
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Background: Dermatoglyphics is the scientific study of epidermal ridges and their configurations on the palmar region of hand and fingers and plantar region of foot and toes. Dermatoglyphics as a diagnostic aid is now well established in a number of hereditary diseases. Against this genetic background of coronary artery disease (CAD), the study was undertaken to determine the correlation between dermatoglyphics and different group of CAD depending on number of coronary arteries involved due to atherosclerosis. Material and methods: The present study includes 150 patients of angiographically diagnosed coronary artery disease and 150 controls with normal healthy individuals. The palmar and finger prints of the patients and the controls were taken on the Map Litho White paper by ink method as described by Cummins and Midlo. Results: It is noted that there is significant decrease in loops with corresponding increase in whorls in single vessels disease (SVD) and triple vessels disease (TVD) with increase in the mean value of total and absolute finger ridge count in all groups of CAD. The true palmar pattern is significantly decrease in thenar area in double vessels disease (DVD) and ID3 area in SVD. There is significant increase in frequency of ‘4’ and ‘7’ palmar triradii in SVD and ‘5’ palmar triradii in DVD. Conclusions: It appears that there are characteristic dermatoglyphic patterns in different groups of CAD.
Dermatoglyphics is the scientific study of epidermal ridges and their configurations on the palmar region of hand and fingers and plantar region of foot and toes. The term dermatoglyphics was coined by Cummins and Midlo in 1926 and was derived from Greek words ‘derma’ means skin and ‘glyphics’ means carvings [1]. The ridge formation in the foetus begins at about three months of intrauterine life when the volar pads are at or near their peak development, and completed by sixth month of intrauterine life, when the sweat gland formation and keratinization have began [2]. The original ridge characteristics are not disturbed unless the skin is damaged to a depth of about one millimetre [3].
Development of dermatoglyphic pattern is under genetic control. This is evident from the clear resemblance of dermatoglyphics among related person [4]. There are many diseases known to be caused by abnormal genes. Whenever there is any abnormality in the genetic make-up of parents it is inherited to the children and is reflected in dermatoglyphic pattern [5]. Cummins H [6] professor of Anatomy at Turan University was the first person to show the possible use of dermatoglyphics in clinical medicine while dealing with mongolism cases.
Dermatoglyphics as a diagnostic aid is now well established in a number of diseases, which have a strong hereditary basis, and is employed as a method of screening abnormal anomalies [7].
Apart from its use in predicting the diagnosis of genetic disease, dermatoglyphics is also used in forensic science for individual identification. It is also a valuable research tool in the field of Physical Anthropology, Human Genetics and Medicine [8]. Sir Herschel WJ [9] Chief Magistrate of Hooghly district in Bengal, India was the first to use finger print identification against impersonation. The research findings put forth by some scientists suggest that muzzle prints of animals similar to fingerprints in human being could be used as permanent method of identification of such animal to check fraud particularly in insurance matter [10]. Dermatoglyphics patterns were also used for fortune telling in accordance with the number of loops and whorls on fingers [11].
Coronary artery disease is a prevalent heart condition characterised by development of atherosclerosis in the coronary arteries. The atherosclerotic lesions in coronary arteries are distributed in one or more of the three major coronary arterial trunks, the highest incidence being in left anterior descending artery (LAD), followed by right coronary artery (RCA) and left circumflex artery (LCX) [12]. Kumar V et al. [13] also described that although only a single major coronary epicardial trunk may be affected, two or all three – LAD, LCX, and RCA are often involved. Clinically significant stenosing plaques may be located anywhere within these vessels but tend to predominate within the first several centimetres of LAD and LCX and along the entire length of the RCA.
Autopsy in individuals who died of non-cardiac causes revealed a high prevalence of SVD up to 10% [14]. The frequency of TVD is more common in Asian Indians as compared to Europeans, which suggests that severity of LAD is greater in Asian Indians [15]. Enbergs A et al. [16] studied 331 patients in whom the underlying disease was not related to CAD and found a prevalence of CAD in 7.3% cases with SVD in 3.6%, DVD in 2.1% and TVD in 1.6% with at least one critical stenosis greater than 50% lumen.
Coronary Artery Disease (CAD) is the leading single cause of death and loss of Disability Adjusted Life Years (DALYs) globally. It was responsible for 8.9 million deaths and 164.0 million DALYs globally in 2015 [17]. There were 315 million prevalent cases of CAD globally in 2022 [18]. About 1.5 million individuals in the US suffer an acute myocardial infarction annually and approximately one third of them die. At least 250,000 people a year die of a heart attack before they reach the hospital [13]. CAD is the leading cause of cardiovascular mortality worldwide, with >4.5 million deaths occurring in the developing world [19]. In India, cardio-vascular diseases accounted for 31% of all deaths in 2021, making it the leading cause of mortality in the country according to sample registration survey report published by Registrar General of India [20]. The aetiology of Coronary Artery Disease (CAD) is multifactorial with genetics playing an important role. Taking into consideration of genetic predisposition of dermatoglyphics and coronary artery disease, the study was undertaken to find out correlation between different groups of CAD with dermatoglyphic patterns.
The present study includes 150 patients of angiographically diagnosed coronary artery disease and 150 controls with age ranges between 31 years to 75 years. It was carried out in the Department of Anatomy from July 2007 to August 2009 at NKP Salve Institute of Medical Sciences, Nagpur. The cases were divided into three different groups depending on the involvement of number of coronary arteries as single vessel disease (SVD), double vessels disease (DVD) and triple vessels disease (TVD). There were 120 males and 30 females in cases and controls.
The palmar and finger prints of the patients and the controls were taken on the Map Litho White paper by ink method as described by Cummins and Midlo [6] Kores Camel duplicating ink was spread over plain glass slab of size 12”x8” with the help of a spreading roller. Both hands were first washed with soap and water followed by soaking. Then, the palm and fingers were placed on the inking glass slab. The smeared/ inked palm and fingers of both hands were then kept on the white paper with firm pressure on the dorsum of hand and interdigital area [8]. The dermatoglyphic patterns were thus recorded and parameters like finger tip pattern, true palmar pattern, number of palmar triradii, atd angle and ab ridge count were studied. The dermatoglyphic patterns on both hands were analysed and subjected to statistical test to evaluate the pattern. The statistical evaluation was done by chi square method and t-test (Figure 1).
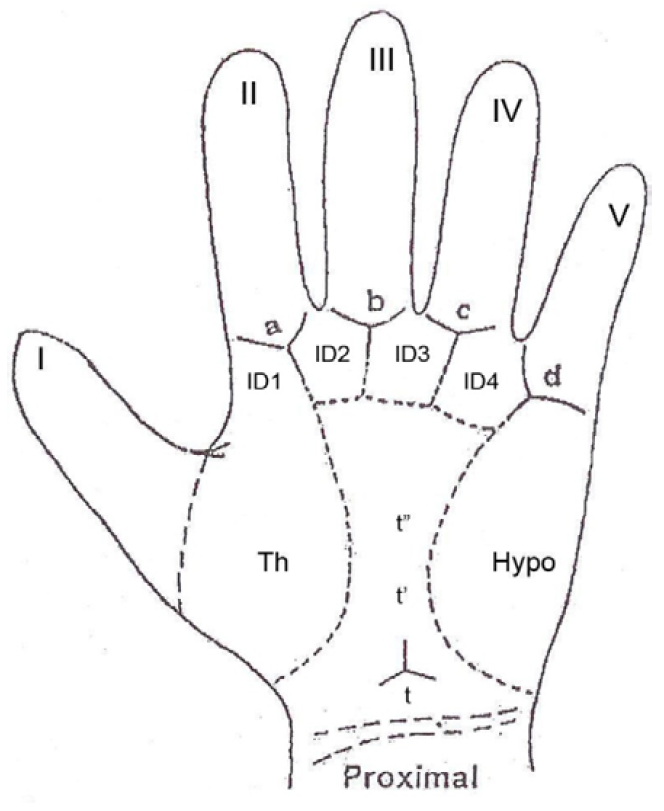
Figure 1: Showing Palmar Pattern Configuration and Palmar Areas with Palmar Triradii
The dermatoglyphic patterns of CAD patients are analysed depending on the number of coronary arteries involved and are subjected to statistical tests to evaluate significant pattern of identifiable difference between different groups of CAD and controls.
Different Groups of CAD
Table 1 show that 35.3% of the patients have single vessel involvement (SVD), 27.3% of cases have double vessels involvement (DVD), and 37.3% have three vessels involvement (TVD).
Table 1: Distribution of Different Groups Depending on the Number of Coronary Arteries Involved in CAD Cases
| No of vessels involved | Male | Female | Total | |||
No | % | No | % | No | % | |
SVD | 41 | 34.2 | 12 | 40.0 | 53 | 35.3 |
DVD | 34 | 28.3 | 7 | 23.3 | 41 | 27.3 |
TVD | 45 | 37.5 | 11 | 36.7 | 56 | 37.3 |
TOTAL | 120 | 80.0 | 30 | 20.0 | 150 | 100.0 |
Finger Tip Patterns (FTP)
Qualitative analysis of Finger Tips is done according to Galton’s [21]. Classification.
As per Table 2, the maximum percentage of loops is seen in DVD. Most numbers of arches are seen in SVD and whorls in TVD.
In SVD, there is significant decrease in the percentage of loop pattern (P<0.001) and increase in whorl patterns (p<0.001) as compared to the controls.
In DVD, there is slight increase in the percentage of loop and whorl pattern and decrease in arch pattern as compared to the controls but not statistically significant.
In TVD, there is significant decrease in the percentage of loop pattern (P<0.01) and increase in whorl patterns (P<0.0001) as compared to the controls.
Thus, in SVD and TVD group, there is statistically significant decrease in loop and corresponding increase in whorl patterns as compared to the control.
Table 2: Statistical Comparison of Total Finger Tip Pattern between different groups of CAD with Controls
| Groups of | FINGER TIP PATTERNS | ||
| CAD | LOOPS | ARCHES | WHORLS |
| CONTROLS | 870 | 124 | 506 |
| % | 58.0 | 8.3 | 33.7 |
| SVD | 257 | 44 | 229 |
| % | 48.5 | 8.3 | 43.2 |
| Chi Sq | 13.96 | 0.00 | 14.81 |
| P-Value | 0.0001869 | 0.9470546 | 0.0001188 |
| Remark | S | NS | S |
| DVD | 243 | 24 | 143 |
| % | 59.3 | 5.9 | 34.9 |
| Chi Sq | 0.16 | 2.30 | 0.14 |
| P-Value | 0.6854632 | 0.1297030 | 0.7077705 |
| Remark | NS | NS | NS |
| TVD | 279 | 34 | 247 |
| % | 49.8 | 6.1 | 44.1 |
| Chi Sq | 10.73 | 2.47 | 18.48 |
| P-Value | 0.0010549 | 0.1157774 | 0.0000172 |
| Remark | S | NS | S |
(S= Significant; NS= Non-significant)
Ridge Count of Finger Patterns
Holt SB (1961)7 stated that the ridge counts, which are size related numerical representatives of pattern types are considered to be of greatest significance in genetic terms.
Total Finger Ridge Count (TFRC): It represents the sum of ridge counts of all ten digits, where only the larger count is used on those digits with more than one ridge count. It expresses the size of pattern
Absolute Finger Ridge Count (AFRC): It is the sum of the ridge counts from all the separate triradii on the fingers. It reflects the pattern size as well as pattern intensity, which depends on the pattern type
Table 3 shows statistical calculation of TFRC in different Groups of CAD and controls. There is increase in the mean value of TFRC in all groups of CAD as compared to the controls, but not statistically significant.
Table 3: Statistical Calculation of TFRC count in different Groups of CAD and Controls
| Groups | TFRC | ||||||
| Mean | SD | SE-M | CV | t-value | P value | Remarks | |
| Controls | 142.00 | 46.85 | 3.83 | 32.99 | |||
| SVD | 147.64 | 44.77 | 6.15 | 30.33 | 0.762 | 0.447 | NS |
| DVD | 147.76 | 39.24 | 6.13 | 26.56 | 0.721 | 0.472 | NS |
| TVD | 151.71 | 42.33 | 5.66 | 27.90 | 1.358 | 0.176 | NS |
Table 4 shows statistical calculation of AFRC in different Groups of CAD and controls. There is increase in the mean value of AFRC in all groups of CAD as compared to the controls, but not statistically significant except TVD (p<0.05).
Table 4: Statistical Calculation of AFRC count in Different Groups of CAD and Controls
| Groups | AFRC | ||||||
| Mean | SD | SE-M | CV | t-value | P value | Remarks | |
| Controls | 184.68 | 83.58 | 6.82 | 45.25 | |||
| SVD | 196.58 | 83.05 | 11.41 | 42.25 | 1.972 | 0.373 | NS |
| DVD | 190.39 | 76.69 | 11.98 | 40.28 | 1.973 | 0.694 | NS |
| TVD | 205.93 | 78.44 | 10.48 | 38.09 | 1.972 | 0.049 | S |
Palmar Patterns
Galton F [2]1 classified quantitative categories of total true palmar pattern in different areas of palm. The palm has been divided into several anatomically well divided areas to carry out dermatoglyphic analysis. These include thenar, interdigital areas-ID1, ID2, ID3, ID4 and hypothenar areas. The quantitative pattern types are subjected to chi-square test.
As per Table 5, the total percentage of true palmar patterns is 39.8%, 37.2% and 38.1% in SVD, DVD and TVD respectively. In all groups, palmar patterns are predominantly seen in hypothenar area followed by ID4 area and ID3 area.
Table 5: Statistical Comparison of true Palmar Pattern between Different Groups of CAD with Controls
| Groups | TRUE PALMAR PATTERNS IN DIFFERENT AREAS | Sum | |||||
| of CAD | HYPO | THENAR | ID-1 | ID-2 | ID-3 | ID-4 | Total |
| Controls | 254 | 132 | 14 | 17 | 153 | 173 | 743 |
| % | 84.7 | 44.0 | 4.7 | 5.7 | 51.0 | 57.7 | 41.3 |
| SVD | 92 | 46 | 7 | 9 | 39 | 60 | 253 |
| % | 86.8 | 43.4 | 6.6 | 8.5 | 36.8 | 56.6 | 39.8 |
| Chi Sq | 0.14 | 0.01 | 0.27 | 0.62 | 5.79 | 0.01 | 0.38 |
| P-Value | 0.7106865 | 0.9142420 | 0.6037673 | 0.4294973 | 0.0161583 | 0.9394374 | 0.5394859 |
| Remark | NS | NS | NS | NS | S | NS | NS |
| DVD | 73 | 25 | 1 | 8 | 38 | 38 | 183 |
| % | 89.0 | 30.5 | 1.2 | 9.8 | 46.3 | 46.3 | 37.2 |
| Chi Sq | 0.67 | 4.31 | 1.22 | 1.16 | 0.39 | 2.9 | 2.51 |
| P-Value | 0.4130006 | 0.0377808 | 0.2085598 | 0.2823646 | 0.5332411 | 0.0886800 | 0.1132812 |
| Remark | NS | S | NS | NS | NS | NS | NS |
| TVD | 91 | 45 | 6 | 7 | 49 | 58 | 256 |
| % | 81.3 | 40.2 | 5.4 | 6.3 | 43.8 | 51.8 | 38.1 |
| Chi Sq | 0.47 | 0.34 | 0.08/ 0.00 | 0.00 | 1.44 | 0.92 | 1.93 |
| P-Value | 0.4926545 | 0.5583472 | 0.9740607 | 0.9908444 | 0.2305501 | 0.3377942 | 0.1649691 |
| Remark | NS | NS | NS | NS | NS | NS | NS |
In SVD and TVD groups of CAD, there is increase percentage of true palmar pattern in ID-1 and ID-2 but not statistically significant. In DVD group, there is increase percentage of true palmar pattern in hypothenar and ID-2 area but not statistically significant. The true palmar patterns are decreased in thenar, ID-3 and ID-4 area in all groups of CAD with statistically significant decrease in ID-3 area (<0.05) in SVD group and thenar area (<0.05) in DVD group.
Number of Palmar Triradii
Table 6 shows statistical comparison of different groups of CAD with the controls.
In SVD, there is increase in the percentage of ‘4’ and ‘7’ palmar triradii and decrease in the percentage of ‘5’ and ‘6’ palmar triradii as compared to the controls with statistically significant difference is seen in ‘4’ palmar triradii (p<0.0001) and ‘7’ palmar triradii (p<0.01).
In DVD, there is increase in the percentage of ‘4’, and ‘5’ palmar triradii and decrease in the percentage of ‘6’ palmar triradii as compared to the controls with statistically significant difference is seen in ‘5’ palmar triradii (P<0.01) and ‘6’ palmar triradii (p<0.001).
In TVD, there is increase in the percentage of ‘4’, ‘5’ and ‘7’ palmar triradii and decrease in the percentage of ‘6’ palmar triradii as compared to the controls with statistically significant difference is seen in ‘6’ palmar triradii (p<0.01).
Table 6: Statistical Comparison of Number of Palmar Triradii between Different Groups of CAD with Controls
| Groups | NUMBER OF PALMAR TRIRADII | |||||
| of CAD | 4 | 5 | 6 | 7 | 8 | 9 |
| Controls | 4 | 167 | 104 | 17 | 6 | 2 |
| % | 1.3 | 55.7 | 34.7 | 5.7 | 2.0 | 0.7 |
| SVD | 11 | 49 | 30 | 15 | 1 | 0 |
| % | 10.4 | 46.2 | 28.3 | 14.2 | 0.9 | 0.0 |
| Chi Sq | 15.55 | 2.44 | 1.16 | 6.64 | 0.08 | 0.0 |
| P-Value | 0.0000802 | 0.1184849 | 0.2811403 | 0.0099671 | 0.7761360 | 0.9714613 |
| Remark | S | NS | NS | S | NS | NS |
| DVD | 3 | 62 | 12 | 3 | 2 | 0 |
| % | 3.7 | 75.6 | 14.6 | 3.7 | 2.4 | 0.0 |
| Chi Sq | 0.86 | 9.85 | 11.29 | 0.2 | 0.04 | 0.01 |
| P-Value | 0.354099 | 0.0016956 | 0.0007782 | 0.6572240 | 0.8500247 | 0.9028631 |
| Remark | NS | S | S | NS | NS | NS |
| TVD | 5 | 72 | 22 | 10 | 3 | 0 |
| % | 4.5 | 64.3 | 19.6 | 8.9 | 2.7 | 0.0 |
| Chi Sq | 2.42 | 2.15 | 7.98 | 0.93 | 0.00 | 0.00 |
| P-Value | 0.119822 | 0.1429470 | 0.0047360 | 0.3337330 | 0.9677337 | 0.9445075 |
| Remark | NS | NS | S | NS | NS | NS |
ab Ridge Count
Table 07 shows that the mean value of ab ridge count in different groups of CAD is slightly lower as compared to the controls and not statistically significant in any group of CAD.
Table 7: Statistical Calculation of ab-ridge count in different Groups of CAD and Controls
| Groups | MEAN | SD | SE-M | CV | t-value | p-value | Remark |
| Controls | 40.09 | 5.24 | 0.42 | 13.08 | - | - | - |
| SVD | 39.72 | 4.81 | 0.66 | 12.12 | 0.445 | 0.668 | NS |
| DVD | 39.93 | 5.08 | 0.79 | 12.73 | 0.174 | 0.862 | NS |
| TVD | 39.91 | 5.38 | 0.73 | 13.51 | 0.205 | 0.839 | NS |
atd Angle
Table 08 shows that the mean value of atd angle in all groups of CAD is higher as compared to the controls, and it is statistically significant in DVD group (p<0.05) and TVD group (p< 0.05).
Table 8: Statistical Calculation of atd Angle in Different Groups of CAD and Controls
| Groups | MEAN | SD | SE-M | CV | t-value | P value | Remarks |
| Controls | 39.78 | 4.22 | 0.34 | 10.61 | - | - | - |
| SVD | 40.33 | 4.84 | 0.66 | 11.99 | 0.761 | 0.504 | NS |
| DVD | 41.34 | 5.37 | 0.84 | 12.99 | 1.982 | 0.044 | S |
| TVD | 41.41 | 4.81 | 0.64 | 11.64 | 2.361 | 0.020 | S |
The angiographically diagnosed CAD patients were classified into three groups as SVD, DVD, TVD depending on the number of vessels involved due to atherosclerosis, and it is found that 35.3% of the patients have SVD, 27.3% have DVD and 37.3% have TVD. This finding is similar to Harsh Mohan [12]. About one third of cases of CAD have single vessel disease (SVD), most often LAD arterial involvement; another one third have two vessels disease (DVD), and the remainder have three major vessels disease (TVD) [12]. Fischer et al. [22] noticed SVD in 23.1%, DVD in 33.1% and TVD in 40.3% cases to an extent of >50% stenosis due to atherosclerotic lesion.
Among patients with unstable angina who undergo coronary angiography, ~25% will have one vessel, 25% have two vessels and 25% have three vessels involvement, 10% will have significant left main stenosis and the other 15% will have narrowing of less than 50% or normal vessel on angiography [23].
Finger Tip Pattern
In the present study, there is significant decrease in the percentage of loops in SVD (p< 0.001) and TVD (p< 0.01) with slight increase in DVD when compared to the controls. Whereas, there is significant increase in the percentage of whorls in SVD (p<0.001) and TVD (p<0.0001) when compared to the controls. There is slight decrease in the arches in DVD, but not statistically significant.
Rashad and Mi [24] reported significantly lower frequency of ulnar loops and higher frequency of whorls in myocardial infarction (MI) patients. Rashad et al. [25] observed less frequency of ulnar loops and tented arches with higher frequency of true whorls in MI patients. Anderson MW et al. [26] found decrease loop pattern and increase whorl pattern in MI but not statistically significant difference when compared with the controls. Bhatt [27] revealed lower incidence of loops and higher incidence of whorls in MI. Dhall et al. [28] observed significantly lower loop pattern and higher whorls pattern in MI patients as compared to the control group (p<0.001); whereas, the arches were decreased but not statistically significant. Jalali et al. [29] also revealed significant decrease in loops and increase in whorls pattern in MI; whereas, the arches were significantly increase by roughly two times in MI patients as compared to the controls. Chimne et al [8] noted decrease in loops and increase in whorls pattern in MI. Thus the finding of decreased frequency of loops and increased frequency of whorls in the present study coincides with the finding of above workers. However, Shamsadini S et al. [30] reported significant increase in the frequency of loops in MI patients (p<0.001).
Significant decrease percentage of loops in SVD and TVD, decrease percentage of arches in DVD and TVD, and significant increase percentage of whorls in all groups of CAD could not be compared as none of the workers had classified CAD into SVD, DVD and TVD for dermatoglyphic study. Moreover, the frequency of loops is higher in DVD, arches in SVD and whorls in TVD in contrast to other groups of CAD.
Ridge Count of Finger Print
In the present study there is increase in the mean value of TFRC and AFRC in all groups of CAD as compared to the controls with statistically significant increase of AFRC in TVD group (p<0.05). Rashad and Mi [24] and Arun Kumar et al, [31] observed significant increase in TFRC and AFRC in myocardial infarction patients. Rashad et al. [25] also reported significant increase in TFRC and AFRC in MI patients. Anderson MW et al. [26] observed no statistically significant increase in TFRC and AFRC in MI patients. In contrast to this above findings, Reenu Kumari et al [32] reported significant decrease in TFRC and AFRC in MI patients.
However, increase mean value of TFRC and AFRC in all groups of CAD could not be compared as none have classified and studied different groups of CAD for dermatoglyphics.
Palmar Patterns in Different Palmar Areas
In the present study, palmar patterns are predominantly seen in hypothenar area followed by ID4 and ID3 area in all groups of CAD and controls. In SVD, there is decrease in the percentage of true palmar pattern in all areas except hypothenar and ID1 area with statistical significant decrease in ID3 area (p<0.05). In DVD, there is decrease in the percentage of true palmar pattern in all areas except hypothenar and ID2 area with statistical significant decrease in thenar area (p<0.05). In TVD, there is decrease in the percentage of true palmar pattern in all areas except ID1 and ID2 area but not statistically significant in any areas.
No previous workers has carried out the study on palmar pattern in different groups of CAD, hence the present study findings could not be compared. However, Takashina and Yorifuji [33] observed significant increases in the loop pattern in hypothenar area in acquired heart disease (33%) as compared to the congenital heart disease (21%).
Total Number of Palmar Triradii
In the present study, there is increase in the percentage of ‘4’ and ‘7’ palmar Triradii in SVD; ‘4’ and ‘5’ palmar triradii in DVD and ‘4’, ‘5’ and ‘7’ palmar triradii in TVD with significant increase in ‘4’ palmar triradii (p<0.0001) and ‘7’ palmar triradii (p<0.01) in SVD; and ‘5’ palmar triradii in DVD (p<0.01). Also, there is decrease in the percentage of ‘5’ and ‘6’ palmar triradii in SVD and ‘6’ palmar triradii in DVD and TVD with significant decrease in ‘6’ palmar triradii in DVD (p<0.001) and TVD (p<0.01).
No study has been carried out previously on number of palmar Triradii in different groups of CAD, hence present study findings could not be compared.
ab Ridge Count
In the present study, the mean value of ab ridge count in different groups of CAD is slightly lesser as compared to the controls but not significant.
This present study findings could not be compared as no previous study has been carried out on ab ridge count in different groups of CAD.
atd Angle
In the present study, the mean value of atd angle in all groups of CAD is increased as compared to the controls with significant increase in DVD (P<0.05) and TVD (P<0.05) group of CAD.
No study has been carried out on atd angle in different groups of CAD, hence present study findings could not be compared.
In the present study, it is concluded that:
Penros, L.S. “Finger prints, palms and chromosomes.” Nature, vol. 197, 1963, pp. 933–938.
Babler, J.W. “Prenatal selection and dermatoglyphic patterns.” American Journal of Physical Anthropology, vol. 46, 1978, pp. 21–25.
Cummins, H. and Midlo. “Finger prints of palms and soles: an introduction to dermatoglyphics.” Dover Publications Inc., New York, 1943.
Schaumann and Alter. “Dermatoglyphics in medical disorders.” Springer Verlag, New York, 1976, pp. 187–189.
Walker, J.F.A. “Sex linked recessive finger print pattern.” Journal of Heredity, vol. 32, 1964, pp. 279–280.
Cummins, H. “Dermatoglyphics stigmata in mongolism.” Anatomical Record, vol. 64, 1936, pp. 11.
Holt, S.B. “Dermatoglyphic patterns.” In Genetical variation in human population, Oxford, Pergamon, 1961, pp. 791.
Chimne, H.D. and Ksheersagar, D.D. “Dermatoglyphic patterns in angiographically proven coronary artery disease.” Journal of Anatomical Society of India, vol. 61, no. 2, 2012, pp. 262–268.
Hershel, W.J. “The encyclopedia of palmistry.” Berkley Publishing Group, New York, 1996, pp. 98–124.
Tarasiuk, S.I. et al. “The muzzle prints and biochemical genetic markers as supplementary breed characteristics in cattle.” 1997, vol. 31, no. 4, pp. 89.
Ambade, H.V. and Ambade, V.N. “Fingerprint pattern in myocardial: does the fate of heart lies in fingertips?” Journal of Forensic Medicine and Toxicology, vol. 31, no. 2, 2014, pp. 45–49.
Harsh Mohan. “Textbook of pathology.” 5th ed., Jaypee Publishers, New Delhi, 2006, pp. 316–326.
Kumar, V. et al. “Robbins and Cotran pathologic basis of disease.” 7th ed., Saunders Elsevier Publication, Philadelphia, 2007, pp. 571–587.
Davies, M.J. “Anatomic features in victims of sudden death: coronary artery pathology.” Circulation, vol. 85, 1992, pp. 19–24.
Premlatha, G. and Mohan, V. “Hyperinsulinaemia, diabetes and coronary heart disease in India.” International Journal of Diabetes in Developing Countries, vol. 15, 1995, pp. 85–86.
Enbergs, A. et al. “Prevalence of coronary artery disease in a general population without suspicion of coronary artery disease: angiographic analysis of subjects aged 40–70 years referred for catheter ablation therapy.” European Heart Journal, vol. 21, 2000, pp. 45–52.
Ralapanawa, U. and Sivakanesan, R. “Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review.” Journal of Epidemiology and Global Health, vol. 11, no. 2, 2021, pp. 169–177.
Stark, B. et al. “Global prevalence of coronary artery disease: an update from the global burden of disease study.” Journal of the American College of Cardiology, vol. 83, no. 13, 2024, pp. 216.
Okrainec, K. et al. “Coronary artery disease in the developing world.” American Heart Journal, vol. 148, no. 1, 2004, pp. 7–15.
Registrar General of India. “Sample registration survey report on causes of death: 2021–23.” The Indian Practitioner, 2025.
Galton, F. “Fingerprints.” Macmillan, London, 1892.
Fischer, M. et al. “Distinct heritable patterns of angiographic coronary artery disease in families with myocardial infarction.” Circulation, vol. 111, 2005, pp. 855–862.
Fuster, V. et al. “Hurst’s the heart.” 10th ed., McGraw Hill Medical Publishing Division, 2001, pp. 1065–1537.
Rashad, M.N. and Mi, M.P. “Dermatoglyphic traits in patients with cardiovascular disorders.” American Journal of Physical Anthropology, vol. 42, no. 2, 1975, pp. 281–283.
Rashad, M.N. et al. “Dermatoglyphic studies of myocardial infarction patients.” Human Heredity, vol. 28, 1978, pp. 1–6.
Anderson, M.W. et al. “Dermatoglyphic features of myocardial infarction patients.” American Journal of Physical Anthropology, vol. 55, no. 4, 1981, pp. 523–527.
Bhatt, S.H. “New sign of myocardial infarction.” Medicine Update, 1996, pp. 411–416.
Dhall, V. et al. “Utility of finger prints in myocardial infarction patients.” Journal of Anatomical Society of India, vol. 49, no. 2, 2000, pp. 153–154.
Jalali, F. and Hajian-Tilaki, K.O. “A comparative study of dermatoglyphic pattern in patients with myocardial infarction and control group.” Acta Medica Iranica, vol. 40, no. 3, 2002, pp. 187–191.
Shamsadini, S. et al. “Relationship between fingerprint dermatoglyphics in association with susceptibility to myocardial infarction in man.” Journal of Kerman University of Medical Sciences, vol. 4, no. 3, 1997, pp. 136–143.
Arun Kumar, K.R. et al. “A study on dermatoglyphics pattern of patients with myocardial infarction.” International Journal of Anatomy Research, vol. 9, 2021, pp. 8160–8167.
Reenu Kumari et al. “A study on fingertip dermatoglyphic pattern in patients with myocardial infarction in north Indian population.” Asian Journal of Pharmaceutical and Clinical Research, vol. 17, no. 2, 2024, pp. 69–71.
Takashina, T. and Yorifuji, S. “Palmar dermatoglyphics in heart disease: differential studies in Japanese and American populations with congenital and acquired heart diseases.” JAMA, vol. 197, no. 9, 1966, pp. 689–692.
