
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Anterior neck swellings are common in surgical and ENT practice; however, pulsatile anterior neck masses are rare and often indicate underlying vascular anomalies. Failure to recognize such conditions may result in catastrophic hemorrhage during diagnostic or surgical procedures. We report a case of a 65-year-old woman presenting with a painless, slowly progressive, pulsatile anterior neck swelling. Clinical examination and ultrasonography with Doppler suggested a vascular origin. Contrast-enhanced computed tomography confirmed a high-riding brachiocephalic artery ascending anterior to the trachea up to the C7–T1 level before bifurcation. The patient was managed conservatively and counseled regarding potential surgical risks. This case highlights the importance of careful clinical assessment and appropriate imaging in evaluating pulsatile neck swellings to prevent inadvertent injury during invasive procedures.
Anterior neck swellings are commonest presentation in a Surgical and ENT OPD practice [1]. The differential diagnoses of these swellings are myriad and vary from benign to malignant. These swellings can be acute or chronic in nature and can be life threatening sometimes. Moreover, these swellings cause clinical and cosmetic issues to the patients. Each of these swelling has to be investigated completely as it can have multiple variations. Anatomy of neck is very complex and has been reported with may anatomical aberrations [2,3]. Besides clinical history a good knowledge of anatomy is required to address these aberrations.
However, pulsatile anterior neck swellings are suggestive of vascular anomalies. Normally, brachiocephalic or innominate artery passes upward and to the right of the thoracic trachea and divides into the right subclavian and right common carotid arteries behind the sternoclavicular joint [4,5].
The aberrant high-riding of the brachiocephalic artery riding as far as the thyroid gland is rare, it can be asymptomatic or present with respiratory distress due to tracheal compression and may cause catastrophic haemorrhage if not recognized during neck surgeries [5-7].
A 65 years old lady, without any significant past history, complained of painless, pulsatile, approximately 4cm×3cm, soft, non-tender, anterior neck swelling for more than 7 months which slightly increased in size over the due course. She had no signs and symptoms of hyperthyroidism or any constitutional symptoms. Also, there was no thrill and the swelling was not moving with deglutition or protrusion of tongue.
On investigating further with ultrasound and Doppler, both thyroid lobes were normal in size. The neck swelling was possible to have a vascular origin most likely right subclavian or brachiocephalic artery, located just inferior to the right thyroid lobe. There was no other mural or eccentric dilatation of vessel wall or any change on Valsalva or coughing (Figure 1 and 2). CECT scan shows that the neck swelling corresponded to the right brachiocephalic artery which ascended along the anterior aspect of the trachea beyond the right sternoclavicular joint. Axial CECT image shows the brachiocephalic artery travels anterior to the trachea. Whereas, coronal CECT image shows the high rising right brachiocephalic trunk extending beyond the right sternoclavicular joint.
It reaches the level of C7-T1 then turned laterally (right) just inferior to the superiorly displaced right thyroid lobe to give off the right common carotid and subclavian arteries branches (Figure 3 and 4).

Figure 1: Realtime greyscale ultrasound cine loop of the neck
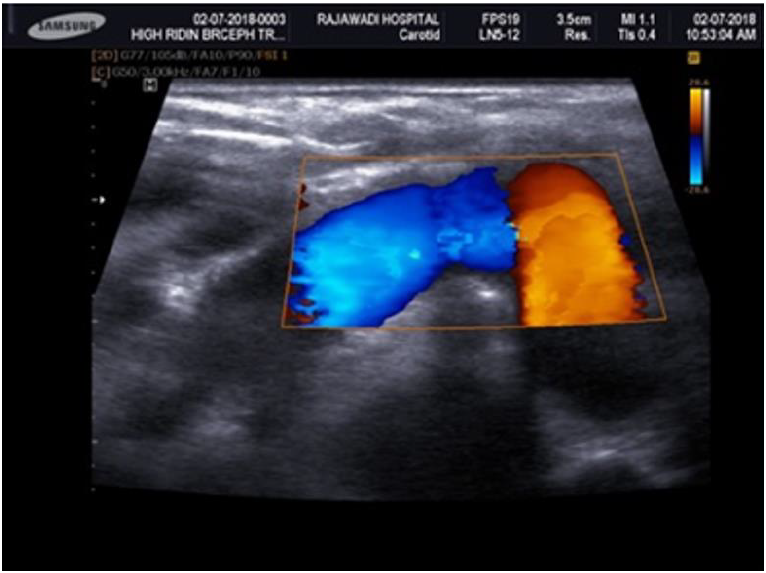
Figure 2: Doppler ultrasound image of the neck
Anterior neck swellings are very common and symptomless and noticed incidentally on palpation and can be of cosmetic concern. Most common differential diagnoses are Thyroid, Thyroglossal cyst in the midline and Salivary gland tumour, Lymphangioma on lateral side [1]. However, anterior neck mass which is pulsatile in nature is uncommon and can present as carotid body tumour. Brachiocephalic trunk or innominate artery develops from the aortic sac and the proximal right fourth aortic arch. One possible explanation of high riding brachiocephalic artery might be due to persistence of a portion of the proximal segment of right fourth aortic arch, which causes the elongation of the brachiocephalic artery superiorly. With the presence of the pulsation leads us to the suspicion of vascular origin.
As far as imaging modalities are concerned, ultrasound scan and doppler are the initial screening tool as FNAC or surgical biopsy are contraindicated to detect the vascular lesion. Ultrasound and doppler will also give a clear picture of vessels differentiating malformation, aneurysmal dilatation with normal variant. At the same time, it will be cost effective method of diagnosis in case patient needs conservative management. Computed tomography, magnetic resonance imaging, and angiography could be ordered for further detailed anatomic evaluation and definite guidance for therapeutic approach but may be costly in some patients.
It was challenging to find literature for high riding brachiocephalic artery. Prashant et. al. reported an incidental high riding brachiocephalic artery during mediastinoscopy [7]. Similarly, Racic et al. [8] reported incidental high riding brachiocephalic artery as potential operative hazard during a surgical procedure for parathyroid adenoma. Dua et al. [9] and Wong et al. [10] were able to diagnose high riding brachiocephalic artery during a radiological procedure. High riding brachiocephalic trunk reported as potential hazard during surgical procedure can pose as potential threat and can cause fatal hemorrhage while operating on anterior neck region if went unnoticed. This case was treated conservatively and patient was counselled regarding her neck swelling and was reported in her medical records to avoid any complications during neck surgery [10].
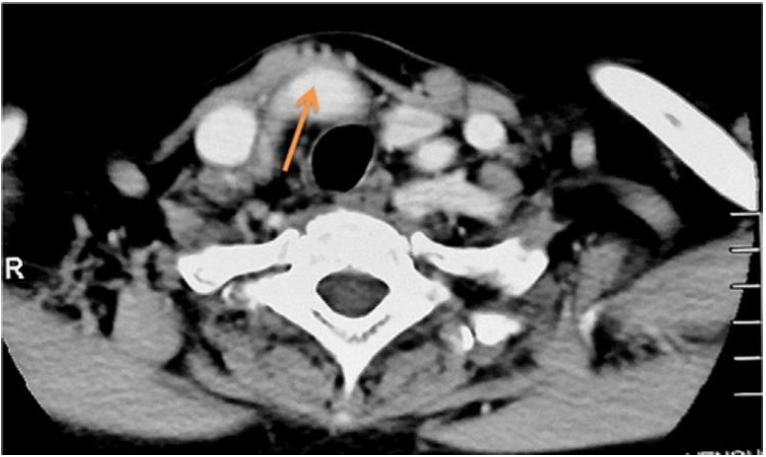
Figure 3: Axial CECT image shows the brachiocephalic artery travels anterior to the trachea
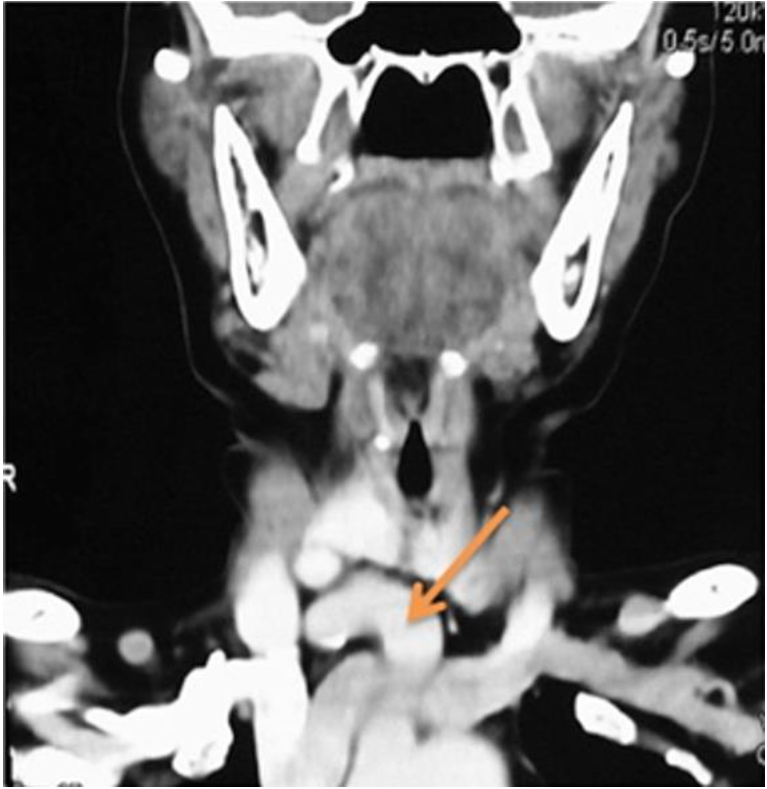
Figure 4: Coronal CECT image shows the high rising tight brachiocephalic trunk extending beyond the sternoclavicular joint
Pulsatile anterior neck swelling is very uncommon yet potential operative threat which can cause fatal hemorrhage if unnoticed. Hence, it should be diagnosed with ultrasound or doppler which is less expensive. In case asymptomatic cases the patient can be managed conservatively.
Khokhale, P.D. et al. “Study of benign neck swellings of anterior neck triangle at a tertiary care centre.” International Journal of Otorhinolaryngology and Head and Neck Surgery, vol. 5, 2019, pp. 941–945.
Russell, R.C. et al. Bailey and Love Short Practice of Surgery, 24th ed., 2004, chapter 72, p. 1253.
Skandalakis, J. et al. Skandalakis’ Surgical Anatomy. McGraw Hill Companies, Incorporated, 2004.
Bergman, R.A. et al. Illustrated Encyclopedia of Human Anatomic Variation, 1999, pp. 1–35.
De Garis, C.F. et al. “Patterns of the aortic arch in American white and Negro stocks, with comparative notes on certain other mammals.” Journal of Anatomy, vol. 67, no. 4, 1933, pp. 599–619.
Saniasiaya, J. and I. Mohamad. “A rare differential diagnosis of a solitary anterior neck mass.” Oman Medical Journal, vol. 31, no. 5, 2016, pp. 384–386, https://doi.org/10.5001/omj.2016.76.
Upadhyaya, P.K. et al. “Beware of the aberrant innominate artery.” The Annals of Thoracic Surgery, vol. 85, no. 2, 2008, pp. 653–654.
Racic, G. et al. “Abnormally high bifurcation of the brachiocephalic trunk as a potential operative hazard: case report.” Otolaryngology–Head and Neck Surgery, vol. 133, no. 5, 2005, pp. 811–813.
Dua, S.G. et al. “Incidental detection of high-riding innominate artery and bilateral retropharyngeal carotid arteries: radiological findings and clinical relevance.” Clinical Radiology, vol. 66, no. 7, 2011, pp. 685–687.
Wong, B. et al. “High riding of brachiocephalic artery: a rare case of pulsatile anterior neck mass.” Egyptian Journal of Ear, Nose, Throat and Allied Sciences, vol. 18, no. 3, 2017, https://doi.org/10.1016/j.ejenta.2017.07.006.
