
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Background: Swallowed foreign bodies are not uncommon in a typical ORL practice and could be wrought with a lot of challenges in the management. This study is therefore to determine the pattern, presentation and outline their management and challenges encountered. Methodology: A retrospective review of all patients diagnosed of foreign body ingestion seen in the ENT surgery department of UPTH within the period of 2016 to 2020. The patients’ records, clinic, ward and theatre register were the source of the data. The biodata, presenting complaints, management and outcome were collected and analysed. Diagnosis was made on the basis of history, clinical findings, radiological evaluation and confirmed at surgery. Results: There was a total of 32 subjects; 19 males and 13 females. The age 1-10 years were the most affected; 46.9%. Fish bone was the commonest object and was seen both in children and adults while dentures were the second commonest and found only in adults. About 31.3% of the foreign bodies were seen as radiopaque on x-ray while 17.5% were diagnosed based on presence of soft signs. .Most had emergency oesophagoscopy; 87.5%. Failed oesophagoscopy was recorded in 3.1%. Conclusion:Swallowed foreign body is commoner in children and males are more affected. Fish bone and dentures are the objects commonly swallowed. While dentures is seen more in adults, toy parts, button batteries and other small objects are commonly seen in children
In about 80-90 percent of cases, swallowed foreign body will pass straight down the gastrointestinal tract however; a few could get stuck in the oesophagus with possibility of complications. It is documented that in the United States of America, about 100,000 cases of oesophageal foreign bodies are seen annually with a mortality of around 1500 recorded [1,2].
The oesophagus has some known anatomical constrictions and it is known that foreign bodies can get impacted or stuck at these constrictions. Most of the foreign bodies are said to be stuck in the first constriction; the cricopharyngeal junction[3]. Swallowed foreign body is seen mainly in children, the elderly and the mentally challenged. It is said to occur more in children aged 6months to 6years with a peak from 6months to 3years[4]. it is also known that in children majority of the objects swallowed are inorganic ranging from coins, toy parts to button batteries. While in adults, it is mainly of organic origin relating with food example fish and chicken bone and are often accidental[5,6]. There are factors that could lead to accidental swallow of foreign body in an adult, these are poor vision, hurried feeding, addiction or intoxication and long worn dentures [7,8] Dentures swallowed in adults are often because they are ill fitting and has been worn for a long time[9]. Decreased palatal sensitivity in the wearers and poor dental follow up has also been implicated in swallowed dentures [9,10]. The presentations seen in these patients are dependent on the size, site of impaction and the time interval between incident and presentation to the hospital. Commonly documented features include; dysphagia, drooling, vomiting [11-13]. Some could be asymptomatic and discovered on endoscopy [14] children could present with nonspecific symptoms making diagnosis a challenge if ingestion was not witnessed. In about 40% of children, swallowed foreign bodies maybe asymptomatic[2].
The greatest fear in oesophageal foreign body is in the ingestion of sharp objects for this could destroy the wall of the oesophagus with resultant complications of mediastinitis which can be fatal and more so in children[3]. It is known that majority of the swallowed foreign bodies can easily be removed, however serious complications can also arise such as perforations, tracheoesophageal fistula and death [15,16]. Therefore swallowed foreign bodies can be associated with a high rate of morbidity and mortality[17]. it is therefore important that prompt diagnosis be made especially in children so as to prevent increase in morbidity and mortality[18]. Radiological investigations are very paramount in making most of this diagnosis clinically. Plain chest x-rays and sometimes barium swallow are the commonly employed form of investigations especially in poor resource regions[19]. However the diagnostic tool of choice in this era remains computed tomogram scan of the area. An added advantage is the 3D type that is obtainable in more developed climes[20]. it is known that the first challenge in the management is that of making accurate diagnosis of ingestion unless it was witnessed. In our environment however most diagnosis is made with plain chest and lateral soft tissue of the neck x-ray and rarely computed tomograms. This study therefore looks at the pattern of swallowed foreign bodies, their presentations and challenges of management in UPTH.
A retrospective review of all patients diagnosed of foreign body ingestion seen in the ENT surgery department of UPTH within the period of 2016 to 2020. The patients’ records, clinic, ward and theatre register were the source of data. The biodata, presenting complaints, management and outcome were collected and analysed. Diagnosis was made on the basis of history, clinical findings and radiological evaluation and was confirmed at surgery.
Data collected were analysed using IBM SPSS version 20 and results shown with statistical tables and figures. Frequencies and proportions were used to summarize categorical variables while numerical variables employed mean± standard deviation, and median/ranges. Differences in proportions were compared using Chi square test. A p-value of less than 0.05 was considered statistically significant.
The study involved 32 subjects comprising of 19males and 13 females giving a ratio of 1.4:1. The age ranged from 9mths to 70yrs with a mean age of 22.94+/-23.1years. The age range 1-10 years were the most affected with 46.9% followed by age 31-40years with 18.8% table 1 The commonest presenting complaints was odynophagia seen in 41.8% followed by drooling(25.45%) . respiratory distress was seen in some very young children. Table 2 majority of the subjects presented for treatment within the first 3 days and 7-13 days of the incident. Figure1 Radiologic investigation showed that 31.3% of the objects were radio opaque and could be seen on the x-ray while most though not radiopaque therefore not seen ,the presence were inferred by presence of soft signs such as air oesophagogram in n= 17(53.1% ) and in n= 5(15.6%) there was no sign of any foreign body. Figure2. Distribution of foreign body types showed fish bone as the most commonly swallowed foreign body (34.4%) followed by dentures in 21.9%, plastic(toy parts) were seen in 18.8% .Table 3. The age distribution of swallowed objects showed that fish bone was seen both in children and adults unlike dentures that was seen only in adults especially age 61-70 years. Other objects such as button batteries, clips and toy parts were seen only in children 1-10years. Difference was not however statistically significant. Table4 Most of the patients had emergency rigid oesophagoscopy carried out (87.5%). There was 1 failed attempt at removal that required open surgery for the removal of the foreign body. In addition, there was a patient with suspected perforation that after the removal had to have a nasogastric tube passed to forestall further complications. Table5. Correlating radiologic finding and treatment showed that most of the patients including those in whom the x-ray showed no foreign body were all scoped. All the patients had foreign body recovered following surgery. There was no statistically significant difference in the radiologic findings and the treatment offered the subjects. Table6. The subjects all had emergency intervention despite the time of presentation, most of the subjects had presented for treatment by the end of 2 weeks of the incident. However, the patient that had failed retrieval by oesophagoscopy and had open surgery, presented at about 13days after incident while the subject with suspected perforation had presented within 3days of incident. This was found not to be statistically significant. Table
Table 1: Demographic Distribution of Subjects
Frequency (n=32) | Percent (%) | |
SEX | ||
Male | 19 | 59.4 |
Female | 13 | 40.6 |
| Age group (years) | ||
1 to 10 | 15 | 46.9 |
11 to 20 | 2 | 6.3 |
21 - 30 | 2 | 6.3 |
31 - 40 | 6 | 18.8 |
41 - 50 | 3 | 9.4 |
51 - 60 | 1 | 3.1 |
61 - 70 | 3 | 9.4 |
Table 2: Distribution of Symptoms
Symptoms | Frequency | Percent (%) |
Odynophagia | 23 | 41.82 |
Drooling | 14 | 25.45 |
Dysphagia | 9 | 16.36 |
Refusal to feed | 5 | 9.09 |
Respiratory distress | 3 | 5.45 |
Perforation | 1 | 1.82 |
Total | 55 | 100.00 |
* Multiple responses apply
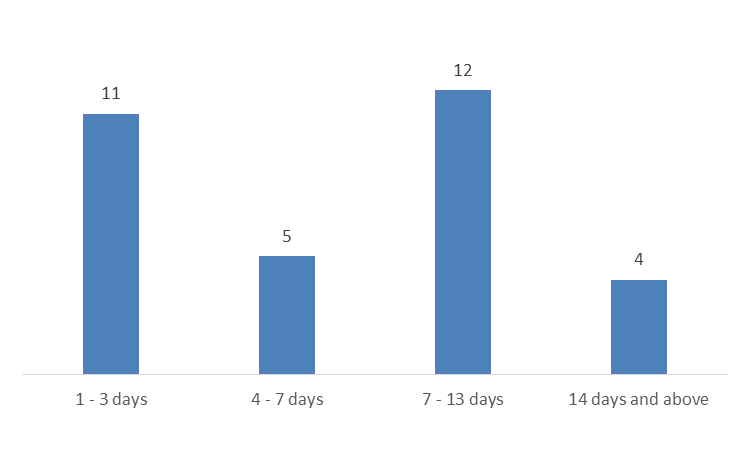
Figure 1: Distribution of No. of days before presenting for treatment
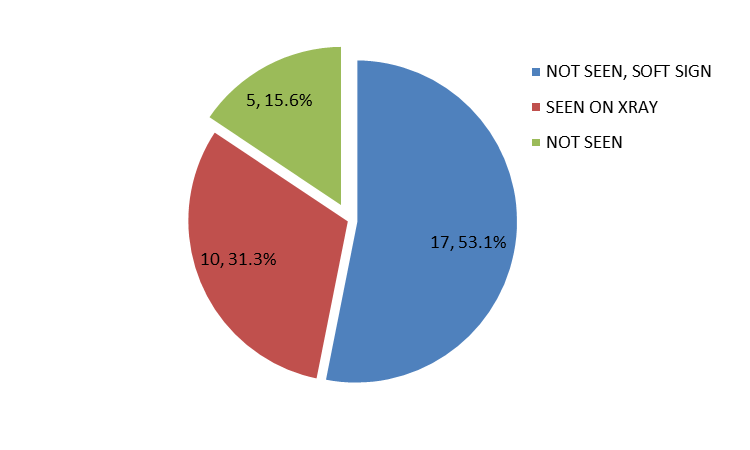
Figure 2: Distribution of X-ray findings
Table3:Distribution of foreign bodies
Type of Foreign Body | Frequency | Percent |
Fish bone | 11 | 34.4 |
Dentures | 7 | 21.9 |
Plastics(toy parts) | 6 | 18.8 |
Button battery | 2 | 6.3 |
Clip pin | 2 | 6.3 |
Bottle cork | 1 | 3.1 |
Meat bolus | 1 | 3.1 |
Nail | 1 | 3.1 |
Shoe buckle | 1 | 3.1 |
Total | 32 | 100 |
Table 4: Distribution of foreign body according to age
Foreign Bodies | Age – groups (years) | Chi-square (p-value) | ||||||
1 to 10 | 11 to 20 | 21 - 30 | 31 - 40 | 41 - 50 | 51 - 60 | 61 - 70 | ||
Bottle cork | 1(6.67) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 64.74 (0.054)** |
Button battery | 2(13.33) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Clip pin | 2(13.33) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Dentures | 0(0.00) | 0(0.00) | 0(0.00) | 2(33.33) | 1(33.33) | 1(100.00) | 3(100.00) | |
Fish bone | 3(20.00) | 1(50.00) | 1(50.00) | 4(66.67) | 2(66.67) | 0(0.00) | 0(0.00) | |
Meat bolus | 0(0.00) | 0(0.00) | 1(50.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Nail | 0(0.00) | 1(50.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Plastic(toy parts) | 6(40.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Shoe buckle | 1(6.67) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | 0(0.00) | |
Total | 15(100.00) | 2(100.00) | 2(100.00) | 6(100.00) | 3(100.00) | 1(100.00) | 3(100.00) | |
**Distribution is not statistically significant (p >0.05)
Table 5: Distribution of treatments
Frequency | Percent | |
Emergency rigid oesophagoscopy | 28 | 87.5 |
Hypopharyngoscopy | 2 | 6.3 |
Failed oesophagoscopy, oesophagotomy done | 1 | 3.1 |
Suspected perforation therefore Ng tube passed after oesophagoscopy | 1 | 3.1 |
Total | 32 | 100 |
Table 6: Cross tabulation of x-ray findings and treatment
Treatment modality | Not seen | Not seen, soft sign | Seen on x-ray | Chi-square (p-value) |
Emergency rigid oesophagoscopy | 5(100.00) | 16(94.12) | 7(70.00) | 5.46 (0.486)** |
Failed oesophagoscopy, oesophagotomy done | 0(0.00) | 0(0.00) | 1(10.00) | |
Hypopharyngoscopy | 0(0.00) | 1(5.88) | 1(10.00) | |
Suspected perforation therefore Ng tube passed after oesophagoscopy | 0(0.00) | 0(0.00) | 1(10.00) | |
Total | 5(100.00) | 17(100.00) | 10(100.00) |
|
**Not statistically significant (p > 0.05)
Table 7: Distribution of Type of treatment by the duration before presentation
Treatment | 1 - 3 days | 4 - 7 days | 8 - 13 days | ≥14 days | Chi-square (p-value) |
Emergency rigid oesophagoscopy | 9(81.82) | 4(80.00) | 11(91.67) | 4(100.00) | |
Failed oesophagoscopy, oesophagotomy done | 0(0.00) | 0(0.00) | 1(8.33) | 0(0.00) | |
Hypopharyngoscopy | 1(9.09) | 1(20.00) | 0(0.00) | 0(0.00) | 6.39 (0.699)** |
Suspected perforation therefore Ng tube passed after oesophagoscopy | 1(9.09) | 0(0.00) | 0(0.00) | 0(0.00) | |
Total | 11(100.00) | 5(100.00) | 12(100.00) | 4(100.00) |
**distribution is not statistically significant (p >0.05)
The predominance of males in epidemiology of swallowed foreign bodies is already documented as also observed in this study [21,19,22] While in contrast some had found females more affected [23]The finding of children (ages 1-10 years) being more affected agrees with that already documented [24,23,25,18]. It is of note however that the next commonly affected age group was not the elderly but adults in ages 31 to 40 years. This we could not readily explain. The commonest presenting complaints were odynophagia, drooling and dysphagia. It is known that the presentation actually depends on the size and therefore the locations of the foreign bodies in this study majority of the foreign bodies were located around the cricopharyngeal junction. Hence the above common symptoms similar to other works [26,11,12, 5,27]. In the very young children there was respiratory distress and the foreign bodies in these cases were found to be just below the hypopharynx resulting in respiratory compromise in addition. These had hypopharyngosopy and removal of foreign body.
The percentage of the objects seen on the plain x-ray was 31.3% however in addition, 53. 1% though not radiopaque, was identified by presence of soft signs; air oesophagogram, increase in the prevertebral soft tissue shadow, all these can indicate presence of foreign body in plain neck and chest radiograph. Therefore plain radiograph was found to be diagnostic in 84.4% but failed in 15.6% and these were found to be fishbone. These finding were similar to that of other researchers [19,28]. Ngan et al found plain x ray negative for fishbone with a sensitivity of only 32%[29]. There was no use of contrast studies such as barium swallow due to possibility of aspiration and making it more difficult to see and remove the foreign body. Fish bone was found to be the commonest object swallowed in contrast to some studies that found it to be the second commonest.[18,30] similarly, toy parts, button batteries, clips were all found only in children [18] while dentures were seen in adults [18,9]. In the present study in contrast to other studies, coins was not seen as foreign body possibly due to the fact that coins are no longer in use in the country unlike in other countries [19,30].
Almost all the subjects had endoscopic (rigid) removal carried out similar to other studies.[19]The subjects with negative x- ray findings also had oesophagoscopy carried out due to clinical findings despite the radiologic diagnosis of no foreign body seen. It is known that the diagnosis and therefore management of swallowed foreign bodies depends often on the history and clinical findings [31,32]. Emergency rigid oesophagoscopy was commonly done in these subjects however some of the objects presented a challenge at removal. The button batteries though easily diagnosed on the x-ray tended to give rise to complications. The patient with suspected perforation had swallowed button battery and was initially managed in a peripheral center, therefore had to be managed as such after the endoscopy. This patient on follow up had a tracheoesophageal fistula which was managed conservatively. Singh et al in their study recorded tracheoesophageal fistula in 1.2% of their subjects[19]. There was a case of failed retrieval in a 12 year old that swallowed a bent nail. It was a sharp object and because it was bent, though it could be seen in the second part of the oesophagus during the oesophagoscopy, could not be removed easily without perforating the oesophagus hence endoscopic removal was abandoned and a cervical oesphagotomy was done with the cardiothoracic team. The challenge with the denture was often due to the large abutment especially when it is for more than a tooth and the color being difficult to differentiate from the mucosa.
There was no statistically significant difference found in the form or result of treatment in relation to the time of presentation in the present study, even though majority presented for treatment in less than two weeks of incident. In contrast, some other researchers found complications in delays in treatment for more than 12hours after incident[19]. Therefore swallowed foreign body can pose a challenge both in diagnosis and management especially in children.
Swallowed foreign body is commoner in children and males are more affected. Fish bone and dentures are the objects commonly swallowed. While dentures is seen more in adults, toy parts, button batteries and other small objects are commonly seen in children. The type , size of foreign body and when it is sharp can pose a challenge to management and outcome.
None declared
No funding sources
The study was approved by the University Of Port Harcourt Teaching Hospital Port Harcourt, Rivers State, Nigeria.
Hesham, H., & Kader, A. (2010). Foreign body ingestion: children like to put objects in their mouth. World Journal of Paediatrics. 6(4), 301-310
Uyemura, M.C. (2005). Foreign body ingestion in children. Am Fam Physician. 72(2), 287-292
Albrecht, P., Kotowska, M., Dziechciarz, & Radzikowski, A. (2005). Management of ingested foreign bodies in children. Pediatria Wspolczesna. 7(4), 297-301
Wyllie, R. (2006). Foreign bodies in the gastrointestinal tract, Curr Opin Pediatr .18(5), 563-564
Little, D.C., Shah, S.R., St Peter, S.D., Holcomb, G.W., Ostlie, D.J., & Snyder, C.L. (2006). Oesophageal foreign bodies in the paediatric population: our first500cases. journal of pediatric Surgery.14(5), 914-918
Bak- Romaniszyn, L., Czkwianianc, E., & Walecka-Panas, E. (2008). Foreign bodies in the alimentary tract in children. Przeglad Gastroenterologiczny. 3(4),207-211
Okeowo, P.A. (1985). Foreign bodies in pharynx and oesophagus – A10year review of patients seen in Lagos. Niger Quart 3, 46-50
Phillipps, J.J., & Patel, P. (1988). Swallowed foreign bodies. J Laryngol Otol. 102, 235-241
Nwaorgu, O.G., Onakoya, P.A., Sogebi, O.A., Kokong, D.D., & Dosumu, O.O. (2004). Esophageal impacted dentures. J Natl Med Assoc 96, 1350-1353
Baraka, A., & Bikhazi, G. (1975). Oesophageal foreign bodies, Br Med J 1, 561-563
Conners, G.P. (2005). Management of asymptomatic coin ingestion Pediatrics 116:752-753
Balci, A.E., Erens, S., & Eren, M.N. (2004). Oesophageal foreign bodies under cricopharengeal level in children: an analysis of 1116 cases. Interactive cardiovascular and thoracic Surgery.3(1), 14-18
Al- Qudah, A., Daradkeh, S., & Abu-Khalaf, M. (1998). Esophageal foreign bodies. European Journal of Cardio-Thoracic Surgery 13(5), 494-499.
Lasinski, W. (1983). Anatomia Topograficzna I Stosowana, PZWL Warsaw. Poland 1983
Cheng, W., & Tam, P.K. (1999). Foreign body ingestion in children: Experience with 1265 cases. J Pediatr Surg.34, 1472-1476
Sung, S. H., Jeon, S. W., Son, H. S., Kim, S. K., Jung, M. K., Cho, C. M., ... & Kweon, Y. O. (2011). Factors predictive of risk for complications in patients with oesophageal foreign bodies. Digestive and Liver Disease, 43(8), 632-635.
Mahafza, T.M. (2002). Extracting coins from the upper end of the oesophagus using a Magil forceps technique. Int J Pediatr Otorhinolaryngol .62, 37-39
Okhakhu, A.L., & Onyeagwara, N.C. (2018). Aerodigestive foreign bodies: Clinical profile and management. PHMJ 12(1), 37-40.
Singh, A., Bajpai, M., Panda, S.S., Chand, K., Jana, M., & Ali, A. (2014). Oesophageal foreign body in children: 15years experience in a tertiary care pediatric Centre. Afr J Pediatr Surg(serial online) 11, 238-241.
Loh, W.S., Eu, D.K., Loh, S.R., Chao, S.S. (2012). Efficacy of computed tomographic scans in the evaluation of patients with oesophageal foreign bodies. Ann Otol Rhinol Laryngol, 121, 678-681.
Onyeagwara, N.C., Okhakhu, A.L., Emokpaire, E., Ogisi, F. (2012). Dynamics in the trend of foreign bodies in ENT Practice in Nigeria. Any change? Internet J Otorhinolaryngol . 14, 2.
Gupta, P., & Jain, A.K. (2014). Foreign bodies in upper aero-digestive tract: A clinical study. Int J Res Med Sci 2:886-891
Kay, M., & Wyllie, R. (2005). Pediatric foreign bodies and their management. Current Gastroenterology Reports 7(3), 212-218
Rybojad, B., Niedzielski, G., Niedzielski, A., Rudnicka-Drozak, E., & Rybojad, P. (2012). Esophageal foreign bodies in Pediatric patients: A thirteen year retrospective study. The Scientific World Journal Article ID102642; 6pages 2012. https://doi.org/10.1100/2012/102642
Chen, M.K., & Beierle, E.A. (2001). Gastrointestinal foreign bodies Pediatr Ann. 30:736-742
Athanassiadi, K., Gerazounis, M., Metaxas, E., & Kalantzi, N. (2002). Management of esophageal foreign bodies: a retrospective review of 400cases. European Journal of Cardio-Thoracic Surgery 21(4), 653-656.
Asif, M., Haroon, T., Khan, Z., Muhommadu, R., Malik, S., & Khan, F. (2013). Foreign body in oesophagus: types and sites of impaction. Gomal J Med Sci. 11, 163-166
Mosca, S., Manes, G., Martino, R., Amitrano, L., Bottino, V., Bove, A., ... & Balzano, A. (2001). Endoscopic management of foreign bodies in the upper gastrointestinal tract: report on a series of 414 adult patients. Endoscopy, 33(08), 692-696.
Ngan, J.H., Fok, P.J., Lai, E.C., Branicki, F.J., & Wong, J. (1990). A prospective study on fish bone ingestion, Experience of 358 patients Ann Surg. 211(4), 459-462
Denny, W., Ahmad, N., Dillard, B., & Nowicki, M.J. (2012) Children will eat the strangest things: a 10-year retrospective analysis of foreign body and caustic ingestions from a single academic center. Pediatr Emerg Care, 28(8), 731-734
Chiu, Y.A., Hou, S.K., Chen, S.C., How, C.K., Lam, C., & Kao, W.F. (2012). Diagnosis and endoscopic management of upper gastrointestinal foreign bodies. Am J Med Sci. 343, 192-195
Ikenberry, S. O., Jue, T. L., Anderson, M. A., Appalaneni, V., Banerjee, S., Ben-Menachem, T., ... & Dominitz, J. A. (2011). Management of ingested foreign bodies and food impactions. Gastrointestinal endoscopy, 73(6), 1085-1091.
