Lymph nodes tuberculosis: a retrospective study on clinical and therapeutic features.” Pan African Medical Journal vol. 20, year 2015, pp. 65.
Farmer, W.C. et al. “Vocal cord paralysis due to pulmonary tuberculosis.” American Review of Respiratory Disease vol. 112, no. 4, 1975, pp. 565–569.
Song, S.W. et al. “CT evaluation of vocal cord paralysis due to thoracic diseases: a 10-year retrospective study.” Yonsei Medical Journal vol. 52, no. 5, 2011, pp. 831–837.
Meral, M. et al. “Mediastinal lymphadenopathy due to mycobacterial infection.” Japanese Journal of Infectious Diseases vol. 57, no. 3, 2004, pp. 124–126.
Rajasekaran, V. and Srividhya, G. “A clinical study on laryngeal manifestations of tuberculosis.” International Journal of Otorhinolaryngology and Head and Neck Surgery vol. 3, year 2017, pp. 845–848.
Radner, D.B. and Snider, G.L. “Recurrent laryngeal nerve paralysis as a complication of pulmonary tuberculosis: a report of two cases.” American Review of Tuberculosis vol. 65, no. 1, 1952, pp. 93–99.
Fowler, R.W. and Hetzel, M.R. “Tuberculous mediastinal lymphadenopathy can cause left vocal cord paralysis.” British Medical Journal vol. 286, no. 6377, 1983, pp. 1562.
Rafay Mohammed, A. “Tuberculous lymphadenopathy of superior mediastinum causing vocal cord paralysis.” Annals of Thoracic Surgery vol. 70, year 2000, pp. 2142–2143.
