
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Background: Pain after open “Morgan-Milligan” hemorrhoidectomy is a significant problem both for the patient and the surgeon. It increases analgesics need, prolongs the hospital stay, delay first act, hindered early return to usual daily activities and causes a significant anxiety to the patient and family. Aim of the Study: To evaluate effectiveness of oral Metronidazole therapy in the decreasing pain after open hemorrhoidectomy. Patients and Methods: A prospective controlled study was set in the Department of Surgery/Al-Yarmouk Teaching Hospital. The study included adult patients who undergone elective opened “Morgan-Milligan” hemorrhoidectomy for grade III and IV disease. Data collection was completed over the period from the 1st of June 2017 to 15th of January 2019. The total number of patients after exclusion was 64 patients (32 patients in each group). Patients who are discharged in the first operative day were allocated in to two groups; those who received oral Metronidazole course (group A; study group) and those who did not received the therapy (group B; control group). The main parameter studied was pain. Other parameters include frequency of analgesic doses required, time for first bowel motion, time for return for usual daily activities and evidences of Surgical Site Infection. The method for pain assessment was Visual Analogue Scale (VAS) of 10 grades. A scale sheet was supplied for each patient (in native language) and patients were informed clearly how to fill the required information. At the end of the first week, the attendance of the patients and delivery of the VAS sheet is considered the date for termination of assessment. Patients who are lost to follow up or discontinued therapy due to drug intolerance, were excluded from analysis. Data tabulated and appropriately displayed and statistically analyzed using Statistical Package for Social Sciences (SPSS) version 25. A P-Value less than 0.05 was considered significant. Ethical aspects and official approval were appropriately considered. Results: The overall age range was 18 - 55 years (a mean of 32.37 years and a standard deviation of±10.06 years). Female gender predominates in both groups (22 in group A, 18 in group B). The majority in both group A and B have Grade III hemorrhoid (81.3% and 87.5% respectively). There were no statistically significant differences between the two groups regarding age and gender. Postoperatively, the mean of VAS in the 1st, 3rd, 7th day, and on the 1st bowel motion was significantly lower in group A patients compared to those in Group B (5.46 versus 6.71, p = 0.011; 5.31 versus 7.81, p = 0.001; 4.46 versus 6.25, P = 0.001; and 4.06 versus 6.56, p = 0.001; respectively). There was no statistically significant difference (p = 0.104) between study groups in mean of VAS in the 2nd day. The mean of doses of analgesia required in the 1st, 3rd, 7th day, and on the 1st bowel motion was significantly lower in group A patients compared to those in Group B (2.75 versus 3.37, p = 0.001; 2.75 versus 3.37, p = 0.002; 2.37 versus 3, p = 0.016; and 3.43 versus 3.93, p = 0.001; respectively). Again; no statistically significant difference (p = 0.162) between study groups regarding mean doses of analgesia on the 2nd day. No statistically significant difference (p = 0.11) was reported between study groups regarding mean time for 1st bowel motion. Returning to usual daily activities was significantly earlier in group A patients compared with patients in Group B (5.68 versus 7.12 days, p = 0.028). At the end of first week; a total of 7 (11%) patients demonstrated signs of Surgical Site Infection. This was statistically insignificant when compared between both groups (p = 0.229). Conclusion: There are evidences that oral Metronidazole therapy after open hemorrhoidectomy can play a role in reduction of pain intensity.
Hemorrhoids occur when the venous drainage of the anus is altered, causing the venous plexus and connecting tissue to dilate, creating an outgrowth of anal mucosa from the rectal wall [1]. Hemorrhoids are classified as internal or external based on their location relative to the dentate line. Goligher’s classification of hemorrhoid include:
Goligher’s classification of hemorrhoid [2]:
Hemorrhoids are more prevalent in persons 45 to 65 years of age [3]. Both sexes experience about the same incidence of the condition. They are more common in Caucasians and those of higher socioeconomic status [4]. Typical symptoms include: Bleeding commonly in grade I and II, Prolapse, Pain: severe pain is unusual unless associated with acutely prolapsed thrombosed hemorrhoids, Soiling and Pruritus [5]. Hemorrhoid may be treated with conservative measures (change life style, medical treatment (e.g.: Nonsteroidal anti-inflammatory drugs)), Non operative measures (Submucosal seclerosant injection [6], Rubber band ligation [7] and Infrared coagulation [8]) or treated with surgical intervention via hemorrhoiectomty in which the major drawback of it is the postoperative pain [9]. Postoperative pain requires opiate use, prolongs the hospital stay, and affects the patient’s comfort [10].
Post-hemorrhoidectomy pain is explained in many aspects. It may be caused by [11]:
Post-operative spasm of the internal anal sphincter which can be decreased by lateral anal sphincterotomy
Manipulation of the sensitive mucosa distal to the dentate line results in painful symptoms as a result of activating the stretch and somatic pain receptors
Pain from tissue inflammation resulting from bacterial infiltration of the wound. Most of these species of bacteria are nonpathogenic commensal organisms that are harmless as long as they stay in the gut lumen
Poor and delayed wound healing will lead to epithelial denudation
Incarceration of smooth muscle fibers and mucosa in the transfixed pedicle
Thrombosis of residual hemorrhoidal tissue, application of staples closes to the anal verge, or incorporation of the rectal nerve/muscle in the suture [12]
Metronidazole is an effective antibiotic against anaerobic bacteria. It diminishes surgical site inflammation by reducing the rate of bacterial colonization and infection of hemorrhoidectomy wounds. The current study aimed to evaluate the effectiveness of oral Metronidazole therapy on post open hemorrhoidectomy pain relief.
Patients and Methods: A prospective controlled study was set in the Department of Surgery/Al-Yarmouk Teaching Hospital over the period from the 1st of June 2017 to 15th of January 2019. The total number of patients were 64 patients (32 patients in each group). A conventional open “Milligan-Morgan” hemorrhoidectomy was performed in every patient under general anesthesia and in lithotomy position. Every patient received 500 mg i.v Metronidazole and 1 gm i.v Ceftriaxone before induction of anesthesia. During hospitalization; postoperative analgesia was given on need and included 500mg vial Paracetamol with or without 20 mg Nefopam ampule. For the purpose of the study; patients who were included in the analysis were assigned orderly with a number. Those with Odd numbers were assigned as group A and those with even numbers as group B.
Patients in group A (the study group) were prescribed the following treatment:
Metronidazole 500mg Tablet three times a day for 7 days
Combination of Paracetamol 500mg Tablet and Mefinamic acid (Ponstan) 250 mg capsule to be taken on need
Patients in group B (control group) were only prescribed Combination of Paracetamol 500mg Tablet and Mefinamic acid (Ponstan) 250 mg capsule to be taken on need. The main parameter studied in this analysis was pain. The method of assessment used was using a Visual Analogue Scale (VAS) of 10 degrees. Patients were followed up and came for assessment on day 7 post operatively. The data analyzed using Statistical Package for Social Sciences (SPSS) version 25. The data presented as mean, standard deviation and ranges. Categorical data presented by frequencies and percentages. Student t-test (two tailed) was used to compare the continuous variables among study groups. Chi square test was used to test the association between study groups and categorical variables. A level of P-Value less than 0.05 was considered significant.
The distribution of study patients by general characteristics: Study patient’s age was ranging from 18 to 55 years with a mean of 32.37 years and Standard Deviation (SD) of±10.06 years. The highest proportion of study patients in group A aged ≥ 30 years (56.2%), while (56.2%) of group B were aged < 30 years. Regarding gender, proportion of females was higher than males in group A and B (68.7% versus 31.3% and 56.2% versus 43.8% respectively).
The mean of VAS in the 1st, 3rd, 7th day, and on the 1st bowel motion was significantly lower in patients received metronidazole (Group A) compared to those didn’t receive metronidazole (Group B) (5.46 versus 6.71, p = 0.011; 5.31 versus 7.81, p = 0.001; 4.46 versus 6.25, p = 0.001; and 4.06 versus 6.56, p = 0.001; respectively). No statistical significant difference (p = 0.104) between study groups in mean of VAS in the 2nd day, as shown in Table 1.
Table 1: Comparison between Study Groups by Mean of VAS Postoperatively
| Pain by VAS postoperatively | Study Group | P- Value | |
Group A Mean±SD | Group B Mean±SD | ||
| 1st day | 5.46±1.84 | 6.71±1.95 | 0.011 |
| 2nd day | 7.03±1.61 | 7.65±1.41 | 0.104 |
| 3rd day | 5.31±1.52 | 7.81±1.52 | 0.001 |
| 7th day | 4.06±1.52 | 6.56±1.98 | 0.001 |
| On 1st bowel motion | 4.46±2.05 | 6.25±1.79 | 0.001 |
Postoperatively, the mean of doses of analgesia in the 1st, 3rd, 7th day, and in the 1st bowel motion was significantly lower in patients received metronidazole (Group A) compared to those didn’t receive metronidazole (Group B) (2.75 versus 3.37, p = 0.001; 2.75 versus 3.37, p = 0.002; 2.37 versus 3, p = 0.016; and 3.43 versus 3.93, p = 0.001; respectively).
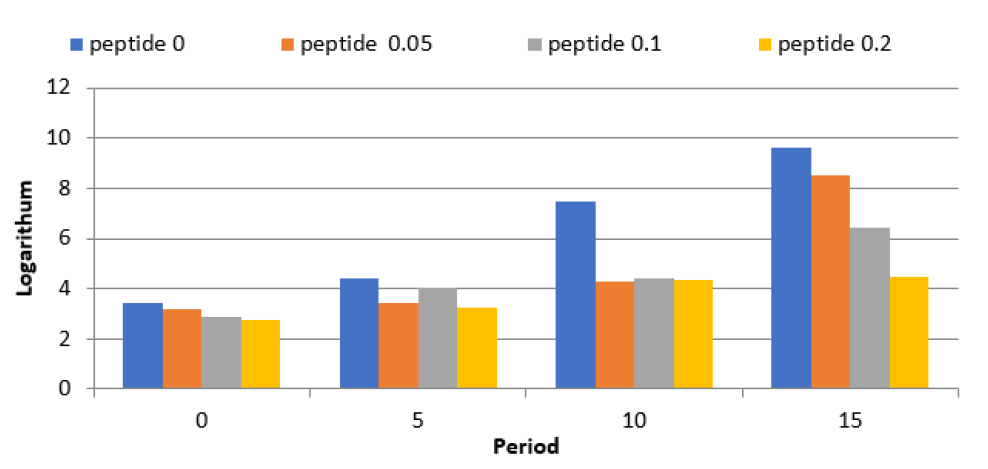
Figure 1: Distribution of Study Groups by Gender
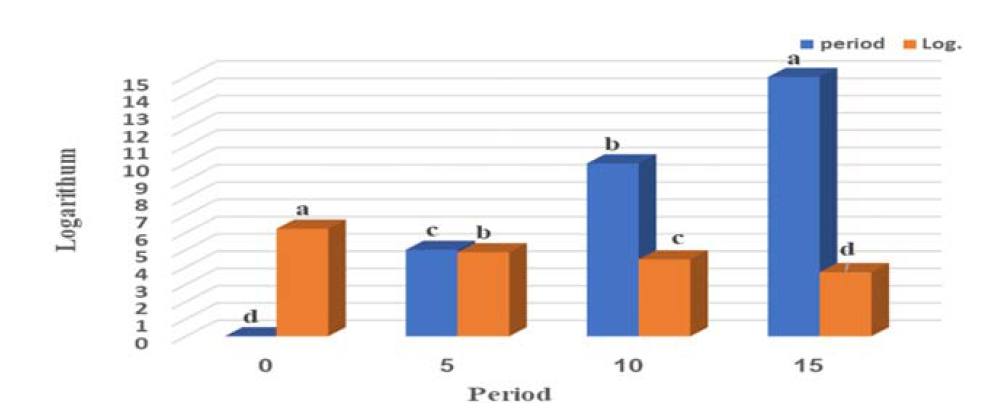
Figure 2: Mean of Doses of Analgesia Required Postoperatively for Study Groups
No statistical significant difference (p = 0.162) between study groups in mean of doses of analgesia in the 2nd day, as demonstrated in Figure 2 and Table 2.
Table 2: Comparison between Study Groups by Mean of VAS Postoperatively
| Doses of analgesia required postoperatively | Study Group | p-value | |
Group A Mean±SD | Group B Mean±SD | ||
| 1st day | 2.75±0.84 | 3.37±0.6 | 0.001 |
| 2nd day | 3.37±0.7 | 3.62±0.7 | 0.162 |
| 3rd day | 2.75±0.76 | 3.37±0.79 | 0.002 |
| 7th day | 2.37±0.87 | 3.0±1.13 | 0.016 |
| On 1st bowel motion | 3.43±0.61 | 3.93±0.56 | 0.001 |
Returning to normal activity was significantly earlier in patients received metronidazole postoperatively (Group A) than in those who didn’t receive metronidazole (Group B) (5.68 versus 7.12 days, p = 0.028). No statistical significant difference (p = 0.11) between study groups in mean of time of 1st bowel motion as in Table 3.
Table 3: Comparison in mean of Time of 1st Bowel Motion and Days until Returning to Normal Activity Postoperatively in Study Groups
| Variable | Study Group | p-value | |
Group A Mean±SD | Group B Mean±SD | ||
| Days for returning to normal activity | 5.68±1.46 | 7.12±3.25 | 0.028 |
| Time of 1st bowel motion | 2.18±0.82 | 2.5±0.71 | 0.11 |
The comparison between study groups by postoperative wound infection is shown in Table (4). We noticed that there was no statistical significant difference (p = 0.229) between study groups regarding postoperative wound infection.
Table 4: Comparison between Study Groups by Postoperative Wound Infection
Wound infection | Study Group | p-value | |
Group A (%) n = 32 | Group B (%) n = 32 | ||
| Yes | 2 (6.3) | 5 (15.6) | 0.229 |
Pain remains the most common symptom found in postoperative anal surgery, the current study is concerned with the assessment of the response of open hemorrhoidectomy pain for postoperative treatment with oral metronidazole over one week. The cohort of patient included in the current analysis have a mean age of 32.37 years (SD + 10.06 years), the proportion of females was higher than males. The majority were diagnosed with hemorrhoid grade III. Among the two groups studied; there was no statistical significant difference (p≥0.05) regarding age and gender. Gallo et al. [13], different results observed. The mean age of the participants was 53 years, which ranged between 30 and 78 years, also noticed a male predominance which represented 62.3% of the study patients with male to female ratio of 1.6:1, a similar results observed, as found that grade III hemorrhoids observed in majority of patients subjected to hemorrhoidectomy and formed 81.1% of the study patients and grade IV disease represented the remaining 18.9%. Furthermore, in Medina-Gallardo et al. [14], the mean of the participants age was 51.7 years, 50.8% of them were women and 49.2% of the remaining were men, with female to male ratio of 1.05:1. González et al. [15], in which, according to the hemorrhoidal disease classification, the majority were having grade III disease. Al-Mulhim et al. [6], the majority of patients included were with Grade IV hemorrhoid. Madhu et al. [17] noticed that grade III was more prevalent among patients included in the study than grade IV (63.3% Vs 36.7%). Differently, Wanis et al. [18] observed that patients who received metronidazole had significantly lower reported pain scores on 1st postoperative day (p = 0.046) and 4th postoperative day (p = 0.044) only. In contrast, in the study of Khan et al. [19] which involved 100 patients undergone hemorrhoidectomy and divided into two groups, (Group A) did not receive any prophylactic antibiotic whereas group B received metronidazole; Pain was compared between both groups from 1st post-op day to 7th post-op day. Results obtained showed that difference in pain score was insignificant between both groups at 1st, 2nd, 3rd, 4th, 5th, 6th and 7th POD (p>0.05), which was in line with Wesarachawit et al. [20], as showed no difference in the pain scores and consumption of analgesics between the two groups included in their retrospective study. There was no significant difference in the total dosages of pethidine given postoperatively, which was 1.06+0.83 and 1.03+0.78 mg/kg in the metronidazole and the non-antibiotic group respectively (p = 0.747). The reasons for the differences observed in the mentioned studies in postoperative pain are attributed to a variety of factors, like; the incisions made during surgery, suturing the anal mucosa, surgical manipulation of tissues and subsequent edema and bacterial colonization, In addition, the type of operation performed may also lead to changes in the results obtained. If wound edges are sutured in closed hemorrhoidectomy, it would facilitate more rapid healing and may cause less pain than in open hemorrhoidectomy. Another important reason could be that the sample size and hence the number of outcomes of interest was too small for the differences to be statistically significant. Metronidazole may limit the inflammatory phase of scarring and may reduce the bacterial count sufficiently to allow the transition to the fibroblastic phase and rapid granulation of scarring, which thereby decreases postoperative pain. In the current study, there was no statistically significant difference (p = 0.229) between study groups regarding postoperative wound infection. Different results were observed in Shaikh et al. [21] in which patients undergone hemorrhoidectomy assessed for wound complications. Results obtained showed that wound infection was observed in only (0.9%) of patients of open hemorrhoidectomy and (1.9%) in patients of closed one. Another dissimilar results were observed in Wesarachawit et al. [20] in which, at 2nd week, there were two wound dehiscence (2.25%) in groups received metronidazole. In this study, returning to normal activity was significantly earlier in Group A than in Group B (5.68 versus 7.12 days, p = 0.028), while a statistically insignificant difference (p = 0.11) between study groups in mean of time of 1st bowel motion was reported. Comparable results observed in González et al. [15] who found that time until resumption of daily life activities was significantly earlier in study group than in control group, as the mean and SD of days to return to normal activity was 7.59±1.56 days and 14.73±3.76 days for the study and control group, respectively. Furthermore, another similar results observed by Wanis et al. [18], metronidazole use was associated with a significantly shorter time to return to normal activities (p = 0.027). Finally; a similar results observed by Al-Mulhim et al. [16], they studied 84 patients who received metronidazole and 82 patients who did not.
They found a significant faster resumption of daily life activities in the group that received metronidazole in comparison to those not received it (p<0.05), but time to 1st bowel motion was not significantly different between both groups (p>0.05). They concluded that Prophylactic metronidazole in Milligan-Morgan hemorrhoidectomy is associdated with an earlier return to normal activity.
Mott, T. et al. “Hemorrhoids: Diagnosis and Treatment Options.” American Family Physician, vol. 97, no. 3, Feb. 2018.
Lohsiriwat, V. “Hemorrhoids: From basic pathophysiology to clinical management.” World Journal of Gastroenterology, vol. 18, no. 17, May 2012, p. 2009.
Riss, S. et al. “The Prevalence of hemorrhoids in adults.” International Journal of Colorectal Disease, vol. 27, no. 2, 2012, pp. 215–220.
Beck, D.E. The ASCRS Textbook of Colon and Rectal Surgery. 2nd Edn., Springer, 2011, p. 175.
Loudon, M.A. “Haemorrhoid Surgery: What Is Best Practice?” In Recent Advances in Surgery 30, edited by I. Taylor and C. Johnson, pp. 128–129.
Kaidar-Person, O. “Hemorrhoidal disease: A comprehensive review.” Journal of the American College of Surgeons, vol. 204, 2007, pp. 102–117.
Chaleoykitti, B. “Comparative Study Between Multiple and Single Rubber Band Ligation in One Session for Bleeding Internal Hemorrhoids: A Prospective Study.” Journal of the Medical Association of Thailand, vol. 85, 2002, pp. 345–350.
American Gastroenterological Association. “Medical Position Statement: Diagnosis and Treatment of Hemorrhoids.” Gastroenterology, vol. 126, 2004, pp. 1461–1462.
Lohsiriwat, V. “Approach to Hemorrhoids.” Current Gastroenterology Reports, vol. 15, 2013, p. 332.
Okuş, A. “Local Pain-Reducing Methods after Hemorrhoidectomy.” World Journal of Surgery, vol. 37, no. 8, Aug. 2013, pp. 2007–2008.
Alper, D. et al. “Resting Anal Pressure Following Hemorrhoidectomy and Lateral Sphincterotomy.” Diseases of the Colon & Rectum, vol. 48, no. 11, Nov. 2005, pp. 2080–2084.
Chen, H.H. “Anal Manometric Findings Before and After Hemorrhoidectomy: A Preliminary Report.” Changgeng Yi Xue Za Zhi, vol. 22, no. 1, Mar. 1999, pp. 25–30.
Gallo, G. et al. “Efficacy of mesoglycan in pain control after excisional hemorrhoidectomy: A pilot comparative prospective multicenter study.” Gastroenterology Research and Practice, 2018.
Medina-Gallardo, A. et al. “Is severe pain after milligan–morgan hemorrhoidectomy still a major postoperative problem? A case series of 117 consecutive patients.” International Journal of Surgery Case Reports, vol. 30, Jan. 2017, pp. 73–75.
González-Ojeda, A. et al. “Efficacy of metronidazole versus placebo in pain control after hemorrhoidectomy: Results of a controlled clinical trial.” Revista Española de Enfermedades Digestivas, vol. 107, no. 11, 2015, pp. 681–685.
Al-Mulhim, A.S. et al. “Post Hemorrhoidectomy Pain: A Randomized Controlled Trial.” Saudi Medical Journal, vol. 27, no. 10, 2006, pp. 1538–1541.
Madhu, B.S. et al. “Harmonic scalpel compared with conventional open (milligan–morgan) method in surgical management of symptomatic Haemorrhoids.” International Surgery Journal, vol. 4, no. 6, May 2017, pp. 2010–2013.
Wanis, K.N. et al. “Systemic metronidazole may not reduce posthemorrhoidectomy pain: A meta-analysis of randomized controlled trials.” Diseases of the Colon & Rectum, vol. 60, no. 4, Apr. 2017, pp. 446–455.
Khan, K.I. et al. “Role of prophylactic antibiotics in milligan–morgan hemorrhoidectomy: A randomized control trial.” International Journal of Surgery, vol. 12, 2014, pp. 868–871.
Wesarachawit, W. and J. Pattana-arun. “Antibiotics and early postoperative complications of closed hemorrhoidectomy: A retrospective matched pair study.” Journal of the Medical Association of Thailand, vol. 90, no. 9, Sept. 2007, p. 1828.
Shaikh, A.R. et al. “An evaluation of milligan–morgan and ferguson procedures for haemorrhoidectomy at Liaquat University Hospital.” Pakistan Journal of Medical Sciences, vol. 29, no. 1, Jan. 2013, p. 122.
