
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Three samples that were subjected to postpartum complications were studied out of 22 cases and the main objective of this study was to know the management in the case of death of a twin foetus As these results were subjected to strong monitoring of the blood clotting file, in addition to that, the resulting complications were studied and were found to indicate that in the case of a twin pregnancy with the death of one foetus with good control. A miscarriage is not likely after week 12 or before week 24 (late miscarriage). In twin pregnancies, the cause of a late miscarriage is either an abnormal twin growth, twin transfusion syndrome or a TTTS foetal transfusion. This condition occurs when one identical twin sharing the same placenta receives a lot of blood in the womb, while the other receives too little, which affects its growth and development. Unfortunately, one baby dies while the other continues to grow for the remainder of the pregnancy.
A multiple pregnancy is a pregnancy in which one or more foetuses are developing in the womb at the same time. Multiple pregnancies occur in 0.4-1.6% of all pregnancies. Recently, there has been a clear trend towards an increased frequency of such pregnancies due to the active use of assisted reproductive technologies, including in vitro fertilization (IVF) [1-5].
Monozygotic (monozygotic) twins are formed due to the separation of a single egg at different stages of its development. The birth rate of monozygotic twins is 3-5 per 1,000 births. The division of the fertilized egg into two equal parts can occur because of delayed implantation (immersion of the embryo in the lining of the uterus) and lack of oxygen, as well as due to a violation of acidity and ionic composition of the environment, exposure to toxic and other factors. The appearance of monozygotic twins is also related to the fertilization of an egg that has two or more nuclei. If the egg separation occurs in the first three days after fertilization, the monozygotic twin has two placentas and two amniotic cavities and they are called monozygotic tuberculosis and diploid tuberculosis [3-6].
If egg splitting occurs between 4-8 days after fertilization, then two embryos will form, each in a separate amniotic sac. The two amniotic sacs will be surrounded by a common chorionic membrane with one placenta for two people these twins are called monochromic twins [5,6].
If separation occurs on the ninth and tenth days after fertilization, two foetuses will be formed with a common amniotic sac and placenta. These monozygotic twins are called monochromic amniotic cavity when dividing the oocyte at a later time, on the thirteenth - fifteenth day after conception, the separation will be incomplete, which will result in conjoined (non-separated, Siamese) twins [7,8]. This type is very rare, approximately 1 note in 1,500 multiple pregnancies or 1: 50,000-100,000 newborns. Monozygotic twins are always the same sex, have the same blood type, the same colour of eyes, hair and lightening of the skin of the fingers and they are very similar to each other [9].
The birth of twins occurs once in 87 sexes, triplets - once in 87 two (6400) twins, quadruples - once in 873 (51200) triplets the origins of triplets, quadruplets and more twins differ [9-11].
Therefore, triplets can be formed from three separate eggs, from two eggs or one egg. They can be identical or different. Squares can also be identical or mismatched [10].
Symptoms of Foetal Death
Miscarriage and loss of the foetus are among the worst things that a pregnant woman may go through, especially if this is her first pregnancy, which causes her to go through a bad psychological state after this operation and abortion often occurs during the first trimester of pregnancy at a rate ranging between 15% and 20% in women [12,13].
Pregnancy symptoms gradually disappear
They are nausea, vomiting, dizziness and swelling
Bleeding from the uterus, which is often dark in colour
No increase in the size of the abdomen
Increased feeling of pain in the lower back
In addition, these pains are constant or intermittent
Secretions such as blood clots or a foul-smelling fluid stream from the vagina
Cramps occur in the body
Foetal loss of a twin during the primary trimester is anything but an exceptional occasion [1,14]. Deficiency of one twin in the main trimester doesn't seem to weaken the advancement of the enduring twin. Notwithstanding, foetal demise happening after mid incubation (17 weeks' development) may expand the danger of IUGR, preterm work, toxaemia and perinatal mortality. The reasons for foetal passing shift and incorporate twin-twin bonding, placental deficiency, intrauterine development impediment identified with toxaemia, velamentous inclusion of the rope, string injury, line around the neck and intrinsic anomalies. Therefore, sequential evaluations of foetal development and prosperity ought to be thought of [9,14,15].
Maternal coagulopathy, the most dreaded complexity following twin downfall, has all the earmarks of being exceptional, notwithstanding, coagulopathy has been accounted for to happen in around 3-5 weeks following foetal destruction. Along these lines, when foetal downfall happens in different growth after the primary trimester, an underlying maternal thickening profile with reassessment in 2-3 weeks isn't outlandish [16]. Observing of maternal coagulation factors isn't vital when foetal misfortune happens before 13 weeks of incubation.
Largely, chronicity instead of zygosity decides the danger of mortality and the dreariness. Thus, deciding the kind of placentation by ultrasonography can help in foreseeing the result. The perinatal mortality of monochromic twin pregnancies is twofold that of dichorionic twin pregnancies [5,8,15]. The commonness of monochorionicity in single intrauterine passing in twins is 50-70%. At the point when foetal downfall happens after mid incubation, there is a 17 % chance that the "enduring twin" in a monochromic development will either kick the bucket or endure significant dreariness. Significant dreariness is probably not going to happen in the enduring twin of a dichorionic growth [2,12].
Identical twins are produced when one egg splits and it grows into two foetuses. Identical twins may share the same placenta and amniotic sac or they may share a placenta while each of them has a separate amniotic sac. Genetically, the two children become the same. Both belong to the same type and share physical traits and characteristics. Identical twins, in rare cases, fail to separate completely and become singles. Infants are then known as conjoined twins [17].
Twenty-two twins were studied in Baghdad Hospital and the cases were well reviewed and it was known through the study to sick or pregnant women as returning to antenatal clinics where complications were found in some female The monitoring system was approved through standard prenatal testing, ABO Rh, Hb, GCT, routine and microscopic urine testing, viral markers and HIV Biweekly NST for more than 32 week as Figure 1 and Biweekly USG with biophysical.

Figure 1: NST
The study clarified several results and conclusions, including that the occurrence of death in a woman who is a twin-pregnant woman of one foetus is no longer an exceptional case and this is due to several reasons, including morbidity is the most common due to the anastomosis of blood vessels, which is present in monochorionic placenta and this leads to several bad results, including the incidence of tunnel syndrome. In the case of the common placenta, there is also a connection between the blood vessels of the twins and this connection can lead to blood flow from one foetus to the other. Which could lead to the death of the twins. In the case of a heterogeneous distribution of the chorionic region, it is possible that one embryo is much smaller than the other and over time it stops growing (Figure 2).
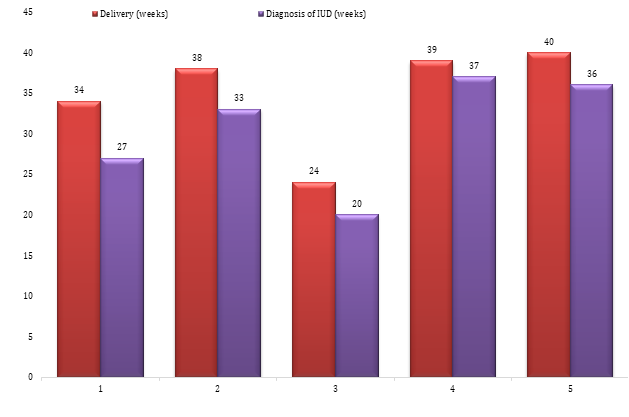
Figure 2: Diagnosis and Delivery (weeks)
It can be ascertained if the blood flow is not uniform in twins who share one placenta, by means of an ultrasound examination, in which case one of the twins has a large amount of amniotic fluid (1) and the other has a little or no amount. Here we need to measure the blood flow. In the umbilical cord to assess the health status of the twins and upon the death of one of the twins in the uterus; This raises the risk of a blood clotting disorder in the mother, especially after more than 3 weeks have passed since the death (Tables 1 and 2). The living foetus may also be affected while it is inside the womb [6,9,10,11,17], so there is a 20% probability that a brain injury will occur to it - God forbid. - and the cause of this damage is the leakage of small clots from the blood of the deceased foetus into the blood of the healthy foetus and settle in the vessels of his brain and we do not know when these clots begin to leak, as some studies have shown that they may leak very early and within only two days of death (which is It goes to the blood of a healthy foetus, not the blood of the mother) [4-12].
Table 1: Clarification and comparison to results before and after
Antepartum complication | Mode of delivery | Outcome |
women have PET in 30 weeks | Vaginal | Stillbirth, preterm child, mother okay |
IUD of 2nd twin at 38 weeks; 1st baby normal | Vaginal | Both baby and mother normal |
demise of the second twin 19 weeks later, the first twin suffers from a congenital heart problem and foetal distress | LSCS | 1st twin died, mother survived |
Single foetal death; no cardiac activity and no complication | Vaginal | jointly, normal |
Single foetal death; no cardiac activity in twin II and no complication | Vaginal | jointly normal |
Table 2: Chorioamnionicity and postmortem results
Specifications | Survivor features | Case |
| fresh | peaceful |
| weight 2.1 kg normal | peaceful |
| nil | peaceful |
After birth, the newborn should be examined well and a CT scan of the brain should be done then, if the imaging was normal and no brain damage appeared, because this indicates that the newborn did not have any clots and was not affected by the death of the first twin, but if the imaging showed the presence of damage in The brain (and this is what happens in 20% of cases, as above), here the treatment will be according to the severity of the case [7].
If the death of the foetus in the second or third trimester of pregnancy, such as the loss of one of the foetuses in the seventh month of pregnancy, the pregnancy becomes in severe danger and the pregnant woman must seek medical care if she suffers from bleeding, cramps or pelvic pain and must Using ultrasound to determine the presence of the dead foetus [13].
The researchers found that the death of one of the twins in the womb in the seventh month causes the spread of cerebral palsy and many other brain problems and the percentage of foetus survivors when the death of one of the twins occurs in the womb reaches one in ten of the foetuses of the same sex [17].
Some British researchers have confirmed that when a twin dies in the womb in the last three months before its birth and the surviving twin remains alive, it is more likely to develop cerebral palsy and other brain impairments, by up to 20% more than the twins survive [4,13,14,16].
Many experts assert that the death of one twin before birth in the second or third trimester of pregnancy causes the risk of cerebral palsy to be higher for the twins who survived and when the remaining twins are of the same sex as the foetus that died, the risk is higher [11].
The risk of childbirth increases when one of the twins dies in the womb after reaching the thirty-eighth week, so doctors perform a caesarean delivery, especially if the case is for identical twins who share the placenta and it is preferable that the birth takes place before the thirty-seventh week of pregnancy [14,17].
Enbom, J.A. “Twin pregnancy with intrauterine death of one twin.” American Journal of Obstetrics and Gynecology, vol. 152, no. 4, 1985, pp. 424-429.
Landy, Helain J. and Allan B. Weingold. “Management of a multiple gestation complicated by an antepartum foetal demise.” Obstetrical and Gynecological Survey, vol. 44, no. 3, 1989, pp. 171-176.
Fusi, L. and H. Gordon. “Twin pregnancy complicated by single intrauterine death: problems and outcome with conservative management.” BJOG: An International Journal of Obstetrics and Gynaecology, vol. 97, no. 6, 1990, pp. 511-516.
Sonneveld, S.W. and J.F. Correy. “Antenatal loss of one of twins.” Australian and New Zealand Journal of Obstetrics and Gynaecology, vol. 32, no. 1, 1992, pp. 10-13.
Ellis, R.F. et al. “The Northwestern University multihospital twin study. II. Mortality of first versus second twins.” Acta Geneticae Medicae et Gemellologiae: Twin Research, vol. 28, no. 4, 1979, pp. 347-352.
Zahálková, M. “Perinatal and infant mortality in twins.” Progress in Clinical and Biological Research, vol. 24, 1978, pp. 115-120.
Nylander, P.P.S. “Perinatal mortality in twins.” Acta Geneticae Medicae et Gemellologiae: Twin Research, vol. 28, no. 4, 1979, pp. 363-368.
Santema, J.G. et al. “Expectant management of twin pregnancy with single foetal death.” BJOG: An International Journal of Obstetrics and Gynaecology, vol. 102, no. 1, 1995, pp. 26-30.
Melnick, M. “Brain damage in survivor after in-utero death of monozygous co-twin.” The Lancet, vol. 310, no. 8051, 1977, pp. 1287.
Weiner, A.E. et al. “Coagulation defects with intrauterine death from Rh isosensitization.” American Journal of Obstetrics and Gynecology, vol. 60, no. 5, 1950, pp. 1015-1022.
Aslan, Halil et al. “The outcome of twin pregnancies complicated by single foetal death after 20 weeks of gestation.” Twin Research and Human Genetics, vol. 7, no. 1, 2004, pp. 1-4.
Botting, B.J. et al. “Recent trends in the incidence of multiple births and associated mortality.” Archives of Disease in Childhood, vol. 62, no. 9, 1987, pp. 941-950.
Myrianthopoulos, N.C. “An epidemiologic survey of twins in a large, prospectively studied population.” American Journal of Human Genetics, vol. 22, no. 6, 1970, pp. 611.
Enbom, J.A. “Twin pregnancy with intrauterine death of one twin.” American Journal of Obstetrics and Gynecology, vol. 152, no. 4, 1985, pp. 424-429.
Yoshida, K. and H. Soma. “Outcome of the surviving cotwin of a foetus papyraceus or of a dead foetus.” Acta Geneticae Medicae et Gemellologiae: Twin Research, vol. 35, nos. 1-2, 1986, pp. 91-98.
Szymonowicz, W. et al. “The surviving monozygotic twin.” Archives of Disease in Childhood, vol. 61, no. 5, 1986, pp. 454-458.
Anderson, R.L. et al. “Central nervous system damage and other anomalies in surviving foetus following second trimester antenatal death of co-twin: report of four cases and literature review.” Prenatal Diagnosis, vol. 10, no. 8, 1990, pp. 513-518.
