
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Background: Acute myeloid leukaemia (AML) is a heterogeneous haematological malignancy characterized by the proliferation of immature myeloid cells in the bone marrow, typically exceeding 20-30% blasts. According to the French-American-British (FAB) classification, AML is divided into eight subtypes (M0-M7) based on morphological and cytochemical features. This study aimed to evaluate alterations in complete blood count (CBC) parameters in adult AML patients and to analyse the distribution patterns of FAB subtypes over time. Materials and Methods: A retrospective review was conducted on 521 adult patients diagnosed with AML and admitted to Baghdad Teaching Hospital, Medical City, between January 2000 and December 2011. After excluding 53 cases due to relapse, age below 15 years, incomplete data, prior haematological disorders or unclassified AML, 468 patients were included in the final analysis. Clinical history, physical examination findings and laboratory investigations were documented. Diagnostic evaluation included CBC, differential white blood cell count, peripheral blood smear, bone marrow examination with blast percentage estimation and special cytochemical stains to confirm AML subtype classification. Results: Among the 468 patients, the most frequent subtype was AML-M3 (28.2%), followed by M2 (26.3%), M1 (19.7%), M5 (15%), M4 (7.9%), M6 (1.9%) and M7 (1%). AML was most prevalent in the 15-24-year age group, with a gradual decline in frequency in older age groups. The male-to-female ratio was approximately 1:1.05, indicating no significant gender predominance. Haematological findings revealed anaemia (haemoglobin <30%) in 95.7% of patients, leukopenia in 59.8% and thrombocytopenia (<150×10⁹/L) in 94.7%. Peripheral blood blasts were detected in 78% of cases, while Auer rods were present in 32.3%. Cytochemical staining (Sudan Black B) was positive in 85.6% of cases. A notable increase in AML incidence was observed in 2011, accounting for 20.5% of total cases during the study period. Conclusion: The findings demonstrate that AML-M3 and AML-M2 were the predominant subtypes in this cohort. Haematological abnormalities, particularly anaemia and thrombocytopenia, were highly prevalent. Not all patients exhibited circulating blasts, highlighting the importance of bone marrow examination for definitive diagnosis. The study underscores the need for advanced diagnostic modalities, including immunophenotyping and molecular genetic analysis, to improve classification accuracy and therapeutic outcomes. Additionally, prompt management of cytopenias and infection risk remains essential due to the high likelihood of severe infections and bleeding complications in AML patients.
The first description of a case of leukaemia in medical literature dates to 1827, when a French physician named Alfred-Armand Louis-Marie Velpeau described a 63-years old florist who developed an illness characterized by fever, weakness, urinary stones and substantial enlargement of the liver and spleen. The term "leukaemia" was coined by Rudolf Virchow, the renowned German pathologist, in 1856. In 2008, AML became the first cancer genome to be fully sequenced. The leukemic cells contained acquired mutations in several genes that had not previously been associated with the disease. Also known as acute myelogenous leukaemia, is a cancer of the myeloid line of white blood cells, characterized by the rapid proliferation of abnormal cells which accumulate in the bone marrow (BM) and interfere with the production of normal blood cells.
Most signs and symptoms of AML are due to an increased number of malignant white blood cells displacing or otherwise interfering with production of normal blood cells in the bone marrow. A lack of normal white blood cell production makes the patient susceptible to infections (although the leukemic cells themselves are derived from white blood cell precursors, but they have no infection-fighting capacity). A lack of red blood cells (anaemia) can cause fatigue, paleness and shortness of breath. A lack of platelets can lead to easy bruising or bleeding with minor trauma [1]. The early signs of AML are often non-specific and may be similar to those of influenza or other common illnesses. Some generalized symptoms include fever, fatigue, weight loss or loss of appetite, shortness of breath with exertion, pallor, easy bruising or bleeding, petechiae (flat, pin-head sized spots under the skin caused by bleeding), bone pain and joint pain and persistent or frequent infections [2]. Enlargement of the spleen may occur in AML, but it is typically mild and asymptomatic. Lymph node swelling is rare in AML (11%), in contrast to acute lymphoblastic leukaemia (40%) [3]. Some patients with AML may experience swelling of the gums because of infiltration of leukemic cells into the gum tissue. Rarely, the first sign of leukaemia may be the development of a solid leukemic mass or tumour outside the bone marrow, called a myeloid sarcoma. Occasionally, a person may show no symptoms and the leukaemia may be discovered incidentally during a routine blood examination [1,2,4].
Diagnostic Criteria for Diagnosis of AML
M0 Category Acute Myeloid Leukaemia with Minimal Evidence of Myeloid Differentiation [5-7]:
Blasts ≥30% of bone marrow nucleated cells
Blasts ≥30% of bone marrow non-erythroid cells (exclude also lymphocytes, plasma cells, macrophages and mast cells from the count) >33% of blasts positive for Sudan Black B in the BM or blasts demonstrated to be myeloblasts by immunological markers or by ultra - structural cytochemistry
M1 Category Acute Myeloid Leukaemia Without Maturation [5-7]
Blasts ≥30% of bone marrow cells
Blasts ≥90% of bone marrow non-erythroid cells
≥3% of blasts positive for peroxidase or Sudan Black B
Bone marrow maturing monocytic component (promonocytes to monocytes ≤10% of non-erythroid cells
Bone marrow maturing granulocytic component (promyelocytes to polymorphonuclear leukocytes) ≤10% of non-erythroid cells
M2 Category Acute Myeloid Leukaemia with Maturation [5-7]
Blasts ≥30% of bone marrow cells
Blasts 30-89% of bone marrow non- erythroid cells
Bone marrow maturing granulocytic component (promyelocytes to polymorphonuclear leukocytes) >10% of non-erythroid cells. 4 Bone marrow monocytic component (mesoblasts to monocytes) <20% non- erythroid cells and other criteria for M4 not met
M3 Category Acute Hyper Granular Promyelocytic Leukaemia [5-7]
The predominant cell is a highly abnormal promyelocyte. In the majority of cases blasts are fewer than 30% of bone marrow nucleated cells. The distinctive cytological features are sufficient to permit a diagnosis and cases are classified as M3 AML despite the low blast percentage. The malignant promyelocytes show usually reniform or bilobed nuclei with abnormally heavy granulation and occasional cells with bundles of Auer rods (Faggot cells).
M3V AML microgranular or hypo granular variant It is characterized by a cell with reniform, bilobed, multilobed or convoluted nucleus and either sparse fine granules or apparently agranular cytoplasm. A variable proportion of cells may have multiple Auer rods, fine dust - like granules or large oval, ellipt form or somewhat angular cytoplasmic inclusions with the same staining characteristics as primary granules.
M4 Category Acute Myelomonocytic Leukaemia [5-7]
Blasts ≥30% of bone marrow cell
Blasts ≥30% of bone marrow non- erythroid cells
Bone marrow granulocytic component (myeloblasts to polymorphonuclear leukocytes) ≥20% of non-erythroid cells
Significant monocytic component as shown by one of the following:
Bone marrow monocytic component (mesoblasts to monocytes): ≥20% of non-erythroid cells and peripheral blood monocytic component ≥5×109 /L, or
Bone marrow monocytic component (mesoblasts to monocytes): ≥20% of non-erythroid cells and confirmed by cytochemistry or increased serum or urinary lysozyme concentration*, or
Bone marrow resembling M2 but peripheral blood monocyte component ≥5×109/L and confirmed by cytochemistry or increased serum or urinary lysozyme concentration
M5 Category Acute Monoblastic/Monocytic Leukaemia (8-12)
Blasts ≥30% of bone marrow cells
Blasts ≥30% of bone marrow non- erythroid cells
Bone marrow monocytic component ≥80 % of non- erythroid cells
Acute Monoblastic Leukaemia (M5a)
Mesoblasts ≥80% of bone marrow monocytic component Acute monocytic leukaemia (M5b)
Mesoblasts <80% of bone marrow monocytic component
M6 Category Acute Erythroleukemia (11-13)
Erythroblasts ≥50% of bone marrow nucleated cells
Blasts ≥30% of bone marrow non- erythroid cells
M7 Category Acute Megakaryoblast Leukaemia (11-13)
Blasts ≥30% of bone marrow nucleated cells
Blasts demonstrated to be megakaryoblasts by immunological markers, ultrastructural examination or ultrastructural cytochemistry
Patient
This is a descriptive study done at the haematology departments of Baghdad Teaching Hospital and Teaching Laboratories of Medical City in Baghdad which receives cases from other centres. The study reviewed cases over a period of 7 years from the beginning of 2005 to the end of 2011. A total of 581 patients with AML were diagnosed, but 113 cases were excluded due to relapse, slide review, age <15y, missing information, unclassified AML, history of previous haematological disorders like myelodysplasia, chronic myeloid leukaemia aplastic anaemia and prior chemotherapy or radiotherapy.
Thus, only 468 patients who were newly diagnosed, untreated, de novo AML were included in the study. It included adult patients (15- 85 years) with no sex selection. Patients were divided according to FAB classification into eight subtypes; M1(92 cases), M2(123 cases), M3(132 cases), M4(37 cases), M5(70 cases), M6(9 cases) and M7(5 cases). The diagnosis of acute leukaemia was established according to the presence of blasts ≥20% in the peripheral blood and/or bone marrow, based on their morphology and cytochemistry.
A total of 468 patients were included in this study which is the largest sample size compared with previous studies in Iraq, 214 cases in 1991 (60), 121 cases in 1980 and 54 cases in 1993 [8]. The average number of patients per 12 months in each study is shown in Figure 1, which reveals a significant increase in the number of patients diagnosed as AML in the current study compared with studies before 1993.
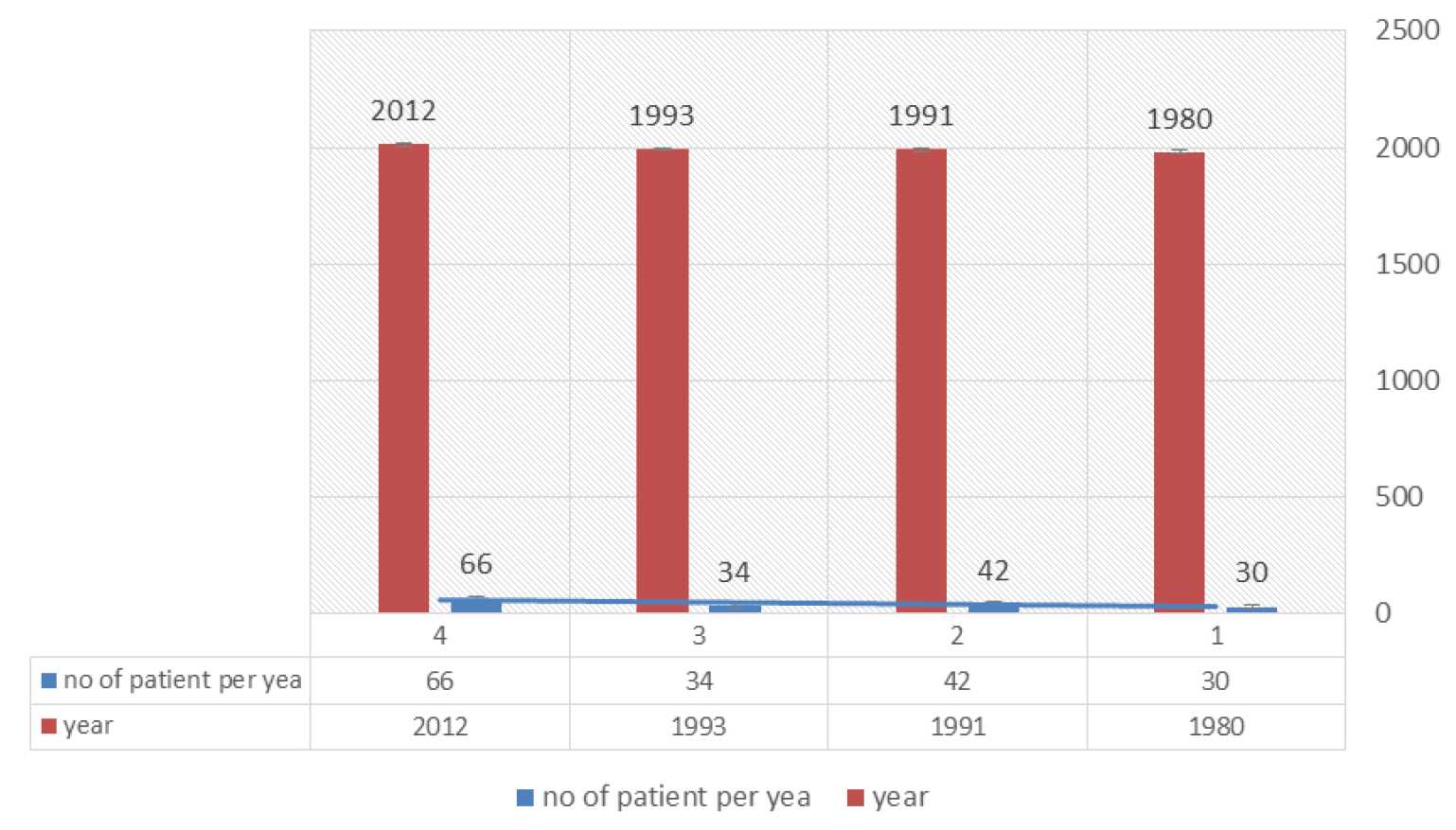
Figure 1: Average number of patients per year in Iraqi studies
This doubling in the incidence of AML may be related to environmental changes mainly ionizing radiation and chemicals, the major etiological factors blamed for the occurrence of acute leukaemia, especially AML, reflecting one of the massive consequences of wars humanity in Iraq (Tables 1-5).
Table 1: Causes of excluded cases of AML related to years from beginning of 2005 to the end of 211
Causes of excluded cases | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | Total |
Relapse | 1 | 3 | 2 | 3 | 3 | 2 | 3 | 17 |
Review | 1 | 2 | 1 | 4 | 4 | 2 | 4 | 18 |
Age < 15y | 3 | 1 | 2 | 2 | 2 | 7 | 4 | 21 |
Un classified AML | 2 | 1 | 1 | 2 | 4 | 4 | 4 | 18 |
Missing information | 2 | 3 | 2 | 3 | 3 | 4 | 3 | 20 |
Previous hematological disorders | 1 | 2 | 1 | 3 | 4 | 4 | 4 | 19 |
Total | 10 | 12 | 9 | 17 | 20 | 23 | 22 | 113 |
The WHO classification has been widely applied in the diagnosis of leukaemia and improved the predictive value of classification However, it was shown that FAB classification, based on morphology and simple cytochemical stains, remain effective enough, although cytogenetics and immunophenotyping can add to diagnostic accuracy in some cases [9] (Tables 6-8).
WHO classification of leukaemia was formulated in 1997, however, the requirement of cytogenetics and immunophenotyping makes it difficult for many countries to put it in routine use.
This study revealed that 28.2% of the patients had AML-M3. This finding may be attributed to the age of the studied sample (Table 3). AML is a disease of older adults [10].
This study showed a significant association between age and subtype of leukaemia. This was consistent with that reported in united states and Northern Europe [5]. The median age (38 y), the mean age 40.2 ± 2 and the age range was (15-85 years) (Table 2), which is in agreement with that previously reported in Iraq [6]. The finding of more than 25% of AML patients were aged greater than 55 years is similar to that reported in Saudi Arabia (mean age 30 ± 13 years) [7] and Pakistan (mean age was 38 ± 2 years) [11] but inconsistent to that reported in developed countries like Europe and North America in which approximately 60% of AML cases are in patients greater than 60 years of age [7,11,12] (Table 2).
Table 2: Age distribution in AML
Age groups (year) | AML | |
No. | % | |
A (15 –24) | 113 | 24.1 |
B (25 –34) | 87 | 18.6 |
C (35 –44) | 70 | 15 |
D (45 –54) | 73 | 15.6 |
E (55 –64) | 69 | 14.7 |
F (≥ 65) | 56 | 12 |
Total | 468 | 100 |
P= 0.00002
This may be attributed to the fact that demographic differences exist between developed and developing countries. Geographical and economical variations may explain the difference too.
This study showed that males to females' ratio 1:1.05 in agreement with the findings of Al-Azawi and Yaha in Iraq 1993 (M: F 1-1.4) (Table 3) [6], a slight female predominance in adult patients of AML in contrary to that reported in Pakistan and United States in which male to female ratio was 1.3:1 [13,14]. No male predominance was observed in AML which was similar to that reported previously in Iraq (Baghdad 1991) (1.04:1) [5]. This could be due to the difference in the sample size.
Table 3: Sex distribution in subtypes of AML
| AML Subtypes | Male | Female | M:F ratio | |
No. (%) | No. (%) | No. (%) | ||
M 0 | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
M 1 | 92 (19.7) | 46 (50) | 46 (50) | 1:1 |
M 2 | 123 (26.3) | 67 (54.5) | 56 (45.5) | 1.2:1 |
M 3 | 132 (28.2) | 59 (44.7) | 73 (55.3) | 1:1.2 |
M 4 | 37 (7.9) | 15 (40.5) | 22 (59.9) | 1:1.5 |
M 5 | 70 (15) | 33 (47.1) | 37 (52.9) | 1:1.1 |
M 6 | 9 (1.9) | 6 (66.7) | 3 (33.3) | 2:1 |
M 7 | 5 (1) | 2 (40) | 3 (60) | 1:1.5 |
Total 468 (100) | 228 (48.7) | 240 (51.3) | 1:1.05 | |
P= 0.435
This is probably due to smaller sample size in previous studies or due to a change in environmental factors.
It is in concordant with that of Arber et al. [15], a study from UK showed that the predominant subtype was M1 [16]. These differences may be attributed to the fact that there are specific genetic factors responsible for particular FAB subtype of AML. Variation in haemoglobin levels as reflected by the variations in PCV in this study is similar to that reported in Iraq previously which reveal PCV >30% in the majority of cases [6]. The study demonstrated an extreme leucocytosis which was observed in 53.2% AML patients. It is in agreement with that reported by Chen et al. as said Godwin and Smith [7].A significant variation of WBC count with the subtypes of AML was observed. Recently, it was stated that WBC count is a simple and powerful prognostic factor in a range of malignancies [11], because most of cases have leucocytosis and when WBC count is >30,000/µl it is considered as bad prognosis (Tables 4 and 5).
Table 4: PCV distribution in AML patients
| AML | PCV % | |||||
< 24 | 24 - 30 | > 30 | ||||
No. | % | No. | % | No. | % | |
221 | 47.2 | 173 | 37 | 74 | 15.8 | |
Table 5: WBC count distribution in AML patients
AML | WBC count (× 109/ L) | |||||
0.4 – < 4 | 4 – 11 | > 11– 320 | ||||
No. | % | No. | % | No. | % | |
110 | 23.5 | 109 | 23.3 | 249 | 53.2 | |
P = 0.00001
This study revealed that neutropenia was detected in 59.8%, of AML patients, it is in agreement with findings of Al-Azawi and Yaha (<50%) [6]. Neutropenia is a major factor for developing serious infection and subsequent infection related death and the finding that more than half of AML patients had low platelets count (<50×109/ L) is in agreement with that of other investigators like Tornebohm et al. [17], who reported that patients with acute leukaemia had platelets count of <20×109/L. Several workers [5] reported disseminated intravascular coagulation and fibrinolysis in patients with acute myeloid leukaemia, this may explain the reduction in the platelets count which may aggravate the reduction due to BM suppression of normal haematopoiesis In This study 78% of AML patients had circulating blast in peripheral blood, it is dissimilar with findings reported by Al-Azawi and Yaha (<90% of patients with AML had circulating blast in peripheral blood) [6]. Chen et al. [18] reported that survival time was significantly reduced when peripheral blasts exceed 5%. The peripheral blast cells count is strongly correlated with WBC count. The study showed that 32.3% of patients with AML had Auer rods and highly frequent in AML-M3 subtype than other subtypes this is similar to that previously reported by AL-Allawi [5] and Hilmi in Baghdad 1991 (Tables 6-12).
Table 6: Neutrophil Count in AML
AML (468) | Neutrophil | |||||
Neutropenia < 2 × 109/L | Normal 2-7 × 109/L | Neutrophilia >7 × 109/L | ||||
No. | % | No. | % | No. | % | |
280 | 59.8 | 125 | 26.7 | 63 | 13.5 | |
P = 0.00002
Table 7: Neutropenia in AML patients
AML (280/468) | Neutropenia | |||||
< 0.5 × 109/L | 0.5-1 ×109/L | >1 – < 2 × 109/L | ||||
No. | % | No. | % | No. | % | |
168 | 35.9 | 51 | 10.9 | 61 | 13 | |
P = 0.00002
Table 8: Platelets count distribution in AML patients
AML | Platelet's count (× 109/L) | |||||||
< 50 | 50 - 100 | 100 – 150 | > 150 | |||||
No. | % | No. | % | No. | % | No. | % | |
325 | 69.5 | 84 | 17.9 | 34 | 7.3 | 25 | 5.3 | |
P=0.00004
Table 9: Circulating blast cells in peripheral blood of AML patients
AML | Blast | |||
Present | Absent | |||
No. | % | No. | % | |
365 | 78 | 103 | 22 | |
P = 0.00002
Table 10: Presence of Auer rods in subtypes of AML
Subtype | No. (total) | Percent in each subtype |
M 0 | 0 (0) | 0.0 |
M 1 | 37 (92) | 40.2 |
M 2 | 44 (123) | 35.8 |
M 3 | 58 (132) | 44 |
M 4 | 7 (37) | 18.9 |
M 5 | 4 (70) | 5.7 |
M 6 | 1 (9) | 11.1 |
M 7 | 0 (5) | 0.0 |
Total | 151/468 | 32.3 |
P = 0.00001
Table 11: SBB results in AML
AML | SBB | |
Positive | Negative | |
No. (%) | No. (%) | |
n=243 | 208(85.6) | 35(14.4) |
P = 0.00002
Table 12: comparison of AML subtypes distribution in Iraqi studies
Year of studies | AML subtypes (%) | ||||||
M1 | M2 | M3 | M4 | M5 | M6 | M7 | |
1980 (121) | 17.4 | 38 | 19.8 | 18.2 | 6.6 | 0 | 0 |
1991 (214) | 22 | 24.3 | 16.8 | 22 | 9.8 | 5.1 | 0 |
1993 (54) | 11.1 | 31.4 | 24 | 14.8 | 11.1 | 5.5 | 1.8 |
2012 (468) | 19.7 | 26.3 | 28.2 | 7.9 | 15 | 1.9 | 1 |
There is an increase in the number of cases reported per year compared with previous studies in Iraq, showing a peak in the year 2011
AML is more common in younger age groups
The percentage and number of M3 AML subtype are getting more compared with previous Iraqi studies and ranked the first among other AML subtypes by M2
Death due to serious complications related to severe neutropenia is expected in more than one-third of patients and in more than two- third of patients due to severe thrombocytopenia
About 15% of acute leukaemia patients do not show blasts in the peripheral blood
Abeloff, M.D. et al. Clinical Oncology. 3rd ed., Churchill Livingstone, 2004, pp. 978.
Hoffman, R. et al. Haematology: Basic Principles and Practice. 4th ed., 2005.
Zhen-yi, W. “Ham-Wasserman Lecture: treatment of acute leukaemia by inducing differentiation and apoptosis.” American Society of Haematology, vol. 12, 2003, pp. 23.
American Cancer Society. Cancer Facts and Figures. American Cancer Society, 2007.
Al-Allawi, N.A. et al. “Acute myeloid leukaemia morphological subtyping and haematological findings.” Journal of the Faculty of Medicine Baghdad, vol. 33, 1991, pp. 59-71.
Al-Azawi, F.H. and H. Yahya. “Acute myeloid leukaemia: clinical features and follow up in 54 Iraqi patients.” Journal of the Faculty of Medicine Baghdad, vol. 35, 1993, pp. 51-58.
Godwin, J.E. and S.E. Smith. “Acute myeloid leukaemia in the older patient.” Critical Reviews in Oncology/Haematology, vol. 48, 2003, pp. S17-S26.
Abdulateef, S. et al. “Molecular study of FLT3-ITD mutation in Iraqi adult acute myeloid leukaemia patients; its correlation with clinicopathological parameters.” Pathology and Laboratory Medicine, vol. 1, 2017, pp. 14.
Nasreldin, E. et al. “T-regulatory and T-helper type17 cells associated cytokines (IL-35, IL-17) as potential diagnostic and prognostic biomarkers in Egyptian acute myeloid leukaemia patients.” Journal of Clinical and Cellular Immunology, vol. 7, no. 478, 2016, pp. 2.
Hulegårdh, E. et al. “Characterization and prognostic features of secondary acute myeloid leukaemia in a population-based setting: a report from the Swedish Acute Leukaemia Registry.” American Journal of Haematology, vol. 90, no. 3, 2015, pp. 208-214.
De Angulo, G. et al. “Absolute lymphocyte count is a novel prognostic indicator in ALL and AML: implications for risk stratification and future studies.” Cancer, vol. 112, no. 2, 2008, pp. 407-415.
Wedding, U. et al. “Elderly patients with acute myeloid leukaemia: characteristics in biology, patients and treatment.” Medizinische Klinik, vol. 98, no. 4, 2003, pp. 193-207.
Kakepoto, G.N. et al. “Long-term outcomes of acute myeloid leukaemia in adults in Pakistan.” Journal of Pakistan Medical Association, vol. 52, 2002, p. 482.
Xie, Y. et al. “Trends in leukaemia incidence and survival in the United States (1973-1998).” Cancer, vol. 97, no. 9, 2003, pp. 2229-2235.
Arber, D.A. et al. “Prognostic impact of acute myeloid leukaemia classification: importance of detection of recurring cytogenetic abnormalities and multilineage dysplasia on survival.” American Journal of Clinical Pathology, vol. 119, no. 5, 2003, pp. 672-680.
Swirsky, D.M. et al. “Features affecting outcome during remission induction of acute myeloid leukaemia in 619 adult patients.” British Journal of Haematology, vol. 64, no. 3, 1986, pp. 435-453.
Törnebohm, E. et al. “Bleeding complications and coagulopathy in acute leukaemia.” Leukaemia Research, vol. 16, no. 10, 1992, pp. 1041-1048.
