
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Chronic periodontitis is an infectious disease characterized by gingival inflammation and loss of supporting periodontal tissues leading to destruction of bone and tooth mobility. Langerhans’ cells are unique population of antigen presenting cells which recognize the antigen, capture it, present it to T-lymphocytes and initiates an immune response. They may represent as “key cells” in pathogenesis and development of periodontal diseases. CD1a is considered as a reliable approach for identifying Langerhans’ cells immunohistochemically. Aims and Objectives: To assess and compare the Langerhans cell expression in Chronic Periodontitis and normal gingival epithelium using anti CD1a antibody. The objective of the present study was to compare and evaluate both quantitatively and qualitatively the expression of CD1a in Chronic periodontitis and normal gingiva. Materials and Methodology: A group of 60 individuals included a study group of 30 individuals having chronic periodontitis and a control group of 30 individuals with clinically healthy normal gingiva. The patients with history of systemic diseases, tobacco usage, who had received periodontal treatment in a recent period of time, are excluded in the sample. Informed consent was taken from the patients along with institutional ethical clearance. The gingival biopsies are collected from the Department of Periodontics, Oral Surgery and Orthodontics were fixed in neutral buffered formalin and are stained immunohistochemically for the detection of Langerhans cells using anti CD1a. Dark brown stain of varying intensity scattered within the gingival epithelial were identified as CD1a positive cells. The data obtained were tabulated and subjected to statistical analysis. Results: The mean of Langerhans cells and staining intensity was increased in the study group when compared to that of the control group. The statistical significance was observed in relation to location with increased expression of stratum basale and stratum spinosum. Conclusion: Results showed that there is significant increased expression of mean of Langerhans cells and staining intensity in the study group when compared to that of the control group concludes that there is an increased host immune response in study group.
The periodontium consists of the investing and supporting tissues of the tooth in which soft tissues include gingiva, periodontal ligament and hard tissues like cementum and alveolar bone. The gingiva protects the underlying tissues and the periodontal ligament, cementum and alveolar bone, forming the attachment apparatus. Homeostasis is maintained by various physiological remodeling activities of periodontium [1].
Gingivitis is a non-destructive infectious disease and is characterized by inflammation of the soft tissues surrounding the teeth, which appears clinically as a change in tissue colour and consistency, and can be associated with swelling and a tendency to bleed upon slight provocation [2]. Periodontitis is a destructive multifactorial infectious disease initiated by a biofilm of bacteria on the teeth which trigger an immune-inflammatory response in the adjacent host tissues characterized by the inflammation of the periodontal soft and hard tissues resulting in apical migration of the epithelial attachment, periodontal attachment and alveolar bone loss [3]. The gingival epithelial tissue is important as a physical barrier against external pathogens and play an active role in innate host defenses by responding to bacteria in an interactive manner with specialized dendritic cells.4 Members of the dendritic cell lineage have potent immunostimulatory properties and are widely distributed throughout the body. In the oral epithelium two types of dendritic cells were reported:
Melanocytes in the basal cell layer known as low level dendritic cells
Langerhans cells in the suprabasal and superficial layers known as high level dendritic cells [5]
Langerhans cells (LCs) were first recognized dendritic cells and discovered by Paul Langerhans in 1868, and was named by Inga Silberberg in 1973. These cells are derived from bone marrow and migrate via the blood stream to the peripheral tissue which constitutes an antigen trapping network. The LCs are a type of antigen presenting cells (APCs) and their function is to recognize the antigen, capture it and initiate an early immune response. After capturing the antigen, the Langerhans cells migrate to regional lymph nodes and are converted into mature dendritic cells capable of priming naive T cells [6]. Langerhans cells are immunocompetant and they function as part of the body’s peripheral immune system.
Humans express five CD1 proteins, four of which are surface expressed antigen-presenting molecules (CD1a, CD1b, CD1c, and CD1d) [7]. Each of the four CD1 isoforms differ in size of the antigen-binding grooves, intracellular trafficking patterns, lipid ligand repertoire, and tissue distribution of expression. LCs were shown to express high levels of CD1a, which belongs to family of CD1 group proteins [8]. Among all the markers used, CD1a immunolabelling is considered to be the most dendritic cells and discovered by Paul Langerhans in 1868, and was named by Inga Silberberg in 1973. These cells are derived from bone marrow and migrate via the blood stream to the peripheral tissue which constitutes an antigen trapping network. The LCs are a type of antigen presenting cells (APCs) and their function is to recognize the antigen, capture it and initiate an early immune response. After capturing the antigen, the Langerhans cells migrate to regional lymph nodes and are converted into mature dendritic cells capable of priming naive T cells [6]. Langerhans cells are immunocompetant and they function as part of the body’s peripheral immune system.
Humans express five CD1 proteins, four of which are surface expressed antigen-presenting molecules (CD1a, CD1b, CD1c, and CD1d) [7]. Each of the four CD1 isoforms differ in size of the antigen-binding grooves, intracellular trafficking patterns, lipid ligand repertoire, and tissue distribution of expression. LCs were shown to express high levels of CD1a, which belongs to family of CD1 group proteins [8]. Among all the markers used, CD1a immunolabelling is considered to be the most reliable method to identify the human Langerhans cells [5]. The number of Langerhans’ cells in gingival tissues is a topic of much speculation. Various studies have reported the increased number of LCs in periodontitis, compared to healthy periodontal tissues [9]. Hence Langerhans’ cells as antigen presenting cells could influence the pathogenesis of chronic periodontitis. With this background the present study aimed to evaluate the IHC expression of the density, intraepithelial distribution and morphology of Langerhans’ cells in chronic periodontitis and normal gingiva using anti-CD1a antibody.
Study Design
The present study was conducted in the department of Oral and maxillofacial pathology by collecting gingival tissue biopsies obtained from the patients undergoing treatment in the departments of Periodontics, Orthodontics and Oral and Maxillo-facial Surgery, Vishnu Dental College, Vishnupur, Bhimavaram. Institutional ethical clearance was obtained to conduct the study. The study group included 30 clinically diagnosed cases of chronic periodontitis. The control group included 30 cases of clinically normal gingiva. The inclusion and exclusion criteria were followed in case selection.
Inclusion Criteria
Patients who were clinically diagnosed as having chronic periodontitis and required gingivectomy as part of treatment procedure
Individuals with clinically healthy gingiva which included:
Patients indicated for surgical crown lengthening procedure for fixed prosthesis, surgical extraction of impacted teeth, and extraction of premolars and third molars prior to orthodontic treatment
Exclusion Criteria
Patients with history of systemic diseases
Patients with history of tobacco usage
Patients who had received periodontal treatment in the past 6 months
Case sheet was maintained for each individual. All the personal and clinical data were recorded. Assessment of periodontal status of the study group was collected.
Patients were explained about the surgical procedure, informed consent was obtained from the patients and from the concerned departments. Gingival biopsies from the sites of chronic periodontitis in diseased group and sites representing healthy gingivain control group were collected from the respective departments. Gingival tissues were washed in normal saline to remove the blood clots and were fixed in 10% neutral buffered formalin solution. Tissues were processed, properly oriented, embedded in paraffin blocks and sectioning was done. Paraffin embedded tissue sections of healthy and diseased gingiva were stained by haematoxylin and eosin and the serial sections of the same were stained by immunohistochemical reagent (CD1a antibody).
Equipments
Microtome, Hot plate, Microwave Oven, measuring jars, Coplin jars, Pipettes, Timers, Absorbent wipes, Olympus BX51 research microscope with image pro plus software version 6.0, 3-Aminopropyl tri-ethoxysilane coated glass slides (Positively Charged slides) and Cover slips for slides.
Reagents
Primary antibody
Anti-CD1a (Biogenex)
Secondary antibody
Super Enhancer (Enhances the signal) (Biogenex)
Poly HRP (Anti-mouse and rabbit IgG with enzyme polymer) (Biogenex)
Blocking agents:
Peroxide block- Blocks endogenous peroxides
Protein block- Blocks all non-specific sites. Reduces background stain, 10% normal serum is used
Chromogen: DAB (3,3–diaminobenzidine) substrate (Biogenex)
De-ionized water
PBS (Phosphate Buffer Saline)
Tri-sodium Citrate buffer for Antigen retrieval
Preparation of Tri-sodium Citrate Buffer
2.94 gm of Tri-sodium citrate dissolved in 1000 ml of distilled water and 5 ml of 1N HCl and pH is maintained at 6.0-6.4
Haematoxylin And Eosin Staining
Formalin fixed paraffin embedded tissues were sectioned at 4μm thickness and taken for routine H and E staining.
Immunohistochemistry Procedure
Tissue Preparation
Sectioning: Formalin fixed paraffin embedded tissues were sectioned at 3μm and mounted on positively charged slides
Deparaffinisation:
Overnight incubation (60°C)
Xylene – I (10 min)
II (10 min)
Alcohol – 100% (5 min)
80% (5 min)
70% (5 min)
Running in tap water (5 min)
Wash in distilled water (2 min)
Antigen retrieval in microwave oven:
Microwave oven is pre heated at 450 W for 3 min
Antigen retrieval was done by using Tri-sodium citrate buffer at 600 W for 5min (3 cycles) The solution was allowed to cool at room temperature and then washed in PBS (4ml of Phosphate buffer + 100 ml of distilled water) for 5 min
Peroxide block was added for 10 min at room temperature
Slides were then washed in PBS for 2 min
Slides were power blocked for 10 min. to prevent non-specific staining
Slides were blot drained
Slides were incubated with primary antibody anti -CD1a for 1 hour
Slides were washed with wash buffer (PBS) for 5 min
Slides were incubated with secondary antibody
Super enhancer for 20 min, Wash in PBS for 2 min, followed by Poly HRP for 45 min.
Excess was wiped off and slides were washed with wash buffer (PBS) 2 changes for 5min. Slides were incubated with DAB substrate chromogen for 15 min. Slides were rinsed with distilled water for 2-4min. Slides were counterstained with 1 dip of Harris haematoxylin followed by bluing in running tap water. Slides were dipped twice in 100% alcohol. Slides were air dried. Slides were dipped once in Xylene. Slides were air dried. Sections were mounted using DPX.
Positive Controls
Thymus serves as an external positive control for CD1a.
Immunohistochemical Analysis of Langerhans Cells
Following the immunohistochemical staining, all the stained sections of gingiva, which included 30 diseased and 30 normal tissues, were studied using Olympus BX51 research microscope with image pro plus software version 6.0. Cells with dark brown stain within the gingival tissue were identified as Langerhans positive cells and analyzed qualitatively and quantitatively.
Qualitative Analysis
The staining intensity of immunopositive cells was compared with staining intensity of external control and graded as mild, moderate and intense.
Quantitative Analysis
For quantitative analysis 5 representative areas were randomly selected in each slide by scanning in low power using Olympus BX51 microscope from left to right. Photomicrographs were taken at 40X magnification using Olympus DP71 camera attached to Olympus BX51 microscope and image pro plus software. Counting method:
Counting of the cells was done using image J software
Number of positive cells in each high-power field was counted and the total number of positive cells in 5 high power fields was calculated
The mean number of positive cells in each case was recorded in three layers of gingival epithelium i.e. stratum basale, deep stratum spinosum and superficial stratum spinosum
Results were tabulated and subjected to statistical analysis p value of <0.05 is considered as statistically significant and <0.01 as highly significant statistically. A total of 60 cases were included out of which 30 cases were of Chronic Periodontitis constituting study group and 30 cases with normal gingiva forms the control group. The study group consisted of 16 males and 14 females and control group included 20 males and 10 females within the age groups of 21-30 years, 31-40 years and 41-50 years. The control group subjects are having clinically healthy gingiva and had no history of smoking and other tobacco related habits. Gender-wise distribution and age of the control and study group are given in Tables 1 and 2.
Table 1: Comparison of Gender distribution Among Control and Study Groups
Parameters | Males | Females | Total |
Normal Gingiva | 20 | 10 | 30 |
Chronic Periodontitis | 16 | 14 | 30 |
Table 2: Comparison of Age Distribution Among Control and Study Groups
Parameters | 21-30 years | 31-40 years | 41-50 years |
Normal Gingiva | 21 | 06 | 03 |
Chronic Periodontitis | 06 | 15 | 09 |
Staining Intensity of Langerhans Cells in Subjects of Normal Gingiva and Chronic Periodontitis
In normal gingiva the staining intensity of LCs was predominantly mild and moderate.
The staining intensity of LCs was predominantly moderate, mild in some cases and intense only in few cases of chronic periodontitis. The statistical analysis was performed using Chi-Square test and high statistical significance was observed. (Table 3, Figure 3).
Table 3: Staining Intensity of Langerhans Cells in Subjects of Normal Gingiva and Chronic Periodontitis
| Staining Intensity | Normal Gingiva (N) | Chronic Periodontitis (N) | p value |
Mild | 25 | 12 | 0.002* |
Mild | 25 | 12 | - |
Moderate | 5 | 14 | |
Intense | 0 | 4 | |
Total Count (N) | 30 | 30 | - |
*p (0.002)– Highly significant using Chi-Square test
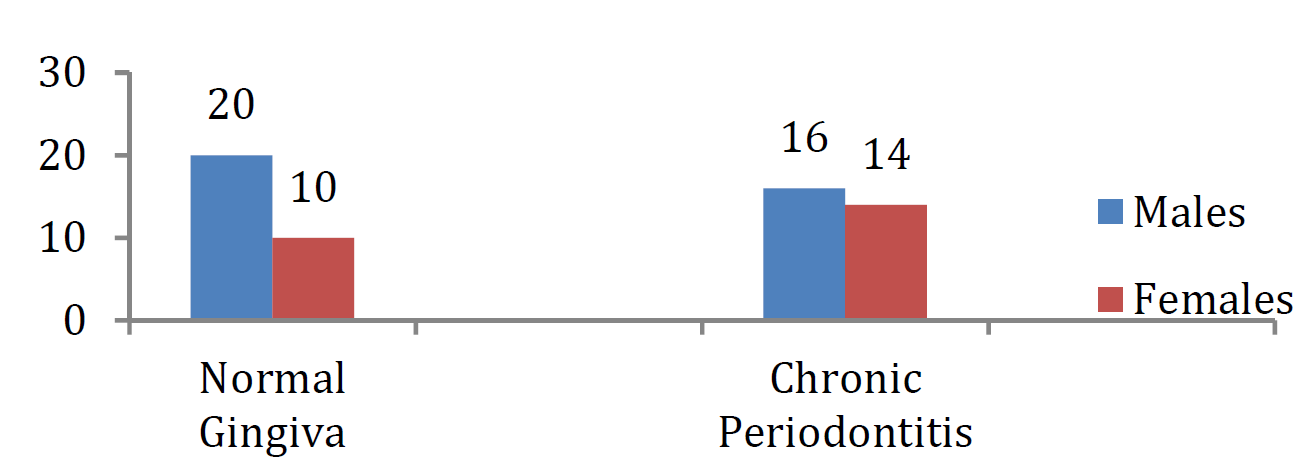
Figure 1: Comparison of Gender Distribution Among Control and Study Groups
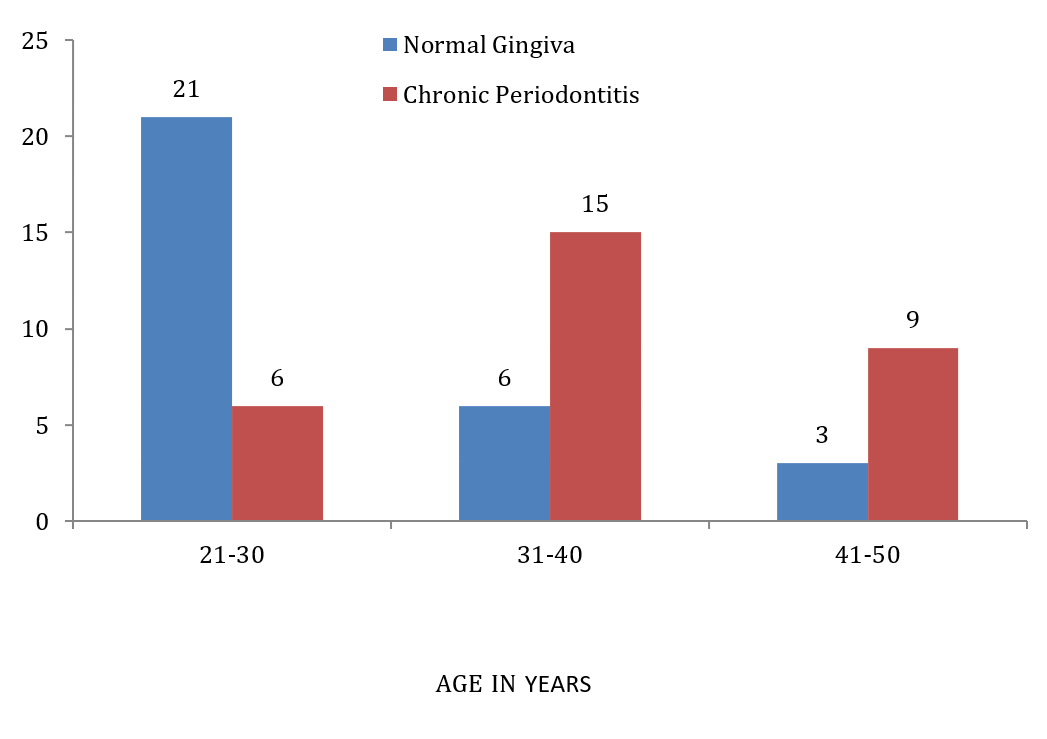
Figure 2: Comparison of Age Distribution Among Control and Study Groups
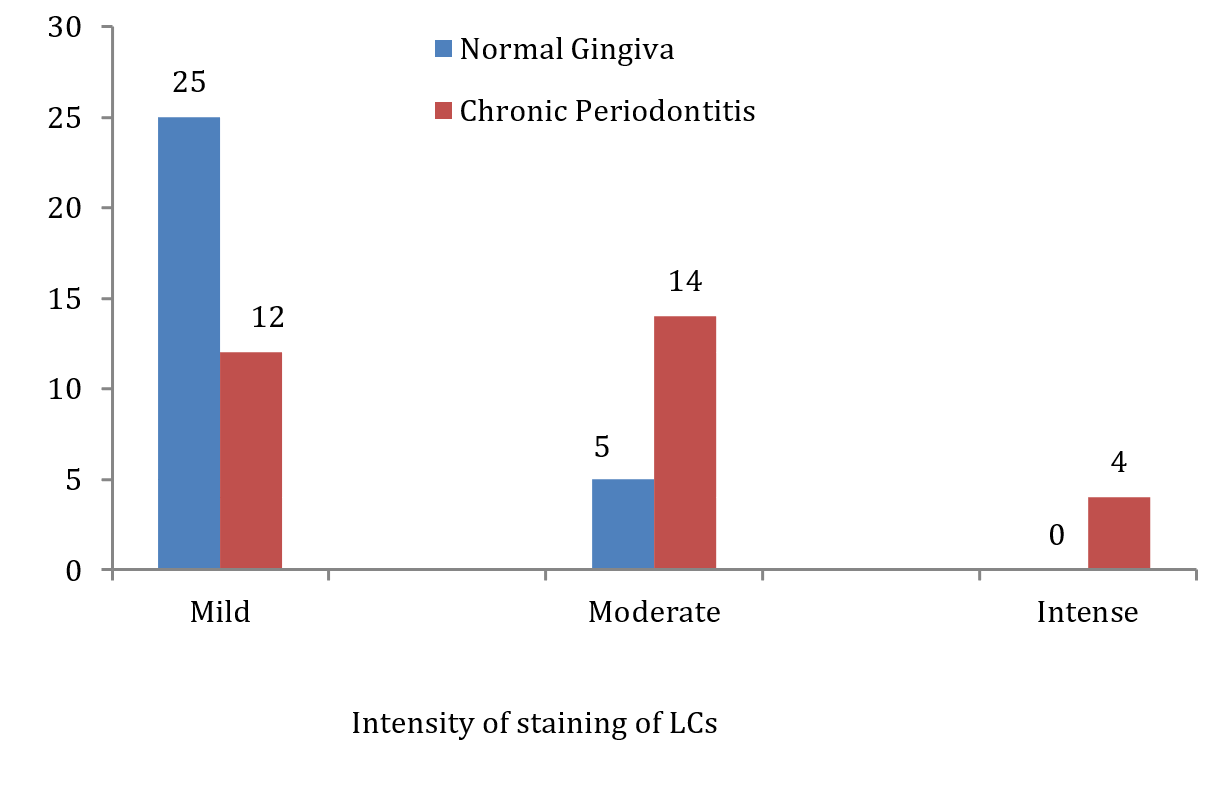
Figure 3: Staining Intensity of Langerhans Cells in Subjects of Normal Gingiva and Chronic Periodontitis
Staining Intensity of Langerhans Cells in Subjects Among Different Age Groups of Normal Gingiva and Chronic Periodontitis
The staining intensity of LCs was predominantly mild among different age group individuals of normal gingiva. The staining intensity of LCs was predominantly mild to moderate among 21-30 and 41-50 age groups whereas mild to moderate and intense was seen in few cases of 31-40 age groups of chronic periodontitis. The statistic alanalysis was performed using Chi-Square test and statistical significance was observed. (Table 4, Figure 4).
Table 4: Comparison of Staining Intensity of Langerhans Cells in Subjects Among Different Age Groups of Normal Gingiva and Chronic Periodontitis
| Age groups | Intensity | Normal Gingiva (N) | Chronic Periodontitis (N) | p value |
21-30 years | Mild | 17 | 3 |
0.05 |
Moderate | 4 | 3 | ||
Intense | 0 | 0 | ||
31-40 years | Mild | 5 | 5 | |
Moderate | 1 | 6 | ||
Intense | 0 | 4 | ||
41-50 years | Mild | 3 | 4 | |
Moderate | 0 | 5 | ||
Intense | 0 | 0 |
*p (0.05) – statistically significant using Chi-Square test
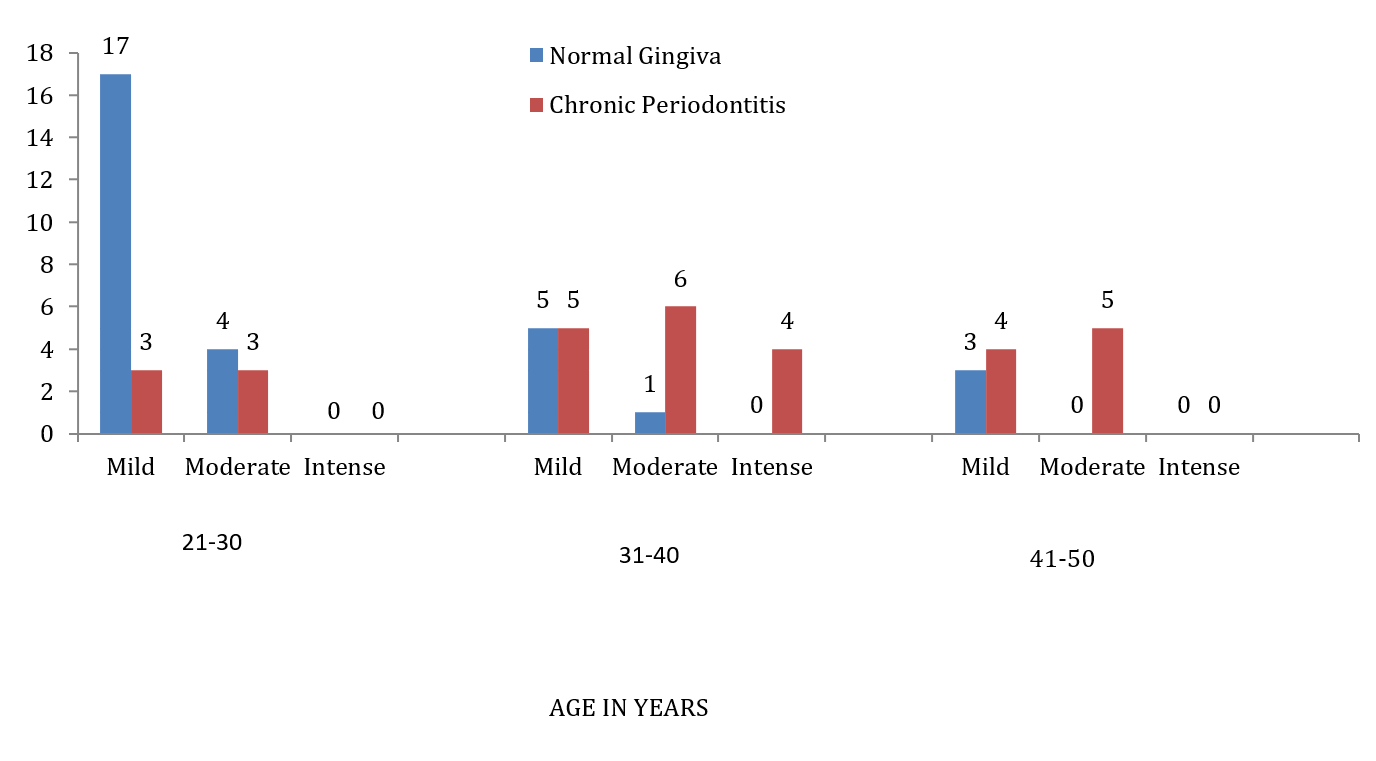
Figure 4: Comparison of Staining Intensity of Langerhans Cells in Subjects Among Different Age Groups of Normal Gingiva and Chronic Periodontitis
Mean Of Langerhans Cells in Subjects with Normal Gingiva and Chronic Periodontitis
The mean of Langerhans cells was significantly higher in gingival epithelium of chronic periodontitis group compared to that of normal gingiva group. The statistical analysis was performed using Mann-Whitney U test and high statistical significance was observed. (Table 5, Figure 5).
Table 5: Comparison of Mean of Langerhans Cells in Subjects with Normal Gingiva and Chronic Periodontitis
| Parameters |
N | Mean of LCs (Mean ± SD) |
p value |
Normal gingiva | 30 | 51.83 ± 18.30 |
0.008* |
Chronic Periodontitis | 30 | 61.93 ± 20.17 |
*p (0.008) – Highly significant using Mann-Whitney U test
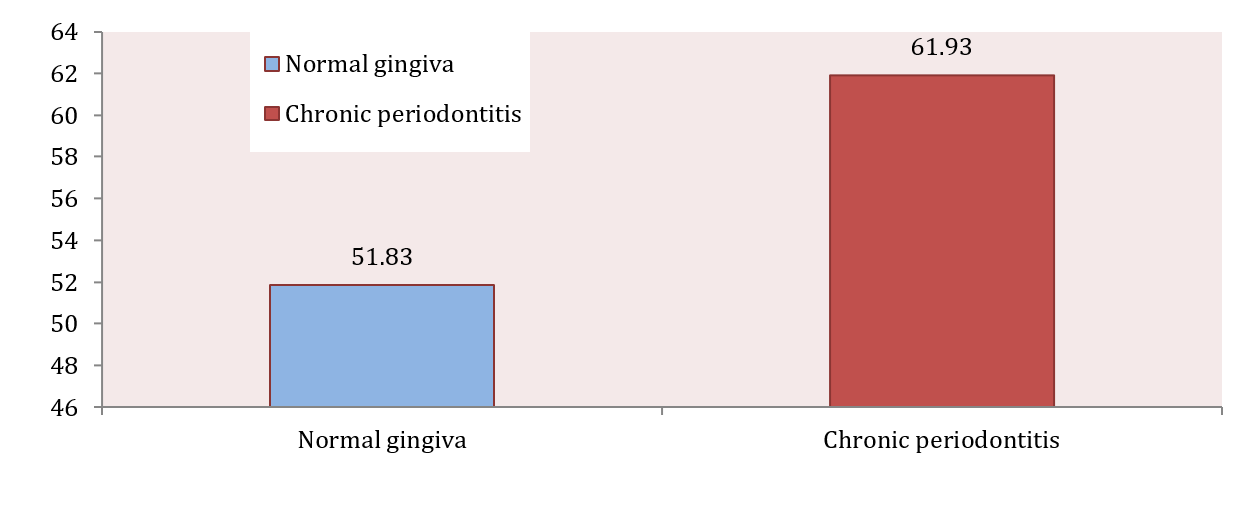
Figure 5: Comparison of Mean of Langerhans Cells Between Normal Gingiva Group and Chronic Periodontitis Group
Mean Of Langerhans Cells in Different Age Groups of Subjects with Normal Gingiva and Chronic Periodontitis
The mean of Langerhans cells in gingival epithelium of chronic periodontitis was higher in 31-40 & 41-50 age groups and lower in 21-30 age groups when compared to normal gingiva. The statistical analysis was performed using Kruskal-Walli’s test and no statistical significance was observed. (Table 6, Figure 6).
Table 6: Comparison Of Mean of Langerhans Cells with Different Age Groups in Normal Gingiva and Chronic Periodontitis Subjects
| Age | Number of Subjects | Mean of LCs (Mean± SD) | p value |
21- 30 years Normal gingiva Chronic Periodontitis |
21 6 |
53.00± 9.66 52.16± 1.64 |
0.775 |
31 - 40 years Normal gingiva Chronic Periodontitis |
6 15 |
48.66± 1.28 67.86± 2.37 | |
41 - 50 years Normal gingiva Chronic Periodontitis |
3 9 |
50.00± 8.54 58.55± 1.57 | - |
p (0.775)- Not significant using Kruskal-Wallis test
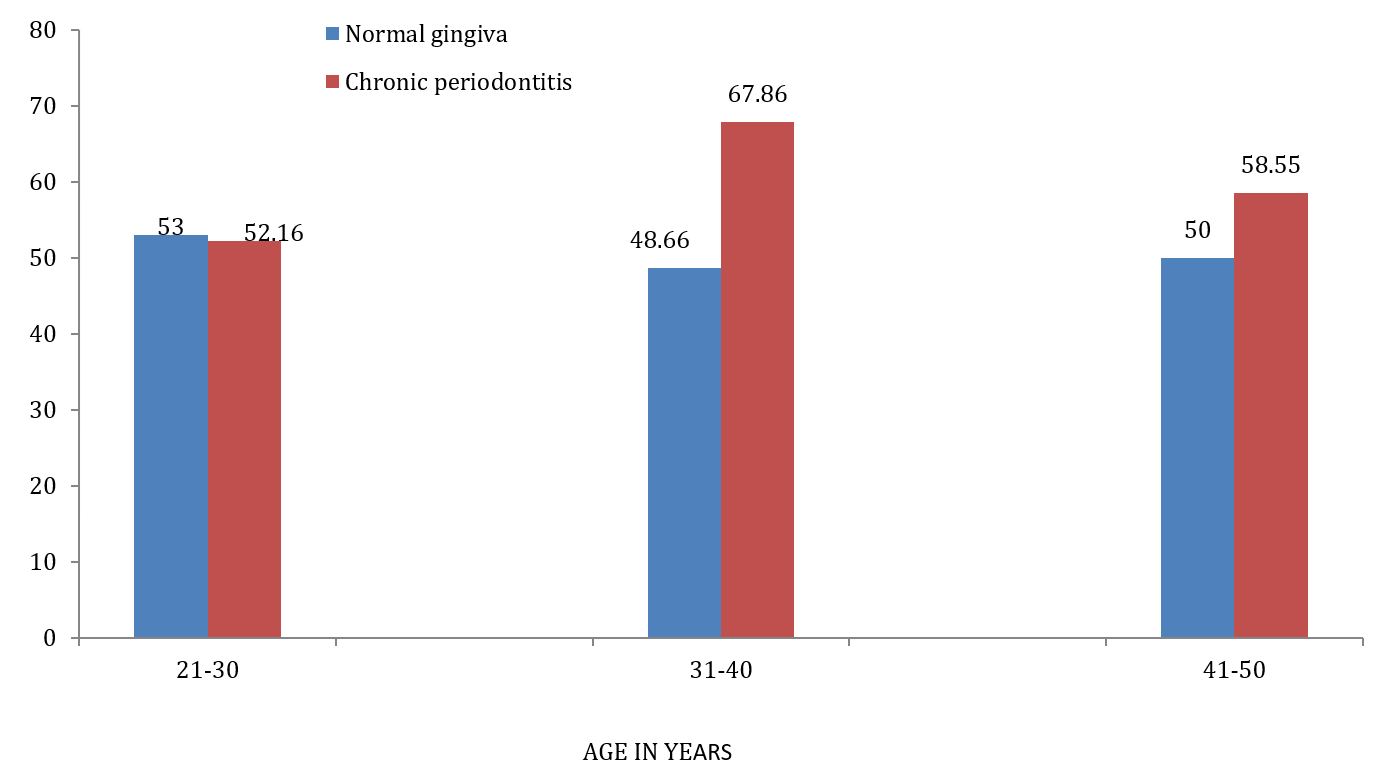
Figure 6: Comparison of Mean of Langerhans Cells with Different Age Groups in Normal Gingiva and Chronic Periodontitis Subjects
Mean Of Langerhans Cells in Subjects with Normal Gingiva and Chronic Periodontitis Based on Location
The mean of Langerhans cells in gingival epithelium of chronic periodontitis was higher in S. Basale, Deep S. Spinosum and superficial S. Spinosum when compared to normal gingiva. The statistical analysis was performed using Mann-Whitney U test and statistical significance was observed in S. Basale & Superficial S. Spinosum and no statistical significance was observed for Deep S. Spinosum. (Table 7, Figure 7).
Table 7: Comparison of mean of Langerhans cells based on Location in Subjects with Normal gingiva and Chronic Periodontitis
| Parameters | N | Mean of LCs (Mean ± SD) | p value |
S.Basale Normal Gingiva Chronic Periodontitis |
30 30 |
14.10±2.36 17.53 ±8.00 |
0.029* |
Deep S. Spinosum Normal Gingiva Chronic Periodontitis |
30 30 |
22.83±4.88 25.73±1.19 |
0.087 |
Superficial S. Spinosum Normal Gingiva Chronic Periodontitis |
30 30 |
14.90±11.04 18.66±10.96 |
0.011* |
*p (<0.05) – Statistically significant using Mann-Whitney U test
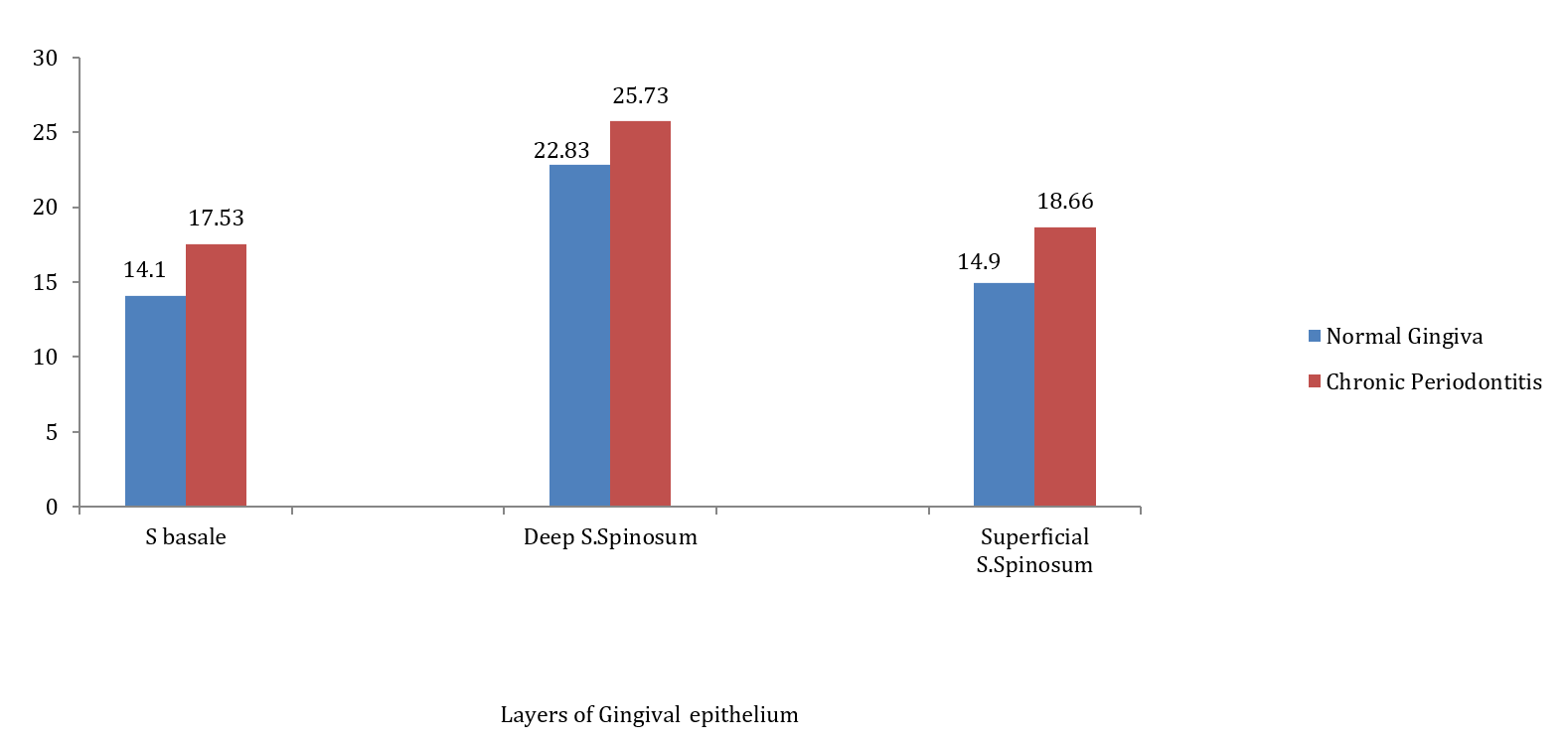
Figure 7: Comparison of Mean of Langerhans Cells Based on Location in Subjects with Normal Gingiva and Chronic Periodontitis
Mean Of Langerhans Cells in Subjects of Different Age Groups Based on Location
In gingival epithelium of normal gingiva of different age groups, the mean of LCs was observed to be highest in deep stratum spinosum and lowest in the superficial stratum spinosum except in 21-30 years age group where stratum basale is lowest. The statistical analysis was performed using Kruskal-Walli’s test and no statistical significance was observed.
In gingival epithelium of chronic periodontitis group, the mean of LCs was high in the deep stratum spinosum and low in the stratum basale. The statistical analysis was performed using Kruskal-Walli’s test and no statistical significance was observed. (Table 8, Figure 8).
Table 8: Mean of Langerhans Cells in Different Age Groups Based on Location
Normal Gingiva | Age groups - Layers | N | Mean of LCs (Mean ± SD) | p value | |
21-30 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
21 |
13.80 ± 2.20 22.85 ± 5.05 16.33 ± 12.63 |
0.635
| ||
31-40 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
6
|
14.83 ±2.92 23.00 ± 5.40 10.83 ± 5.52 |
0.882
| ||
41-50 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
3 |
14.66 ±2.88 22.33 ± 4.16 13.00 ± 4.58 |
0.533
| ||
Chronic Periodontitis | 21-30 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
6 |
14.33 ± 5.85 22.66 ± 1.09 15.16 ± 6.46 |
0.230
| |
31-40 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
15 |
20.00 ± 9.27 27.33 ± 1.40 20.53 ± 14.27 |
0.667
| ||
41-50 years S. Basale Deep S. Spinosum Superficial S. Spinosum |
9 |
15.55 ± 6.08 25.11 ± 9.34 17.88 ± 6.15 |
0.572 | ||
p (>0.05)- Not significant using Kruskal-Wallis test
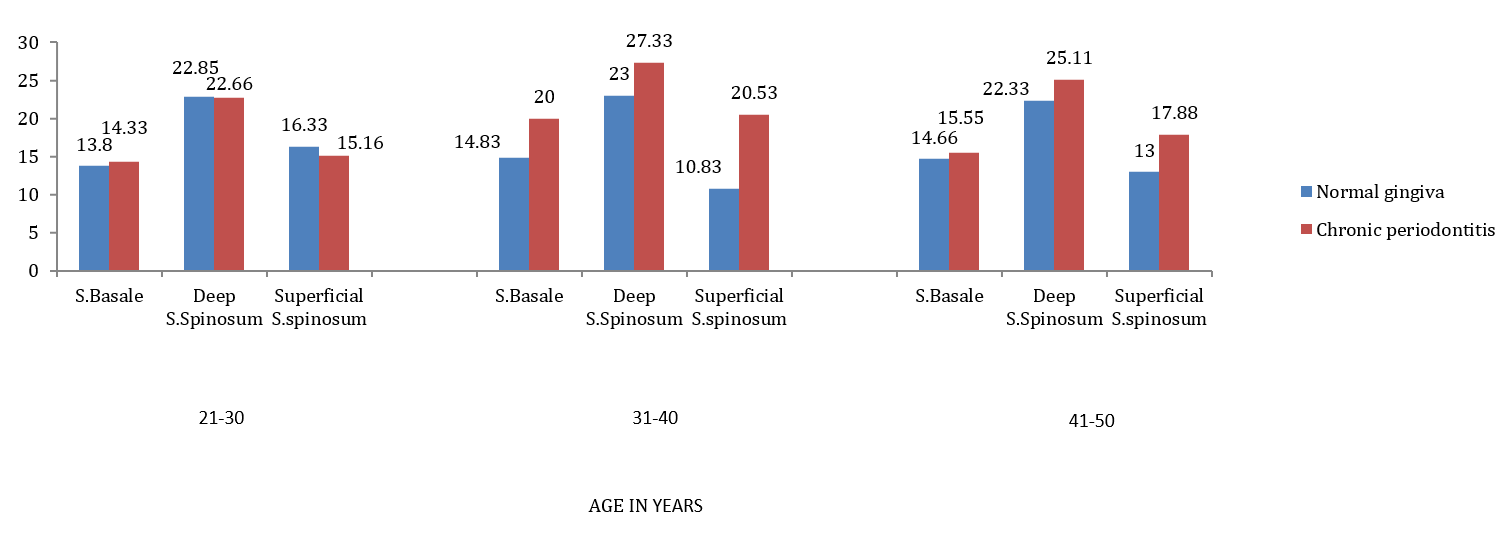
Figure 8: Comparison of Mean of Langerhans Cells with Age and Location in Subjects with Normal Gingiva and Chronic Periodontitis
Immunohistochemical expression of CD1a positive cells with varying intensities (40x)
Periodontal disease is an inflammatory process that affects the protective and supportive tissues around the tooth. These are initiated by specific invasive oral pathogens that colonize dental plaque biofilms on tooth surface [10]. Host immune response to inflammation plays a central role in disease pathogenesis. These are recognized as infectious processes that require bacterial presence and a host response and are further affected and modified by other local, environmental and genetic factors [11] (Figure 9).
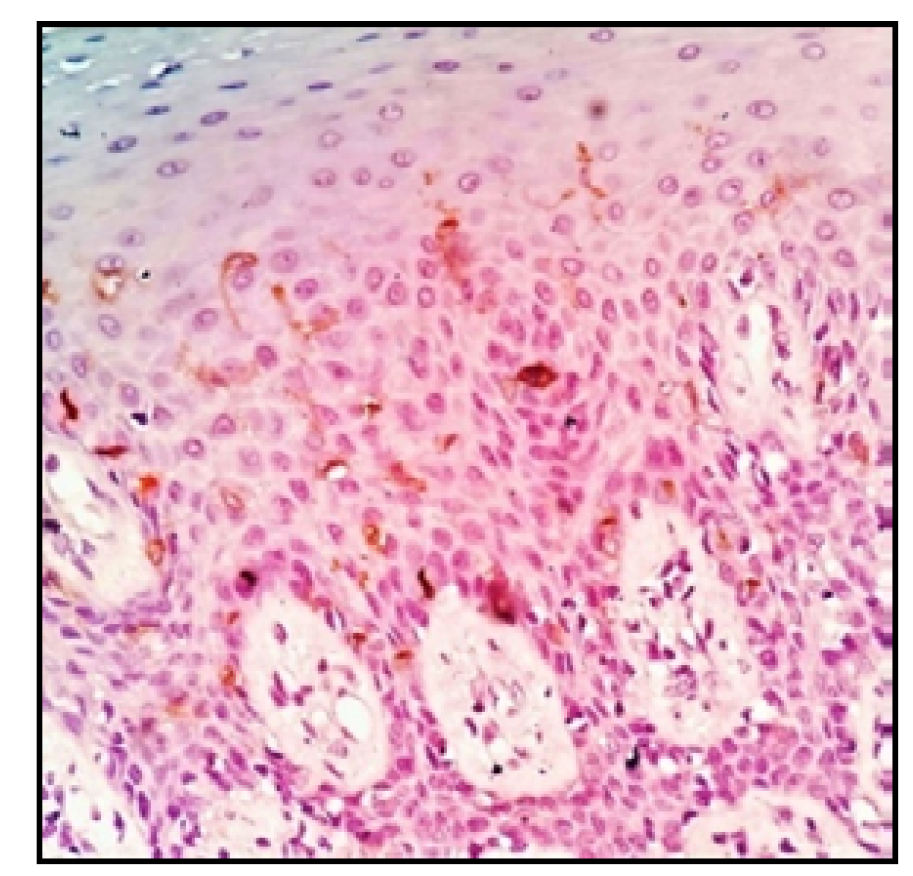
Figure 9: Study Group Expressing CD1a Positive LCs
Periodontitis is defined as an inflammatory disease of supporting tissues of teeth caused by specific microorganisms or groups of specific microorganisms, resulting in progressive destruction of the periodontal ligament and alveolar bone with periodontal pocket formation, gingival recession or both [12]. Gingivitis is the marginal tissue inflammation which is usually caused by bacterial plaque accumulation on the tooth surface. If left untreated, it may progress to periodontitis, which is characterized by loss of periodontal attachment support and bone resorption, eventually resulting in tooth mobility and loss [13]. In periodontal diseases such as gingivitis or periodontitis, the gingival epithelial tissue is important as a physical barrier against external pathogens [14]. Mechanisms of host response in the periodontal tissues are complex and involve numerous systems of interactions. The host inflammatory response is mediated mainly by neutrophils, monocytes/macrophages, and T and B lymphocytes. Neutrophils are the first cells to arrive at the inflammatory infiltrate [15]. The innate response involves the recognition of microbial components by Toll-like receptors (TLRs) expressed by host cells in the infected microenvironment (Figure 10).
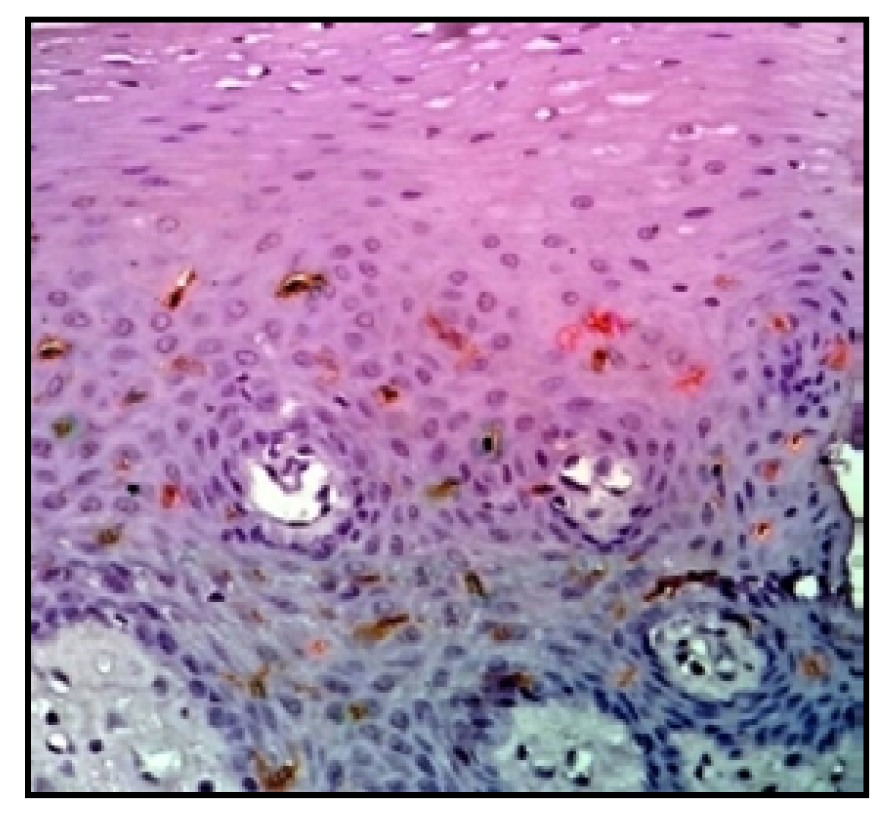
Figure 10: Increased Expression of CD1a Positive LCs in Study Group
Pathogen-associated molecular patterns are biological macromolecules produced by microbial pathogens that are recognized by receptors on mononuclear phagocytes and opsonins in serum and tissue fluids. The innate immune recognition relies on a growing number of receptors termed pattern recognition receptors that have evolved to recognize PAMPs [16]. Immature DCs are capable of capturing and processing the antigen, whereas mature DCs have increased expression of peptide major histocompatibility complex (MHC) on their surface along with increased levels of co-stimulatory molecules. This enhances the ability of mature DCs to present the antigen to T-cells and induce their activation. Apart from initiating innate immune response to PAMP, recognition of PAMP by Toll-like receptors (TLRs) allows an improved acquired immune response to pathogens [17]. When the resolution of inflammation is not achieved, antigen-presenting cells are activated by bacterial products and interact with naive T helper cells (Th0), driving their differentiation into several subsets, such as Th1, Th2, Th17, and Treg. T lymphocytes are central to adaptive immunity and provide help for B cells to generate specific antibodies. Hence the shift over of immune reaction is carried out with the help of antigen-presenting cells (APCs) which serves as a bridge between innate and adaptive immune response [18] (Figure 11).
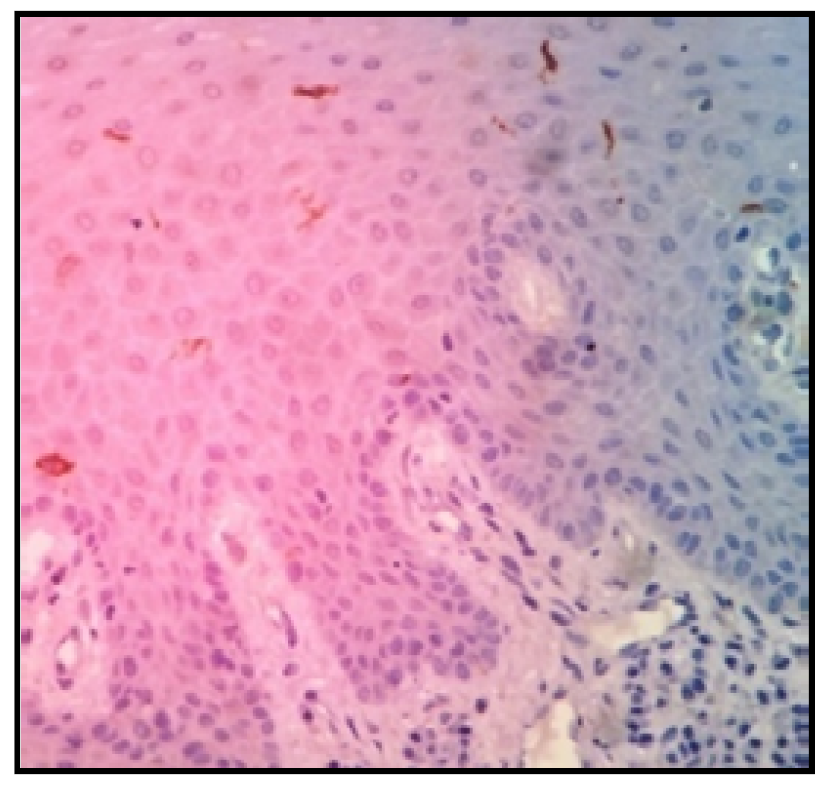
Figure 11: Decreased Expression of CD1a Positive LCs in Control Group.
One of the chief and important cells that play a major role in periodontal immune system are the dendritic cells (DCs). In fact, these cells represent a large family of antigen presenting cells that circulate throughout the blood stream and are scattered in nearly all tissues of the body. Both immature and mature forms exist; the immature forms are present in the epithelium and mature forms in the connective tissue. They are referred to as professional antigen- presenting cells’ as their principal function is to present antigens and they have the ability to induce a primary immune response in resting naive T-lymphocytes [19] (Figure 12).
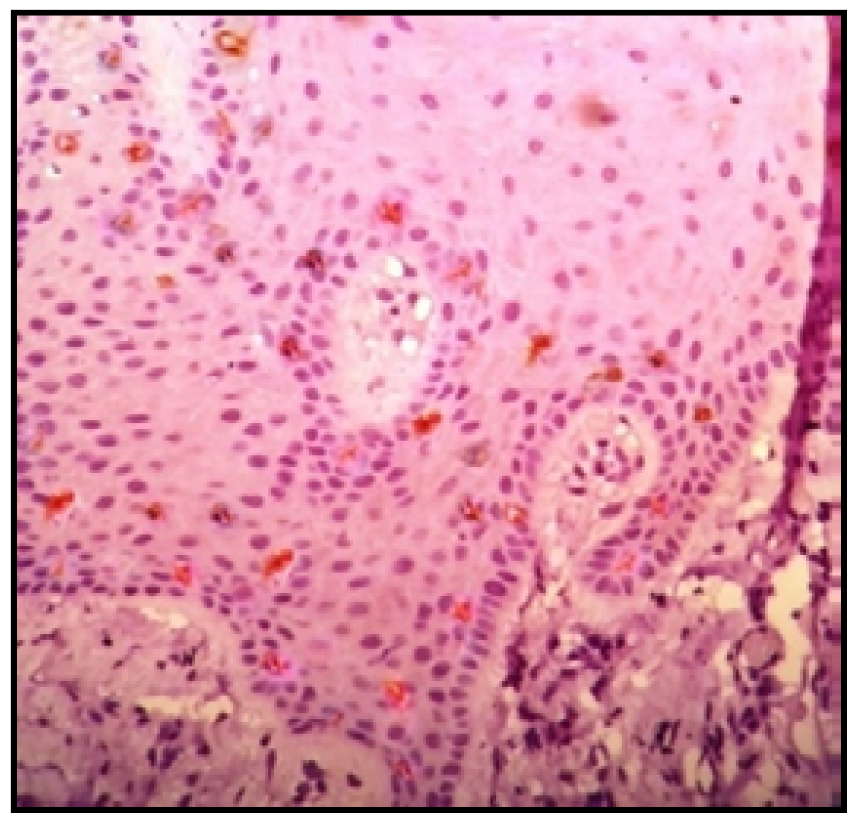
Figure 12: CD1a positive LC expression in Stratum Basale and Deep Stratum Spinosum
The term dendritic cell’ was coined by Steinman and Cohn (1973) in a description of an adherent nucleated cell from the mouse spleen [20]. Evidence demonstrated that DCs can arise from monocytes [21], suggesting that they share common progenitors with osteoclast precursors [22]. Dendritic cells exist in all lymphoid and most non-lymphoid tissues and they are capable of capturing antigen, processing, and presenting them on the cell surface along with appropriate co-stimulatory molecules. They also play a role in maintaining B-cell function and recall responses. Therefore, these cells play a unique role in the innate system by serving a bridge to adaptive immune response [23]. Langerhans cells constitute a subset of DCs that capture antigens in their immature state in the epithelium, and as they get differentiated into DCs, they undergo phenotypic changes that facilitate migration towards lymphoid organs, findings suggest that monocytes must seed LC pool for their renewal in response to stress responses in vivo [24]. It has been determined that a circulating monocyte population is required for the renewal of LCs in response to stress or inflammation. LCs are considered the best characterized immature DCs that are present above the basal layer of epithelial cells in the skin, oral, nasal, esophageal, pulmonary, vaginal, and rectal mucosa [25].
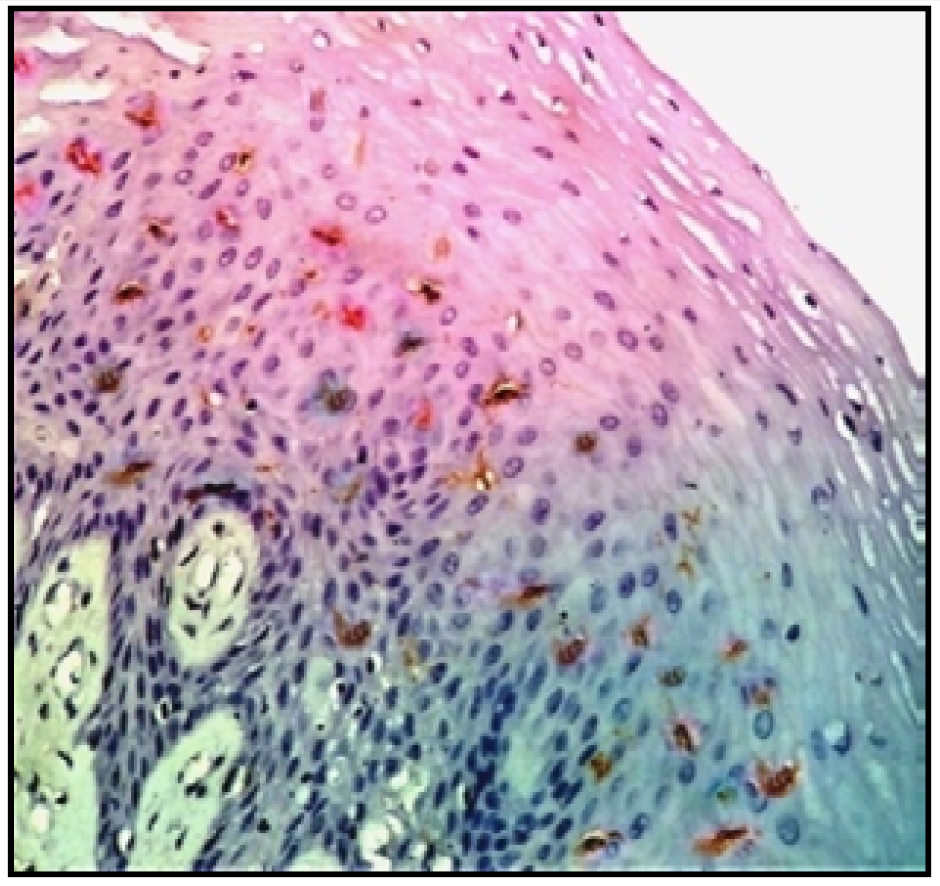
Figure 13: CD1a positive LC expression in Superficial Stratum Spinosum.
In hematoxylin and eosin histological sections LCs are seen as 'clear cells' in suprabasal layers of mucous membranes. The LCs can be visualized as cells with their bodies generally in the middle portion of stratum spinosum. Delicate dendritic processes can often be observed extending to the level of stratum corneum. Their cytoplasmic processes are found in stratum corneum and usually directed towards epithelial surface [26]. The actual sites of cellular enzymatic activity in LCs can be demonstrated by enzyme histochemical techniques like ATPase, which is an excellent method for the identification of human LCs. Other enzymes used are adenosinediphosphatase (ADPase), 5 nucleotidases and amino-peptidases. One of the first techniques employed to demonstrate LCs was the metal impregnation staining technique using heavy metals such as gold chloride, osmium iodide or zinc osmium iodide and uranyl acetate–lead staining. Zinc osmium iodide, although gives good staining, also stains keratinocytes and melanocytes. On Electron microscopic examination LCs exhibit a cleaved or folded nucleus and no tonofilaments or desmosomes. The Birbeck granules are characteristically present in their cytoplasm, which have a three-dimensional profile of a disc. These granules show a vesicle at one end and sometimes at both ends. In cross sections, the granule with vesicle at one end shows a characteristic appearance, which is termed as 'tennis racket' appearance [27].
Markers for LCs were initially non-specific like, ecto-ATPase, and Birbeck granules. Specific markers such as CD1a [28], E-Cadherin [29], and Langerin [30] are now known that can distinguish LCs from other DCs subsets. Among all the markers used, CD1a immunolabeling is considered to be one of the reliable method to identify the human LCs. CD1a is a transmembrane glycoprotein that are encoded by a CD1a gene located on chromosome1. They mediate the presentation of primarily lipid and glycolipid antigens of microbial origin to T cells [9]. Hence the present study was formulated to determine the presence and distribution of LCs of epithelium in gingival tissue samples derived from healthy controls and chronic periodontitis affected human subjects using CD1a monoclonal antibody which is specific to LCs for quantitative assessment (Figure 11).
The subjects in the control group were systemically healthy with no clinical signs of gingival inflammation, no clinical attachment loss and no radiographic evidence of bone loss. whereas for chronic periodontitis group patients exhibited clinical evidence of gingivitis with attachment loss ≥ 4mm, with radiographic evidence of bone loss. In the present study the patients with chronic periodontitis were in the age group of 21 – 50 years with mean age group between 31-40 years and there was male predominance. Shaju conducted a review on various epidemiological studies conducted in India to determine the prevalence of periodontitis, the predominant age group was found to be 35-44 years. According to Eke PIe periodontitis was more prevalent in people >65 years of age in USA. According to various studies in the literature prevalence of periodontitis might vary depending on geographical location, awareness of dental health among patients and several other factors which affects the oral health [31].
The results of the present study showed decreased CD1a positivity of LCs in both study and control groups with increasing age. These findings were in agreement with a study conducted by Zavala WD et al. [32] where they found an age-related decrease in LC density in the human gingival epithelium. This is due to the fact that as the age advances the immune system weakens, that might be related to a decrease in number or reactivity of immune cells such as lymphocytes or dendritic cells (Langerhans cells).
In the present study there is significant increase in the number of CD1a positive cells in chronic periodontitis when compared to the control group. Anjanaet evaluated the presence and distribution of CD1a in healthy gingival and chronic periodontitis in human subjects. They found an increased expression of CD1a in periodontitis affected gingival tissues compared with healthy gingiva which was in accordance to our study. This was consistent with previous studies. Newcomb and Walsh stated that LCs in the gingival epithelium are very responsive to the accumulation of bacterial plaque and they migrate to the inflamed site in large numbers during periodontal diseases. LCs increase or decrease in number may result from different bacterial antigens eliciting different responses or may reflect different responses to similar plaque antigens penetrating the surface of oral epithelium. This indicated that the LCs responded to external stimulus, most likely plaque antigens diffusing through the epithelium [33].
Contrasting results were observed by Seguier S, in their study which was performed to evaluate the Immunohistological and morphometric analysis of intra- epithelial lymphocytes and Langerhans cells in healthy and diseased human gingival tissues. They observed decrease in LCs number in both gingivitis and periodontitis when compared to healthy gingiva. This disparity is likely, due to a number of variables, including the quality of the tissue samples, the method of histomorphometry, the area of the gingiva being analyzed (pocket, junctional, oral, sulcular epithelia), and the ‘time window’ of sampling.
In the present study CD1a positive LCs showed focal distribution pattern in both study and control group with mean positive cells 27.33±1.40 and 23.00±5.40 respectively. Although the difference in number of mean positive cells for both groups in deep spinosum was statistically insignificant, there is increase in the number of mean positive cells in deep spinous layer in study group when compared to control group. Mild intensity of staining was observed in control group whereas study group showed moderate staining intensity. The difference in the intensity might be related to the chronicity of the lesion and several factors such as stage of disease at which sample was collected, method and solution used for antigen retrieval and the marker used for the procedure.
The demographic and clinical details observed in the study were in accordance with previous literature. All the cases in study and control group showed positive immunostaining for CD1a. The mean positive cells for CD1a were more in study group when compared to control group. Focal pattern of staining was observed in both study and control groups. Immunopositive cells were predominantly observed in deep spinosum in study group and in case of control group predominantly seen in superficial spinosum. The intensity of staining was variable from mild to moderate in study groups and predominantly mild in control group. Significant increased expression of mean of Langerhans cells and staining intensity in the study group when compared to that of the control group suggest that there is an increased host immune response in study group.
Newman, F.G. and F.A. Carranza. Carranza’s Clinical Periodontology. 11th ed., Elsevier India Pvt. Ltd., 2012, pp. 160–162.
Pari, A. et al. “Gingival diseases in childhood—A review.” Journal of Clinical and Diagnostic Research, vol. 8, no. 10, 2014, pp. ZE01–ZE04.
Bartold, P.M. and T.E. Van Dyke. “Periodontitis: A host-mediated disruption of microbial homeostasis.” Periodontology 2000, vol. 62, no. 1, 2013, pp. 203–217.
Belkaid, Y. and T. W. Hand. “Role of the microbiota in immunity and inflammation.” Cell, vol. 157, no. 1, 2014, pp. 121–141.
Jaitley, S. and T. Saraswathi. “Pathophysiology of langerhans cells.” Journal of Oral and Maxillofacial Pathology, vol. 16, no. 2, 2012, pp. 239–244.
et al. “In vivo maturation and migration of dendritic cells.” Immunology, vol. 102, no. 3, 2001, pp. 255–262.
et al. “Lipid presentation by human cd1 molecules and the diverse t-cell populations that respond to them.” Current Opinion in Immunology, vol. 26, 2013, pp. 1–6.
Mizumoto, N. and A. Takashima. “CD1a and langerin: Acting as more than langerhans cell markers.” Journal of Clinical Investigation, vol. 113, no. 5, 2004, pp. 658–660.
Jaitley, S. et al. “Immunohistochemical analysis of langerhans cells in chronic gingivitis using anti-cd1a antibody.” Dental Research Journal, vol. 11, no. 2, 2014, pp. 173–179.
Saini, R. et al. “Periodontitis, a true infection.” Journal of Global Infectious Diseases, vol. 1, no. 2, July 2009, pp. 149–150.
Saini, R. et al. “Periodontitis and psychological stress: A Dental View.” Indian Psychiatry Journal, vol. 19, no. 1, January 2010, pp. 66–67.
Lang, N. P. et al. “Gingivitis as a risk factor in periodontal disease.” Journal of Clinical Periodontology, vol. 36, suppl. 10, July 2009, pp. 3–8.
Groeger, S. E. and J. Meyle. “Epithelial barrier and oral bacterial infection.” Periodontology 2000, vol. 69, no. 1, October 2015, pp. 46–67.
Silva, N. et al. “Host response mechanisms in periodontal diseases.” Journal of Applied Oral Science, vol. 23, no. 3, May–June 2015, pp. 329–355.
Male, D. et al. Immunology. 7th ed., Elsevier, 2006. Wilson, N.S., et al. “Dendritic Cells Constitutively Present Self Antigens in Vivo.” Blood, vol. 103, no. 6, March 2004, pp. 2187–2195.
Okoye, I. S. and M. S. Wilson. “CD4+ t helper 2 cells—microbial triggers, differentiation requirements and effector functions.” Immunology, vol. 134, no. 4, December 2011, pp. 368–377.
Nair, S. et al. “Isolation and generation of human dendritic cells.” Current Protocols in Immunology, November 2012, Chapter 7, Unit 7.32.
Servet-Delprat, C. et al. “Flt3+ macrophage precursors commit sequentially to osteoclasts, dendritic cells and microglia.” BMC Immunology, vol. 3, October 2002, p. 15.
Miyamoto, T. et al. “Bifurcation of osteoclasts and dendritic cells from common progenitors.” Blood, vol. 98, no. 8, October 2001, pp. 2544–2554.
Wieder, E. Dendritic Cells: A Basic Review. International Society for Cellular Therapy, 2003.
Ginhoux, F. et al. “Langerhans cells arise from monocytes in vivo.” Nature Immunology, vol. 7, no. 3, March 2006, pp. 265–273.
Girolomoni, G. et al. “Langerhans cells: Still a fundamental paradigm.” Trends in Immunology, vol. 23, 2002, pp. 6–8.
Snehanjan, S. and A. Ritesh. “An insight into the origin, distribution, and techniques of demonstration of langerhans cells.” SRM Journal of Research in Dental Sciences, vol. 8, no. 4, 2017, pp. 162.
Fithian, E. et al. “Reactivity of langerhans cells with hybridoma antibody.” Proceedings of the National Academy of Sciences USA, vol. 78, 1981, pp. 2541–2544.
Tang, A. et al. “Adhesion of epidermal langerhans cells to keratinocytes mediated by e-cadherin.” Nature, vol. 361, 1993, pp. 82–85.
Valladeau, J. et al. “The monoclonal antibody dcgm4 recognizes langerin.” European Journal of Immunology, vol. 29, 1999, pp. 2695–2704.
Shaju, J. P. et al. “Prevalence of periodontitis in the Indian population: A literature review.” Journal of Indian Society of Periodontology, vol. 15, no. 1, January 2011, pp. 29–34.
Eke, P. I. et al. “Prevalence of periodontitis in adults in the United States: 2009 and 2010.” Journal of Dental Research, vol. 91, no. 10, October 2012, pp. 914–920.
Nazir, M. A. “Prevalence of periodontal disease, its association with systemic diseases and prevention.” International Journal of Health Sciences, vol. 11, no. 2, April–June 2017, pp. 72–80.
Zavala, W. D. and J. C. Cavicchia. “Deterioration of the langerhans cell network of the human gingival epithelium with aging.” Archives of Oral Biology, vol. 51, 2006, pp. 1150–1155.
Walsh, L. J. et al. “Oral mucosal langerhans cells express dr and dq antigens.” Journal of Dental Research, vol. 65, 1986, pp. 390–393.
Ganguly, D. et al. “Granulocyte-macrophage colony-stimulating factor drives monocytes to interleukin-10-producing myeloid cells.” Immunology, vol. 121, no. 4, August 2007, pp. 499–507.
Aquino, A. et al. “Exogenous control of the expression of group i cd1 molecules.” Clinical and Developmental Immunology, vol. 2011, 2011, Article ID 790460.
