
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Aims: This study aimed to compare left ventricular (LV) function and clinical/biologic features between septal and apical pacing over a six-month follow-up period in patients with high-grade atrioventricular block. Methods: This non-randomized prospective single-center study includes patients allocated to receive an apical or midseptal ventricular lead. Computed tomography was used to confirm the intended lead tip position. Pacemaker parameters, QRS duration, LV volumes and ejection fraction, European Quality of Life Score, Functional Class, Six-minute Walk test, and NT-proBNP were assessed at baseline and six months later. Results: A pacemaker was implanted in 58 patients (27 in the midseptal group and 31 in the apical group). No significant differences between the two groups were observed at baseline. Paced QRS duration was significantly lower in the midseptal than apical pacing group (p = 0.002). After six months follow-up period, pacing parameters remained comparable between the two groups while patients assigned to the midseptal pacing group have a higher ejection fraction (p = 0.016). Higher LV end-diastolic and end-systolic volumes were observed in the apical than midseptal pacing group at 6 months (p = 0.008 and p = 0.003, respectively). At 6 months, the midseptal group has lower serum NT-proBNP (p = 0.003) and higher six-minute walk test distance (p = 0.030). Nevertheless, EuroQol index and NYHA>1 show no statistical difference. Conclusions: Compared with right ventricular (RV) apical pacing, midseptal pacing was associated with better LV ejection fraction and six-minute walk test, and lower LV volumes and NT-proBNP levels. RV midseptal pacing might be a better option than regular RV apical pacing to lessen its negative effects.
Permanent pacemaker implantation is increasing each year; by 2023, 1.43 million units are anticipated to have been implanted [1]. The right ventricular (RV) apex is the usual location for the pacing lead. Chronic RV apical pacing has been associated with adverse clinical and hemodynamic consequences [2,3]. In addition, RV apical pacing may result in impaired left ventricular (LV) function, particularly with baseline low ejection fraction [4-6]. Implanting RV leads in nonapical locations and/or avoiding RV pacing are two ways used to prevent these detrimental effects. It had been suggested that RV midseptal pacing promotes a more effective ventricular contraction [7]. A meta-analysis of fourteen randomized studies [8] reports that RV midseptal pacing is associated with a better LV ejection fraction during follow-up in comparison to apical pacing.
Many studies found the insufficiency of fluoroscopic and electrocardiographic methods to implant the leads on the true RV septum [9-16]. These are the rationale for confirming the lead tip position by computed tomography (CT). To my knowledge, this is the first research to compare the effects of septal versus apical sites of RV pacing after verification by computed tomography to find the real benefit of septal pacing as compared to other studies.
This study aimed to compare LV function and clinical/biologic features between RV septal and apical pacing over a six-month follow-up period in patients who required RV pacing for high-grade atrioventricular block.
Study Population
This non-randomized prospective single-center study includes patients with second-degree Mobitz type II and third-degree (complete) atrioventricular (AV) block necessitating implantation of dual chamber pacemaker (DDD) per current recommendations (Class I) [17] from November 2020 to July 2022. The study was done in a tertiary cardiac center (Ibn al-Bitar Specialized Center for Cardiac Surgery, Baghdad, Iraq). Patients were excluded if any of the following conditions were present: age less than 18 years, chronic pulmonary disease, atrial fibrillation, significant structural heart disease, heart failure, musculoskeletal condition that interfered with the ability to complete the six-minute walk test, need for implantable cardioverter-defibrillator or cardiac resynchronization therapy, or prior device implanted. Patients who met the requirements to participate in the research were then allocated to receive an apical or midseptal ventricular lead.
The study was carried out in compliance with the Declaration of Helsinki of 1964 and its later amendments, with informed consent obtained from all participants and approval of the Local Ethics Committee. The flow chart of the study sample selection was shown in Figure 1.
Pacemaker Implantation Technique
Active fixation ventricular leads were used to implant the initial pacemaker in the midseptum or apex. The generator and leads were from the same manufacturer in the same patient. Venous access by axillary puncture was used in all patients. Atrial lead implantation in the right atrial appendage was done using a conventional pre-shaped passive lead. Depending on allocation, an active fixation lead with a stylet was inserted and guided to the RV midseptum or apex under fluoroscopic monitoring. Using a manually shaped stylet, the RV lead was advanced across the tricuspid valve to reach the midseptal position, which was confirmed by frontal, lateral, right and left anterior oblique fluoroscopic views, and electrocardiographic features [18] (a QR wave in aVL, a positive QRS in V6 with any of the inferior leads having a positive QRS). Then screwing of the lead tip was done on the midseptum or apex. The technique had been previously described [16,19]. The final position was confirmed by ECG-gated cardiac computed tomography [12]. Done the second day after the procedure and the patients with RV leads not confirmed to be in the allocated position were excluded. No technical issues arose during or after the operation.
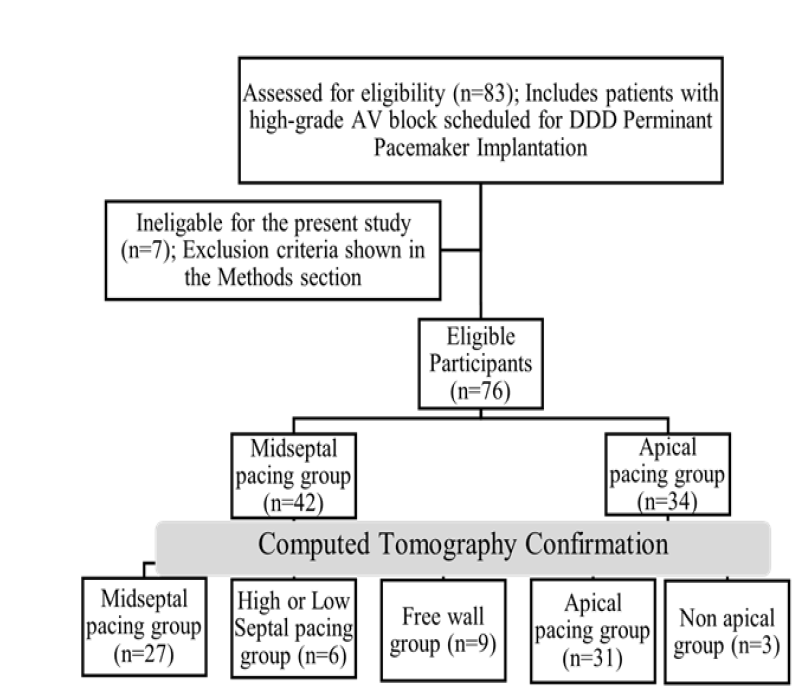
Figure 1: Flow Chart of the Study Sample Selection
Computed Tomography
The center's routine CT coronary angiography protocol was used to perform CT imaging using a single source 64-slice multidetector computed tomography scanner (Brilliance 64, Philips Healthcare, the Netherland). Cardiac acquisition protocol with ECG-gating and body mass index weighted tube voltage (100–140 kV) were used. A 70-mL 20 percent contrast/saline bolus was given as a flush after administering 60 mL of intravenous iodixanol contrast at a flow rate of 6 mL/s to delineate the interventricular septum. A slice thickness of 0.75 mm and 512x512 image matrix were used for image reconstruction. Images were modified and viewed on Comprehensive Cardiac Analyses, Brilliance Workstation (Philips Healthcare, the Netherland). Short- and long-axis planes were used to establish the RV lead position as reported by Pang et al., [15]. The infundibulum, inlet, and trabeculated body are the three segments of the RV complicated structure. The nearly conical LV is encircled by the RV. The right bundle branch, which goes within the septo-marginal trabeculation and subsequently the moderator band ends in the anterior papillary muscle on the anterior RV free wall. The septo-parietal trabeculations make a connection between the RV free wall and infundibulum to the septo-marginal trabeculation [20]. It is believed that pacing in the septo-marginal trabeculation, which is near the His bundle or right bundle branch, will promote more physiological stimulation [21]. The septum was divided into three thirds (high, mid, and lower) with midseptal position in the mid-third. Patients with leads in the high and low septal or free wall were excluded. A cardiologist with competence in cardiac CT reviewed all the images.
Pacemaker Programming and Interrogation
Initially, the pacemaker was set to dual chamber demand pacing (DDD) mode (60 beats per minute). The nominal values of sensed AV interval (120 ms) and paced AV interval (150 ms) were programmed. A digital ECG machine (Philips PageWriter TC30, the Netherlands) was used to record a surface 12-lead electrocardiogram (ECG) at 25 mm/s paper speed to measure the paced QRS duration. The mean duration of all 12 leads was used to calculate the QRS duration automatically. Immediately following the procedure and at the 6-month follow-up appointment, lead impedance capture threshold, and R-wave amplitude were all assessed.
Transthoracic Echocardiography
Cardiac function parameters were calculated and compared for both RV midseptal and apical pacing groups, 1 day and 6 months postoperatively. Indicators reflecting LV function were the following: LV end-diastolic and end-systolic volumes indexed to body surface area (LVEDVi and LVESVi, respectively), and LV ejection fraction by modified Simpson biplane method [22] were measured using GE Vivid E9 echocardiography machine (GE Medical Systems, Chicago, USA). All echocardiographic analyses were carried out while on paced rhythm.
Follow-Up Parameters
The patients were assessed the day following implantation (baseline evaluation) and six months later. The evaluation included a complete clinical interview including history taking and physical examination, 12-lead electrocardiogram, the European Quality of Life [EuroQol] EQ-5D score [23], six-minute walk test [24], New York Heart Association Functional Class (NYHA), transthoracic echocardiography, pacemaker interrogation (lead impedance, pacing threshold, R-wave amplitude, and ventricular pacing percentage), and N Terminal-proBrain Natriuretic Peptide (NT-proBNP) measurement. Also, baseline laboratory investigation includes estimated Glomerular Filtration Rate (eGFR) [25], serum electrolytes, and hemoglobin level.
Statistical Analysis
The continuous data are expressed as the mean ± SD and categorical data were expressed as numbers and percentages. Comparisons between groups (midseptal and apical pacing groups) were performed using analysis of variance for continuous variables and the Chi-Square test for categorical variables. Data were analyzed on Windows using the Statistical Package for Social Sciences (SPSS) version 26 (SPSS, Inc, Chicago, IL). Statistical significance was defined as p <0.05.
A pacemaker was successfully implanted in 58 subjects, and computed tomography verify the intended lead position in the RV. Twenty-seven patients were allocated in the midseptal group and 31 patients in the apical group. No major complications or lead dislodgement occurred during and after the implantation procedure. The midseptal pacing group's mean age was 67.01±10.77 years, similar to the apical pacing group 68.78±9.70 years (p = 0.514). Likewise, the female proportion was 55.6% in the midseptal pacing group and 51.6% in the apical pacing group (p = 0.764). There is no significant difference between the two groups regarding the presence of concomitant diseases, body mass index, type of AV block, estimated Glomerular Filtration Rate, serum electrolytes, hemoglobin level, medication use, baseline LV ejection fraction, and pacing system manufacturer. The study baseline characteristics are presented in Table 1.
Table 1: Baseline Characteristics
| Parameters | RV Midseptal Pacing (n = 27) | RV Apical Pacing (n = 31) | p |
| Age, years | 67.01±10.77 | 68.78±9.70 | 0.514 |
| Female, n (%) | 15(55.6) | 16(51.6) | 0.764 |
| BMI, kg/m2 | 27.90±3.05 | 28.34±4.26 | 0.657 |
| Diabetes, n (%) | 12(44.4) | 13(41.9) | 0.847 |
| Hypertension, n (%) | 17(63.0) | 18(58.1) | 0.704 |
| Coronary Artery Disease, n (%) | 4(14.8) | 4(12.9) | 0.833 |
| ACEi/ARB, n (%) | 14(51.9) | 13(41.9) | 0.450 |
| Beta-blocker, n (%) | 3(11.1) | 4(12.9) | 0.834 |
| Diuretic, n (%) | 2(7.4) | 2(6.5) | 0.886 |
| Second-degree AV block: Mobitz type II, n (%) | 2(7.4) | 3(9.7) | 0.759 |
| Third-degree (complete) AV block, n (%) | 25(92.6) | 28(90.3) | 0.759 |
| eGFR, mL/min/1.73 m2 | 71.03±11.51 | 69.80±15.71 | 0.738 |
| Serum Potassium, mEq/L | 4.07±0.52 | 3.95±0.42 | 0.342 |
| Serum Calcium, mg/dL | 9.05±0.61 | 9.16±0.41 | 0.429 |
| Serum Sodium, mEq/L | 138.55±2.76 | 139.06±3.01 | 0.508 |
| Hemoglobin, g/dL | 12.99±1.74 | 12.86±1.37 | 0.763 |
| Manufacturer (Medtronic), n (%) | 14(51.9) | 17(54.8) | 0.820 |
| Manufacturer (Biotronic), n (%) | 7(25.9) | 7(22.6) | 0.766 |
| Manufacturer (St. Jude), n (%) | 6(22.2) | 7(22.6) | 0.974 |
Abbreviations: n stands for Number; ACEi/ARB stands for Angiotensin-converting enzyme inhibitors/angiotensin receptor blockers; eGFR stands for estimated Glomerular Filtration Rate; AV stands for atrioventricular; BMI stands for Body Mass Index; Significance is denoted by bold font.
Paced QRS duration was significantly lower in the midseptal than apical pacing group after implant (141.83±25.90 vs 164.16±26.10 ms, respectively; p = 0.002). No significant difference was observed at baseline between the two groups regarding the capture threshold, R-wave amplitude, and lead impedance. During the follow-up visit after six months, these parameters remained comparable between the two pacing sites with no significant difference in the ventricular pacing percentage as shown in Table 2.
Table 2: Pacing Measurements at Baseline and 6 Months
| Parameters | Baseline | At 6 months | ||||
| RV Midseptal Pacing (n = 27) | RV Apical Pacing (n = 31) | P | RV Midseptal Pacing (n = 27) | RV Apical Pacing (n = 31) | p | |
| Paced QRS duration, ms | 141.83±25.90 | 164.16±26.10 | 0.002 | 147.53±19.74 | 169.18±24.56 | 0.001 |
| Capture threshold, mV | 0.75±0.25 | 0.69±0.24 | 0.334 | 0.60±0.31 | 0.55±0.32 | 0.608 |
| R-wave amplitude, V | 11.06±4.89 | 12.30±4.27 | 0.307 | 12.43±5.94 | 11.59±5.24 | 0.571 |
| Lead impendence, Ω | 931.77±239.17 | 875.41±260.87 | 0.397 | 979.92±280.49 | 886.48±259.41 | 0.193 |
| Ventricular pacing percentage, % | N/A | N/A | N/A | 82.35(12.40) | 86.99(13.32) | 0.178 |
Abbreviations: Ms stands for milliseconds, mV stands for millivolts, Ω stands for Ohms, Significance is denoted by bold font No significant clinical events, HF hospitalization, or mortality were observed.
Echocardiographic data taken shortly after pacemaker implantation did not show any statistically significant differences between the midseptal and apical pacing groups. The patients assigned to the midseptal pacing group have higher ejection fraction after six months of follow-up that are statistically significant (58.09±5.11 vs 54.52±5.76%, p = 0.016). Higher LVEDVi and LVESVi were observed in the apical than midseptal pacing group (p = 0.008 and 0.003, respectively). These results suggest that apical pacing was more likely to compromise LV function than midseptal pacing. The NT-proBNP levels and clinical characteristics at baseline were similar between the two groups. Serum NT-proBNP levels and the six-minute walk test distance significantly differed between the midseptal and apical pacing groups during the six months of follow-up. Nevertheless, EuroQol EQ-5D index and NYHA>1 show no statistical difference as shown in Table 3.
Table 3: Echocardiographic, Clinical, and Biologic Parameters at Baseline and 6 Months Followup
| Parameters | Baseline | At 6 months | ||||
| RV Midseptal Pacing (n=27) | RV Apical Pacing (n = 31) | p | RV Midseptal Pacing (n = 27) | RV Apical Pacing (n = 31) | p | |
| LV Ejection Fraction, % | 60.01±5.61 | 57.70±6.28 | 0.149 | 58.09±5.11 | 54.52±5.76 | 0.016 |
| LVEDVi, mL/m2 | 48.06±8.53 | 51.70±7.79 | 0.095 | 50.45±8.25 | 57.60±11.13 | 0.008 |
| LVESVi, mL/m2 | 17.46±3.40 | 18.61±2.70 | 0.160 | 18.81±3.46 | 22.05±4.40 | 0.003 |
| NT-proBNP, pg/mL | 669.80±612.82 | 703.02±593.53 | 0.835 | 339.28±263.94 | 607.86±377.54 | 0.003 |
| Six-minute Walk test distance, m | 303.54±184.97 | 278.18±165.32 | 0.584 | 462.76±115.48 | 382.12±153.81 | 0.030 |
| EuroQol EQ-5D index | 0.90±0.09 | 0.91±0.16 | 0.837 | 0.93±0.08 | 0.92±0.08 | 0.769 |
| NYHA>1, n (%) | N/A | N/A | N/A | 5(18.5) | 6(19.4) | 0.935 |
Abbreviations: LV stands for Left Ventricle, LVESVi stands for Left Ventricular End-Systolic Volume indexed to Body Surface Area, LVEDVi stands for Left Ventricular End-Diastolic Volume indexed to Body Surface Area, NYHA stands for New York Heart Association functional class; NT-proBNP stands for N-terminal -pro Brain Natriuretic Peptide, Significance is denoted by bold font
A comparison of echocardiographic parameters of the same group at baseline and 6 months follow-up was shown in Table 4.
Table 4: Echocardiographic Parameters at Baseline and 6 Months Follow-Up (Same Group Comparison)
| Parameters | RV Midseptal Pacing (n = 27) | RV Apical Pacing (n = 31) | ||||
| Baseline | At 6 months | P | Baseline | At 6 months | P | |
| LV Ejection Fraction, % | 60.01±5.61 | 58.09±5.11 | 0.199 | 57.70±6.28 | 54.52±5.76 | 0.069 |
| LVEDVi, mL/m2 | 48.06±8.53 | 50.45±8.25 | 0.232 | 51.70±7.79 | 57.60±11.13 | 0.026 |
| LVESVi, mL/m2 | 17.46±3.40 | 18.81±3.46 | 0.127 | 18.61±2.70 | 22.05±4.40 | 0.001 |
Abbreviations: LV stands for Left Ventricle, LVESVi stands for Left Ventricular End-Systolic Volume indexed to Body Surface Area; LVEDVi stands for Left Ventricular End-Diastolic Volume indexed to Body Surface Area, Significance is denoted by bold font
Until recently, actual RV midseptal pacing had been challenging to achieve consistently and accurately due to the posterior septal orientation and lack of appropriate standardized nomenclature and technique. Now, we have a clearer understanding of the RV chamber anatomy through the fluoroscopic appearances and electrocardiographic patterns which facilitate the true midseptal placement of active fixation leads. The current study found that midseptal pacing has no clinically significant differences from traditional RV apical pacing in terms of pacing threshold, R-wave sensing, or lead impedance. These pacemaker indices remained unchanged six months after pacemaker implantation and were consistent with earlier studies [7,26-33]. More importantly, the significantly shorter paced QRS duration with midseptal pacing produces more physiological pacing. Patients in the RV midseptal pacing group have a higher LV ejection fraction and six-minute walk test distance, lower LV volumes, and NT-proBNP levels than patients in the apical pacing group at the 6 months of follow-up. At least for the first six months following implantation, these advantages did not appear to be associated with an improvement in clinical outcomes of quality of life and NYAH functional class.
Historically, RV apicalpacing had been adopted due to the simplicity of lead fixation, low incidence of dislodgment, and a constant threshold value. Acute and prolonged RV apical pacing may worsen LV function and cause ventricular dyssynchrony as reported in earlier research [4,34]. It is also linked to higher rates of heart
failure hospitalization and worse long-term mortality, unlike the current study. A meta-analysis support these finding by finding that apical pacing causes a decline in LV function after one year of follow-up compared to nonapical pacing in patients who needed continuous RV pacing and had a baseline LV ejection fraction below 40% [35]. The advantages of pacing in sites near the conduction system as a means of reducing the detrimental effects of RV apical pacing have been examined in numerous small studies. One study found that midseptal pacing preserved LV ejection fraction in patients with LV dysfunction at baseline (ejection fraction < 45%) in contrast to apical pacing and confirmed the septal pacing safety and feasibility with its benefit of electrical resynchronization (shorter QRS and normalized QRS axis) [5]. Patients with RV apical pacing were found to have more dyssynchronization than the midseptal and control groups in a randomized single-blind prospective study [32]. Another study conclude that midseptal pacing produces more physiologic and synchronous pacing with RV midseptal pacing had a comparable operation time, no change in lead impedance or pacing threshold, and no lead dislodgement in comparison to apical pacing [36]. The present study findings are in line with these small studies. Not all leads will be implanted on the actual septal location using the standard fluoroscopic and electrocardiographic criteria. Many studies found the inadequacy of these methods and the importance of computed tomography as the gold standard [9-16]. As an example, in one study, only nine out of 35 (about one-fifth) of assumed “septal” leads were actually on the true septum using the traditional fluoroscopic criteria and those patients with lead in the true septum have narrower QRS complexes [15]. The current study also found a high failure rate with 36% (15/42) of the patients in the “intended” mid-septal group failed to implant the RV lead in the true mid-septal area as defined by CT scan. These are the rationale for confirming the lead tip position after implantation in the current study to find the real benefit of septal pacing as compared to other studies and emphasize the need to find a more accurate technique to implant the lead and confirm its position in real-time during the procedure. Shimerno et al., [11] describe specifically the midseptal in comparison to high and low septal pacing and found that it produces a narrower QRS complex with a description of the different ECG findings in these three groups.
The long-term impact ofthe apical and high septal pacing was compared in a study of 240 patients [31]. A total of 168 patients in this population had a 24-month follow-up, with RV pacing percentages of 98% and 93% in the apical and septal groups, respectively. In the apical and septal groups, the LV ejection fraction declined by 2 percent (from 57 percent to 55 percent and 56 percent to 54 percent, respectively) at 24 months of follow-up (p = 0.05). Unlike the current study, they found that septal pacing does not provide a protective effect on LV function over apical pacing in the first 24 months. In smaller research with a longer follow-up, they found that after 4 years of observation, RV septal pacing had no advantage over the apex in terms of LV function [37]. The authors did point out that a significant decrease in LV performance occurs when the RV lead is accidentally implanted anteriorly rather than at the septum which emphasizes the importance of true septal pacing as confirmed by computed tomography in the current study.
Furthermore, the current study assessed the effect of the lead location on physical function (Six-minute Walk test) and observed that it was better in the RV midseptal pacing as compared to apical pacing (p = 0.030). This finding was supplemented by the lower levels of NT-proBNP in the midseptal group at a 6-month follow-up (p = 0.003). Additionally, no significant difference in the prescription of medications was observed that may influence these findings. Nevertheless, the lead location did not impact NYHA>1 and the EuroQol EQ-5D quality of life index. These findings may be explained by the exclusion of patients with structural heart diseases and substantial co-morbidities in the current study. Finding clinical benefits may be more likely with a longer follow-up. In the PROTECT-PACE trial, different results were seen with no statistically significant difference in the six-minute walk test distance [31].
Finally, patients with apical pacing have a wider paced QRS as compared to those receiving a midseptal lead at baseline and 6-month follow-up (p = 0.002 and 0.001, respectively). This result is in line with a prior study showing that midseptal pacing resulted in considerably shorter QRS duration when compared to apical pacing (147 vs 154 ms, respectively) [38]. In the SEPTAL CRT Study, RV septal pacing was assessed after cardiac resynchronization therapy. At a 6-month follow-up, they found no difference in clinical outcomes between RV septal and apical pacing [39].
Study Limitations
The study was nonrandomized and represents a single-center experience despite having a prospective design. It did not show the deleterious impact of RV apical pacing on quality of life, NYAH>1, and HF hospitalization. The study period of 6 months may be inadequate to find a significant difference as earlier studies have found that LV ejection fraction may decline after 12 to 18 months [40,41]. Another reason is the smaller sample sizes in both groups, which may prevent reaching a statistical significance. Other echocardiography parameters that assess LV function, such as ventricular filling pressures and strain, were not evaluated. In fact, LV ejection fraction is not considered the best indicator of LV function and outcomes after interventions.
This study established the safety and reliability of medium-term RV midseptal pacing. Compared with RV apical pacing, midseptal pacing was associated with better LV ejection fraction and six-minute walk test, and lower LV volumes and NT-proBNP levels. In some cases, RV midseptal pacing might be a better option than regular RV apical pacing to lessen its negative effects.
Statista. “Pacemakers market volume worldwide in units 2023 Forecast.” 2022.
Delgado, V. et al. “acute effects of right ventricular apical pacing on left ventricular synchrony and mechanics.” Circulation: Arrhythmia and Electrophysiology, vol. 2, 2009, pp. 135–145.
Tops, L.F. et al. “Right ventricular pacing can induce ventricular dyssynchrony in patients with atrial fibrillation after atrioventricular node ablation.” Journal of the American College of Cardiology, vol. 48, 2006, pp. 1642–1648.
Nahlawi, M. et al. “Left ventricular function during and after right ventricular pacing.” Journal of the American College of Cardiology, vol. 44, 2004, pp. 1883–1888.
Victor, F. et al. “A randomized comparison of permanent septal versus apical right ventricular pacing: Short-term results.” Journal of Cardiovascular Electrophysiology, vol. 17, 2006, pp. 238–242.
Thambo, J-B. et al. “Detrimental ventricular remodeling in patients with congenital complete heart block and chronic right ventricular apical pacing.” Circulation, vol. 110, 2004, pp. 3766–3772.
Molina, L. et al. “Medium-term effects of septal and apical pacing in pacemaker-dependent patients: A double-blind prospective randomized study.” Pacing and Clinical Electrophysiology, vol. 37, 2014, pp. 207–214.
Shimony, A. et al. “Beneficial effects of right ventricular non-apical vs. apical pacing: A systematic review and meta-analysis.” EP Europace, vol. 14, 2012, pp. 81–91.
Chen, Y-L. et al. “Localization of right ventricular non-apical lead position: Comparison of three-dimensional echocardiography, ct, and fluoroscopy.” Journal of International Medical Research, vol. 49, 2021, pp. 300060521996159.
Shenthar, J. et al. “Computed tomography validated right ventricular mid-septal lead implantation using right ventricular angiography.” Journal of Arrhythmia, vol. 37, 2021, pp. 1131–1138.
Shimeno, K. et al. “Usefulness of right ventriculography to aid anchoring a pacing led to the right ventricular septum.” EP Europace, vol. 20, 2018, pp. 1154–1160.
Rowe, M.K. et al. “Surface ECG and fluoroscopy are not predictive of right ventricular septal lead position compared with cardiac CT.” Pacing and Clinical Electrophysiology, vol. 40, 2017, pp. 537–544.
Moore, P. et al. “Imaging and right ventricular pacing lead position: A comparison of CT, MRI, and echocardiography.” Pacing and Clinical Electrophysiology, vol. 39, 2016, pp. 382–392.
Sharma, G. et al. “Inadequacy of fluoroscopy and ECG in predicting septal position in RVOT pacing: Validation with cardiac CT.” Indian Heart Journal, vol. 68, 2016, pp. 174–180.
Pang, B.J. et al. “Validation of conventional fluoroscopic and ecg criteria for right ventricular pacemaker lead position using cardiac CT.” Pacing and Clinical Electrophysiology, vol. 37, 2014, pp. 495–504.
Osmancik, P. et al. “Usefulness of RAO projection for correct localization of ct-verified right ventricular mid-septal lead.” Circulation: Arrhythmia and Electrophysiology, vol. 6, 2013, pp. 719–725.
Kusumoto, F.M. et al. “2018 ACC/AHA/HRS Guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay.” Heart Rhythm, vol. 16, 2019, pp. e128–e226.
Andrikopoulos, G. et al. “Electrocardiographic algorithm for differentiating mid-septal vs. apical lead position: SPICE ECG substudy.” EP Europace, vol. 17, 2015, pp. 915–920.
Rosso, R. et al. “Right ventricular septal pacing: success of stylet-driven active-fixation leads.” Pacing and Clinical Electrophysiology, vol. 33, 2010, pp. 49–53.
Anderson, R.H. et al. “Cardiac anatomy revisited.” Journal of Anatomy, vol. 205, 2004, pp. 159–177.
Mond, H.G. et al. “The right ventricular outflow tract: The road to septal pacing.” Pacing and Clinical Electrophysiology, vol. 30, 2007, pp. 482–491.
Lang, R.M. et al. “Recommendations for Cardiac Chamber Quantification by Echocardiography.” Journal of the American Society of Echocardiography, vol. 28, 2015, pp. 1–39. e14.
EQ-5D Instruments. EuroQol Group, 2022.
Holland, A.E. et al. “Field walking tests in chronic respiratory disease: ERS/ATS technical standard.” European Respiratory Journal, vol. 44, 2014, pp. 1428–1446.
Inker, L.A. et al. “New creatinine- and cystatin c-based equations to estimate gfr without race.” New England Journal of Medicine, vol. 385, 2021, pp. 1737–1749.
Kypta, A. et al. “Long-term outcomes in av block patients with septal lead placement vs. apical pacing.” EP Europace, vol. 10, 2008, pp. 574–579.
Galand, V. et al. “SEPTAL-PM study: Septal vs. apical pacing in permanent rv pacing.” Archives of Cardiovascular Diseases, vol. 115, 2022, pp. 288–294.
Bansal, R. et al. “Incidence and predictors of pacemaker-induced cardiomyopathy: Apical vs. non-apical pacing.” Journal of Interventional Cardiac Electrophysiology, vol. 56, 2019, pp. 63–70.
Spath, N.B. et al. “Complications and prognosis of apical vs. septal rv pacing.” Open Heart, vol. 6, 2019, e000962.
Witt, C.M. et al. “RV lead position and long-term outcomes.” Journal of Cardiovascular Electrophysiology, vol. 28, 2017, pp. 924–930.
Kaye, G.C. et al. “Effect of RV lead site on LV function in high-grade AV block: Protect-pace study.” European Heart Journal, vol. 36, 2015, pp. 856–862.
Cano, O. et al. “RV septal vs. apical pacing effectiveness.” American Journal of Cardiology, vol. 105, 2010, pp. 1426–1432.
Bai, M. et al. “rv mid-septal vs. apical pacing: Randomized-controlled trial.” European Heart Journal Supplements, vol. 18, 2016, pp. F12–F18.
Auger, D. et al. “LV dyssynchrony induced by apical pacing: long-term effects.” Journal of Cardiovascular Electrophysiology, vol. 25, 2014, pp. 631–637.
Hussain, M.A. et al. “RV apical vs. non-apical pacing and lv ejection fraction.” Pacing and Clinical Electrophysiology, vol. 38, 2015, pp. 1121–1136.
Yusu, S. et al. “Selective mid-septal pacing: Follow-up of lead performance.” International Heart Journal, vol. 53, 2012, pp. 113–116.
Domenichini, G. et al. “Septal vs. apical pacing: Prospective randomized study.” European Journal of Internal Medicine, vol. 23, 2012, pp. 621–627.
Alhous, M.H.A. et al. “Temporary RV pacing from different sites and echocardiographic function indices.” EP Europace, vol. 13, 2011, pp. 1738–1746.
Leclercq, C. et al. “Septal vs. Apical Pacing in CRT-D Patients: SEPTAL-CRT Study.” European Heart Journal, vol. 37, 2016, pp. 473–483.
Hillock, R.J. and H.G. Mond. “Pacing the RVOT septum: Time to embrace the future.” EP Europace, vol. 14, 2012, pp. 28–35.
Tse, H-F. et al. “Functional abnormalities in permanent right ventricular pacing.” Journal of the American College of Cardiology, vol. 40, 2002, pp. 1451–1458.
