
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
A single blind comparative clinical study was done in order to evaluate the effectiveness of an external application of ointment which was prepared from seed powder of Pongamia pinnata. Two different concentrations, 5 and 10%, of the drug were prepared. Patients were selected from the outdoor patient division, Rural Siddha Ayurvedic Hospital, Kobalapuram. Thirty patients with bilateral involvement of the lesions were selected for the survey and categorized each to the Test1, Test 2, Standard and Control groups respectively, such that 15 lesions were included in each group. Ointment prepared from the seed power of P. pinnata was given to apply twice a day on the selected lesion in the test groups. Observation was done after two weeks and follow up week. At the end of the treatment, p-value for skin pigmentation reduction T1 and T2 were 0.003 and 0.000 respectively indicating that significant improvement was achieved compared to the control group (p-value of 0.104). The p-values for the area size difference of the two groups were 0.001 and 0.001 respectively. It shows the effectiveness of the area reduction of both groups were significant and same. But the p-value for the control group was 0.153 and it implies an increase of the lesion area. So the improvement of the pigmentation reduction of the lesion and reduction of area size can be seen with the external application of the ointment prepared from the seed powder of P. pinnata.
This is a single blind comparative clinical study to determine the effectiveness of external application of the Pongamia pinnata seed powder in the management of Themal. The effectiveness of the drug will be assessed with two different concentrations on Themal and the associated factors such as skin hypo/hyper pigmentation and size that affect the lesion will be ascertained. Fungal skin infections are the most common skin disease condition within Sri Lanka as per the statistics, out of which the majority is Pityriasis versicolor which accounts for a prevalence of 10.5% [1]. Themal is one of the kuttam in Siddha comparable to Pityriasis versicolor in Allopathic Medicine. It occurs on the upper trunk and extends on to the upper arms finally scaling, guttate or nummular patches appear, particularly on young adults who perspire freely [2]. In siddha system of medicine many plants are documented for the treatment of skin diseases. Among those the P. pinnata seed has been selected by the researcher for the study. Also there are limited studies done to identify the effectiveness of P. pinnata toward its anti-fungal activity. The P. pinnata is widely used as a traditional medicine commonly known as ‘pungai’ in Tamil. It is a source of biomedicines and used as a crude drug for the treatment of tumours, piles, skin diseases, itches, abscess, painful rheumatic joints wounds, ulcers and diarrhoea [3]. According to the Siddha literature, the stanza postulates that the P. pinnata seed has the potency to cure the Themal [4]. Fungal skin infections are the most common skin disease condition in Sri Lanka as per the statistics, out of which the majority is Tinea vesicolor which accounts for a prevalence of 10.5% [1]. On the other hand, limited studies have been done to identify the effectiveness of P. pinnata toward its anti-fungal activity.
Hence, the present study will be an initiative to find out the anti-fungal activity of its seeds such that it could be effectively used for the Tinea versicolor condition.
Review of P. Pinnata
Scientific Name : Pongamia pinnata (Linn.) Pierre, Syn. Pongamia glabra Vent
Plant Family : Fabaceae
Tamil Name : Pungam-maram
Sanskrit Name : karanja
English Name : Indian beech
Sinhala Name : Karanda [5]
P. pinnata is a medium sized evergreen or briefly deciduous glabrous tree, 15-25m high, with straight or crooked trunk 50-80 cm or more diameter and broad crown of spreading or drooping branches. The bark is greyish green or brown, smooth or covered with tubercles, leaves compound, imparipinnate, leaflets opposite, 5-9 in number ovate or elliptic. Flowers white tinged with pink or violet, fragrant, in axillary racemes pods are compressed woody, elliptic to obliquely oblong pointed at both ends, Indehiscent, yellowish gray when ripe, varying in size and shape, 4.0-7.5 cm long and 1.7-3.2 cm broad, seeds usually one, rarely two, elliptical or reniform, 1.7-2.0 cm long and 1.2-1.8cm broad, wrinkled with reddish brown leathery testa [6].
Objective of the study
To identify the effectiveness of seed powder of P. pinnata on Pityriasis versicolor (Themal).
To determine the optimum effectiveness of the drug among two different concentrations based on
Skin pigmentation reduction, Area size difference of the selected macular lesion, Age and sex distribution of patients with Pityriasis versicolor, Lesion distribution in the patient’s body.
Study Design
This is a single blind comparative clinical study in order to evaluate the effectiveness of seed powder of P. pinnata on Pityriasis versicolor (Themal). Thirty patients were selected for the study by systematic randomization. The patients with bilateral involvement of the lesions were selected and categorized each to the Test 1 (T1), Test 2 (T2), Standard (S) and Control (C) groups respectively, such that 15 lesions were included in each group. Altogether 60 lesions were selected for the study. This study was conducted after the selection of patients, for a period of one month from 02/03/2019 to 02 /04/2019.
Selection of Patients
Patients were selected according to the inclusion and exclusion criteria from the outpatient department of the Rural Siddha Ayurveda Hospital, Kobalapuram. The purpose of trial was explained to the patients and got their consent. All the selected patients were interviewed by the researcher in first visit to the OPD.
Plant Material
The plant P. pinnata was selected from the quotation of general character of P. pinnata which is mentioned in the text book of Kunapadam (Part 1) Porutpanpu nool written by Murugesa Muthaliyar [4]. The seeds of P. pinnata were collected from the local area of Trincomalee district. The seeds of P. pinnata was authenticated.
Preparation of the Medicine
The seeds were collected and it will be cleaned, de-shelled naturally and dried. Then seeds were finely powdered using the grinder. The prepared powder was mixed with the emulsifying ointment and 5% and 10% ointment was prepared.
Methodology
Thirty patients with bilateral involvement of the lesions were selected. The assessment of the disease was done through history taking, general examination and the systemic examination. The prepared ointment of two concentrations 5% and 10% were given to test 1 (T1) and test 2 (T2) respectively. It was given to be applied externally twice a day for a period of 2 weeks with a follow up period of 1 week. The ketoconazole cream was given as the standard drug for the standard group (S). The control group (C) was treated with emulsifying ointment. The clinical evaluation of the patients was performed at week 1, week 2 and week 3. In the first day at baseline, a target area was identified and clinical assessment was done in each subject. The evaluation of the skin pigmentation and size of the lesion were done according to the following criteria.
Clinical Evaluation
Clinical evaluation visits were made at baseline, week 1, week 2 and week 3. Effect of treatment was evaluated on the basis of the clinical parameters; reduction in the skin pigmentation and affected area size difference were recorded at every visit. Hyperpigmentation/ erythema and hypopigmentation was evaluated by using IGA scale for hyperpigmentation. The affected area of the lesion, the efficacy of the drug, effectiveness of the drug by the skin hypopigmentation, overall effectiveness of the drug was calculated.
This was a single blind comparative clinical study carried out at Rural Siddha Ayurveda Hospital, Kobalapuram. Thirty patients were selected with hypo-pigmented/ hyper-pigmented and mixed type of macular lesions with normal sensation.
Age and Sex Distribution
The age and sex distribution of the patients with Pityriasis versicolor. Among thirty patients, 63.33% were males and 36.67% were females. The highest number of patients (50%) were between the age group of 20-30 and out of them 33.33% were males while 15% were females. In the age groups 31-40, 41-50 and 51-60, the male sex distribution was 13.33, 10 and 6.66% while female sex distribution was 10, 6.66 and 3.33% respectively.
Distribution of Ptyriasis Versicolor Patients According to the Color of Lesions
Hypo-pigmented macules were seen in 25 patients (83.3%) followed by either mixed hypo and hyper-pigmented in 2 patients (6.67%) and hyper-pigmented in 3 patients (10%). The results are shown in Table 1.
Table 1: Distribution of Patients According to the Color of Lesion
Type of pigmentation | Total | |
No | % | |
Hypopigmentation | 25 | 83.3 |
Hyperpigmentation | 3 | 10 |
Mixed | 2 | 6.67 |
Total | 30 | 100 |
Distribution of Pityriasis Versicolor Lesions in the Patient’s Body
The prominent distribution of lesion on the patient’s body was observed in the neck (38.3%), back (16.8%) and chest (11.7%). Table 2 shows the lesion distribution on the patient’s body.
Table 2: Distribution of Pityriasis Versicolor Lesions on the Patient’s Body
| Affected area | Distribution (%) |
| Neck | 38.3 |
| Back | 16.8 |
| Chest | 11.7 |
| Shoulder | 10.3 |
| Hand | 8 |
| Arm and axilla | 6.6 |
| Abdomen | 5 |
| Face | 3 |
Variation of Skin Pigmentation
According to the evaluation criteria, the skin pigmentation of each and every patient in all groups were noted as follows. According to the Table 3, in 6.7% of the patients almost clear hyperpigmentation was noted in the test group 1 while 20% showed clear hyperpigmentation in the test group 2 (Table 4). According to the Table 5, 26.7% of clear of hyperpigmentation was noted in the standard group and no reduction in hyperpigmentation was recorded in the control group as indicated in Table 6.
Skin Pigmentation Variation Before and After the Treatment in Test 1 Group
According to Table 3, among the 15 lesions of Pityriasis versiolor, 6.7% was noted as almost clear of pigmentation while in 6.7% mild pigmentation was noted. Further 46.6% and 40% were noted as moderate and severe pigmentation respectively (Figure 1,2).

Figure 1: Before Treatment in Test 1 Group

Figure 2: After Treatment in Test 1 Group
Table 3: Skin Pigmentation Before and After Treatment in Test 1 Group
| Skin pigmentation | Test group 1 | |||
| BT | AT | |||
| No | % | No | % | |
| Clear of hyperpigmentation | - | - | - | - |
| Almost clear of hyperpigmentation | - | - | 1 | 6.7 |
| Mild, but noticeable hyperpigmentation | - | - | 1 | 6.7 |
| Moderate hyperpigmentation | 2 | 13.3 | 7 | 46.6 |
| Severe hyperpigmentation | 10 | 66.7 | 6 | 40 |
| Very severe hyperpigmentation | 3 | 20 | - | - |
Skin Pigmentation Variation Before and After the Treatment in Test 2 Group
Clear pigmentation was observed in 20 of the lesions while 26.7%, 20% and 33.3% were noted as almost clear, mild and moderate pigmentation respectively (Table 4) (Figure 3,4).
Table 4: Skin Pigmentation Before and After Treatment Test 2 Group
| Skin pigmentation | Test group 2 | |||
| BT | AT | |||
| No | % | No | % | |
| Clear of hyperpigmentation | - | - | 3 | 20 |
| Almost clear of hyperpigmentation | - | - | 4 | 26.7 |
Mild, but noticeable hyperpigmentation | - | - | 3 | 20 |
| Moderate hyperpigmentation | 1 | 6.7 | 5 | 33.33 |
| Severe hyperpigmentation | 11 | 73.3 | - | - |
| Very severe hyperpigmentation | 3 | 20 | - | - |
Figure 3: Before Treatment in Test 2 Group

Figure 4: After Treatment in Test 2 Group
Skin Pigmentation Variation Before and After the Treatment in Standard Group
Clear of pigmentation was noted in 26.7% of the lesions and almost clear, mild and moderate pigmentation were noted in 20%, 46.6%, 6.7% respectively (Table 5).
Table 5: Skin Pigmentation Before and After the Treatment in Standard Group
| Skin pigmentation | Standard | |||
| BT | AT | |||
| No | % | No | % | |
| Clear of hyperpigmentation | - | - | 4 | 26.7 |
| Almost clear of hyperpigmentation | - | - | 3 | 20 |
| Mild, but noticeable hyperpigmentation | - | - | 7 | 46.6 |
| Moderate hyperpigmentation | 2 | 13.3 | 1 | 6.7 |
| Severe hyperpigmentation | 7 | 46.7 | - | - |
| Very severe hyperpigmentation | 6 | 40 | - | - |
Skin Pigmentation Variation Before and After the Treatment in Control Group
Moderate, severe and very severe pigmentation were recorded in 13.3%, 46.7% and 40% respectively of the control group after the treatment (Table 6).
Table 6: Skin Pigmentation Before and After Treatment in Control Group
| Skin pigmentation | Control group | |||
| BT | AT | |||
| No | % | No | % | |
| Clear of hyperpigmentation | - | - | - | - |
| Almost clear of hyperpigmentation | - | - | - | - |
| Mild, but noticeable hyperpigmentation | - | - | - | - |
| Moderate hyperpigmentation | 3 | 20 | 2 | 13.3 |
| Severe hyperpigmentation | 9 | 60 | 7 | 46.7 |
| Very severe hyperpigmentation | 3 | 20 | 6 | 40 |
Evaluation of Effectiveness of the Test Drug Compared with the Control
Table 7 shows the mean values of skin hyperpigmentation before and after treatment of the test group 1 (T1) as 4.07 and 3.20 and for test group 2 (T2) as 4.13 and 1.67 respectively while for the standard group (S) the mean was 4.27 and 1.6 before and after the treatment. And for the Control Group (C) was 4.00 and 4.27 respectively. The p-value for the T1, T2, standard and the control were 0 .003, 0.000,0 .000 and 0.104 respectively.
Table 7: Evaluation of Skin Pigmentation in Test 1, Test 2, Standard and Control Groups
| Parameters | Test 1 (T1) | Test 2 (T2) | Standard (S) | Control (C ) | ||||
| BT | AT | BT | AT | BT | AT | BT | AT | |
| Mean | 4.07 | 3.20 | 4.13 | 1.67 | 4.27 | 1.33 | 4.00 | 4.27 |
| Mean difference | - | 0.867 | - | 2.467 | - | 2.933 | - | -0.267 |
| Std. deviation | - | 0.915 | - | 0.915 | - | 0.799 | - | 0.594 |
| Std. error mean | - | 0.236 | - | 0.236 | - | 0.206 | - | 0.153 |
| Df | - | 14 | - | 14 | - | 14 | - | 14 |
| Paired t | - | 3.666 | - | 10.435 | - | 14.222 | - | -1.740 |
| P | - | 0.003 | - | 0.000 | - | 0.000 | - | 0.104 |
The mean difference of the T1 is 0.867 while in T2 is 2.467. So the skin pigmentation reduction has increased in the T2. The mean difference of the standard group was 2.933.
So it shows skin pigmentation reduction was higher compared to T2. The mean difference in the control group is -0.267 and it shows that there is an increase in the pigmentation in the control group. The p-value of T1 is 0.003 and T2 is 0.000 (Figure 5,6).
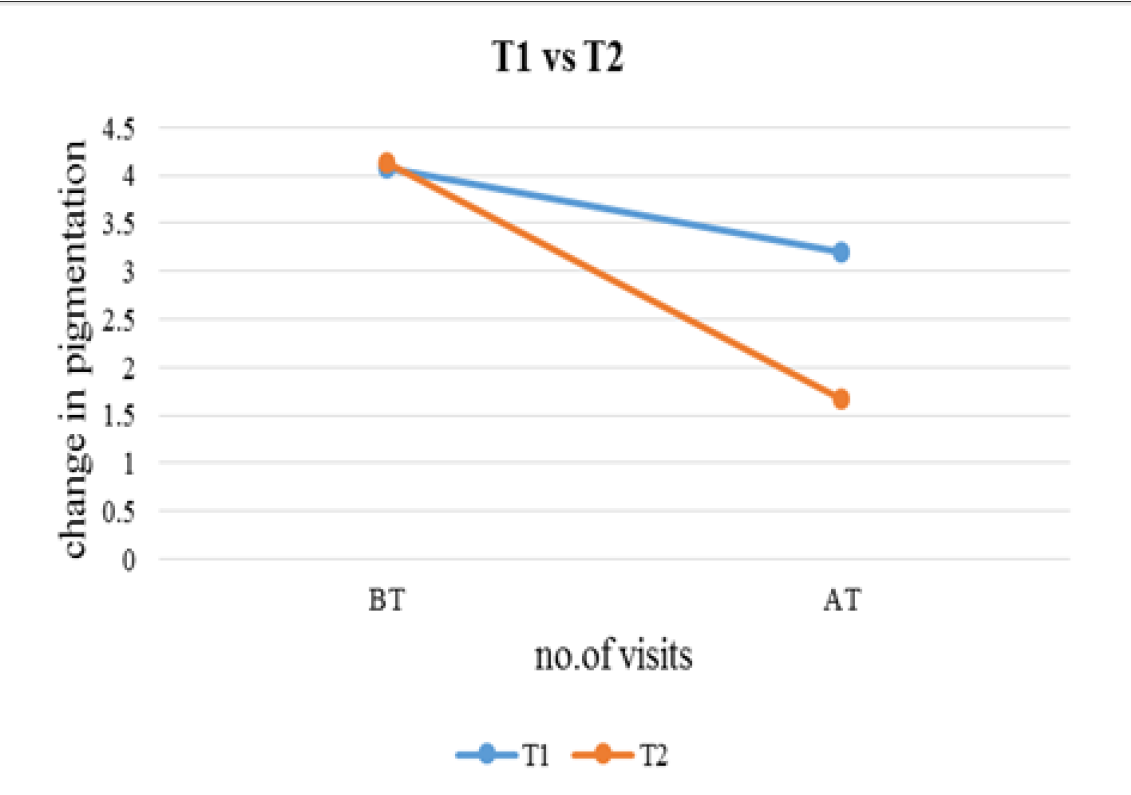
Figure 5: Skin Pigmentation Before and After Treatment in T1 and T2 groups
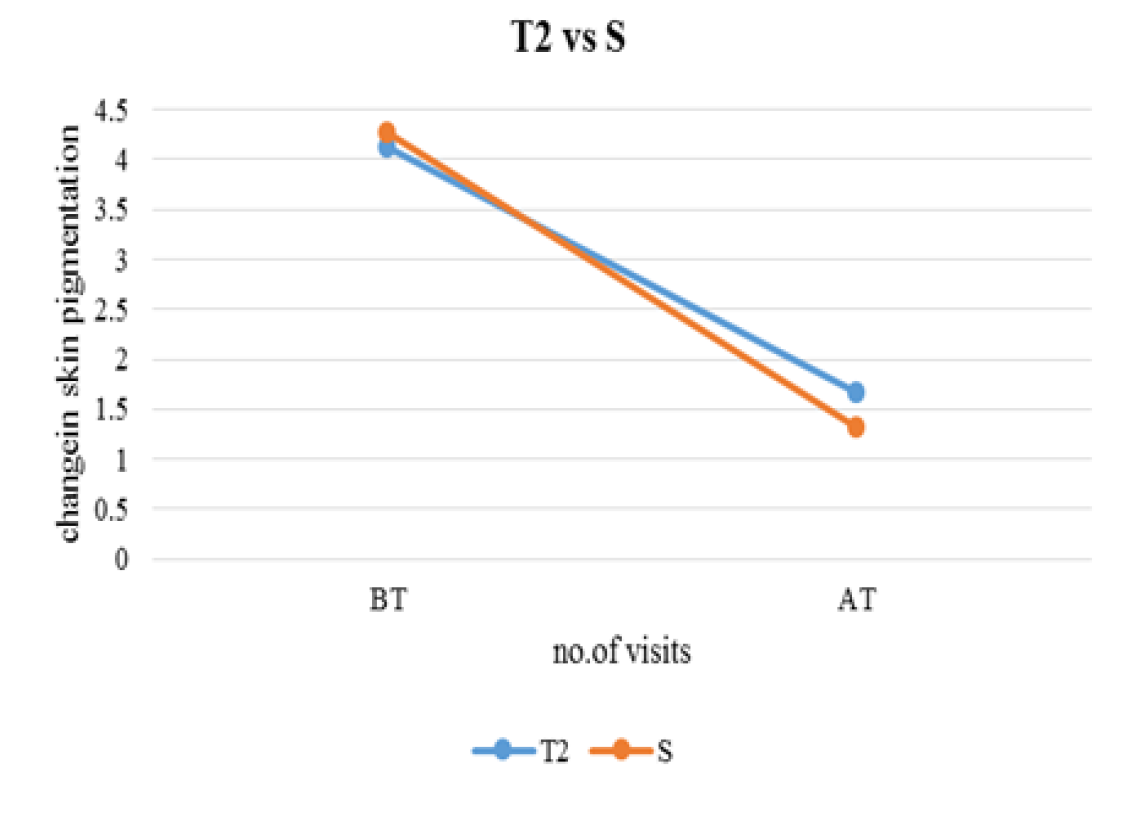
Figure 6: Skin Pigmentation Before and After Treatment in T2 and S groups
Evaluation of Area Size Difference in Each Group
Area Size Difference in Test Group 1: No changes were observed in visit 1 (Figure 7-16) and in visit 2 and visit 3 the mean area size difference was identical (0.0372) (Table 8,9).
Table 8: Area Size Difference in Test 1, Test 2, Standard and Control Groups
| Parameters | Test 1 (T1) | Test 2 (T2) | Standard (S) | Control (C ) | ||||
| BT | AT | BT | AT | BT | AT | BT | AT | |
| Mean | 0 | 0.0372 | 0 | 0.038 | 0 | 0.036 | 0 | -0.056 |
| Mean difference | 0 | 0.37 | 0 | 0.038 | 0 | 0.036 | 0 | -0.056 |
| Std. deviation | 0 | 0.033 | 0 | 0.033 | 0 | 0.021 | 0 | 0.143 |
| Std. error mean | 0 | 0.0087 | 0 | 0.0371 | 0 | 0.005 | 0 | 0.037 |
| Df | - | 14 | - | 14 | - | 14 | - | 14 |
| Paired t | 0 | 4.235 | 0 | 4.483 | 0 | 6.631 | 0 | -1.512 |
| P | 0 | 0.001 | 0 | 0.001 | 0 | 0.000 | 0 | 0.153 |
Table 9: Drug Effectiveness
| Parameters | Test 1 (T1) | Test 2 (T2) | ||||||
| BT | AT | BT | AT | |||||
| M | DE | M | DE | M | DE | M | DE | |
| SPR | 4.07 | 0 | 3.2 | 6.66 | 4.13 | 0 | 1.67 | 20 |
| ASD | 0 | - | 0.037 | 22.4 | 0 | - | 0.038 | 27.5 |
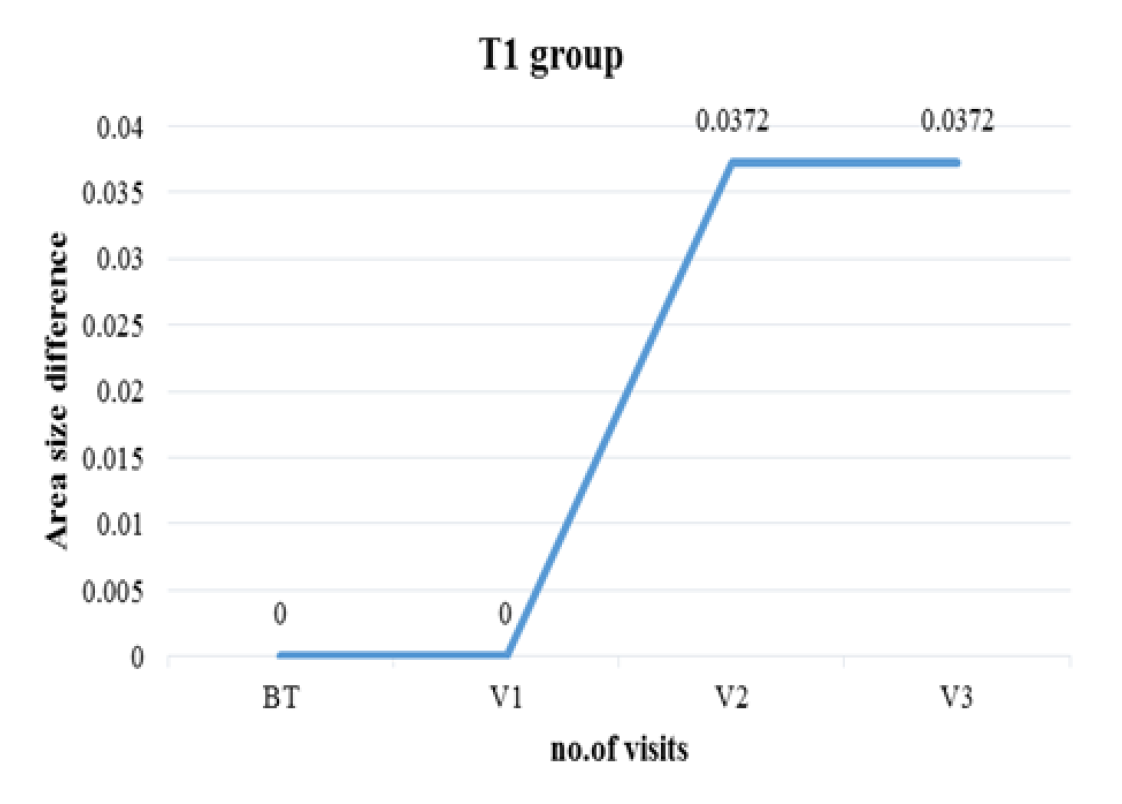
Figure 7: Area Size Difference in Test Group 1
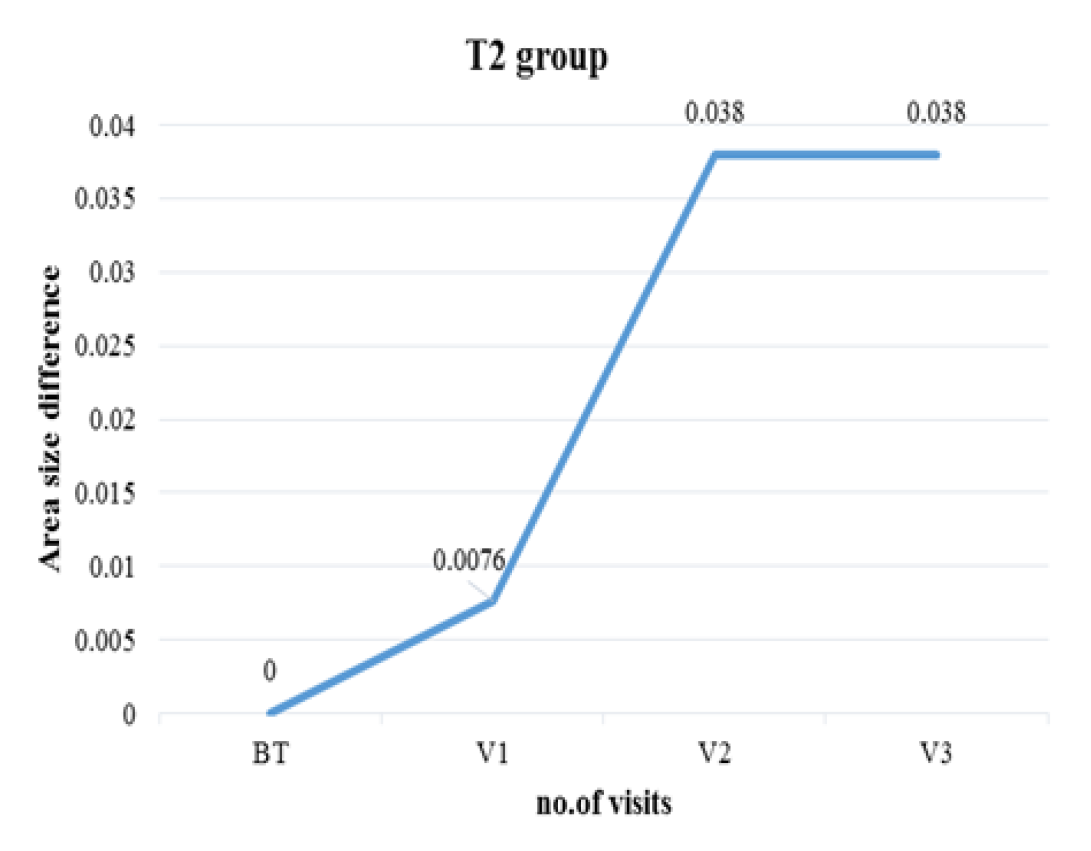
Figure 8: Area Size Difference in Test Group 2
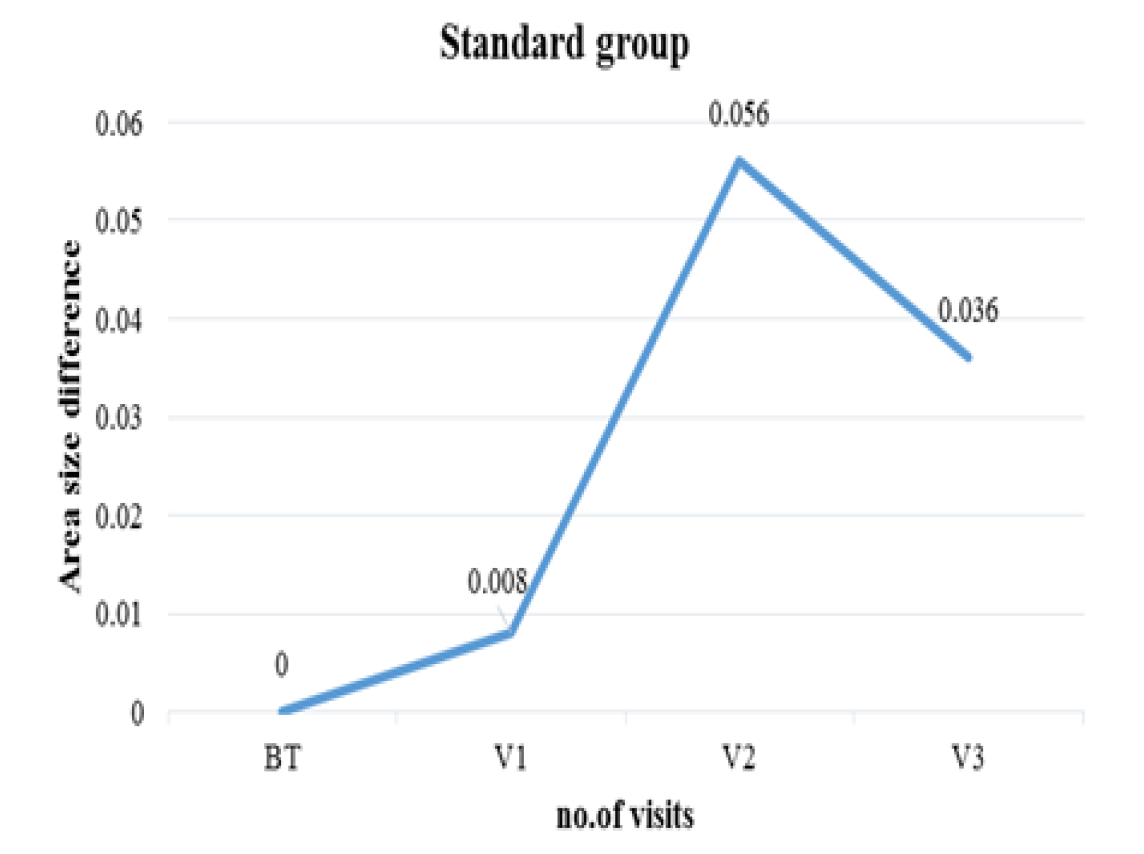
Figure 9: Area Size Difference in Standard Group
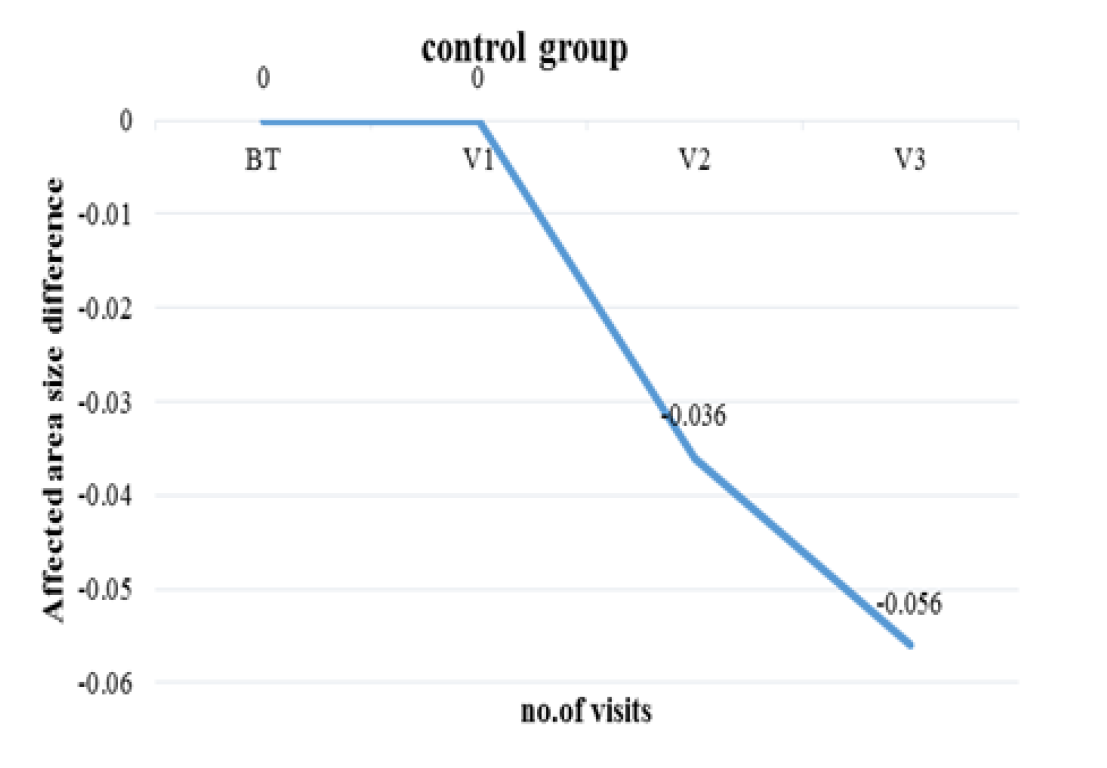
Figure 10: Area Size Difference in the Control Group
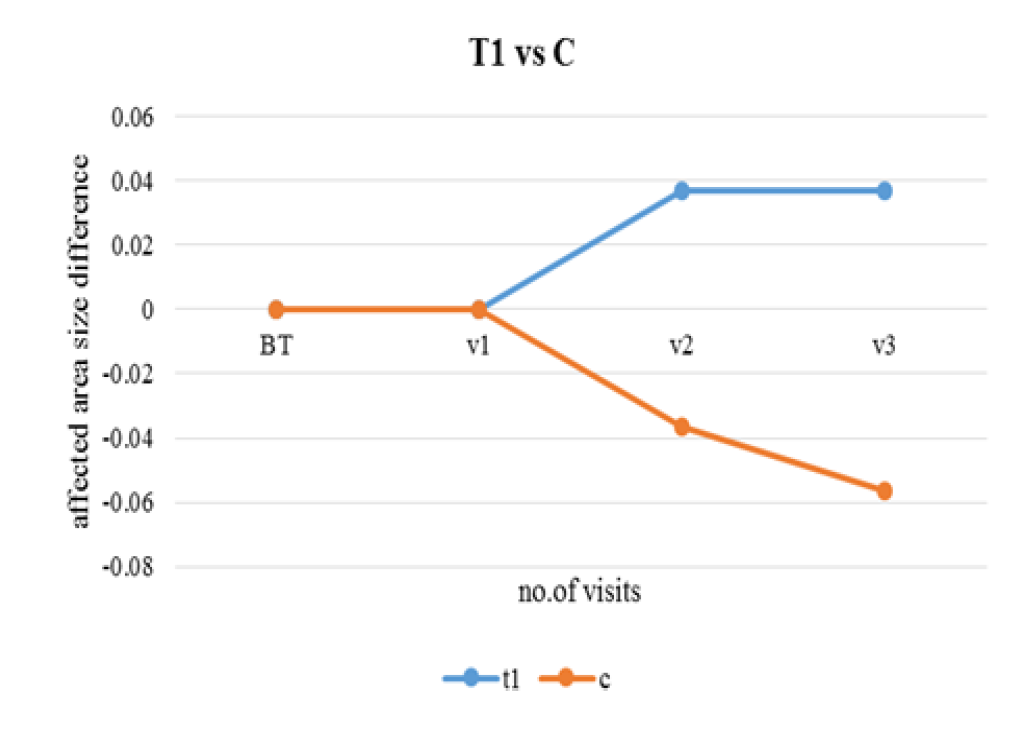
Figure 11: Area Difference Between T1 and C
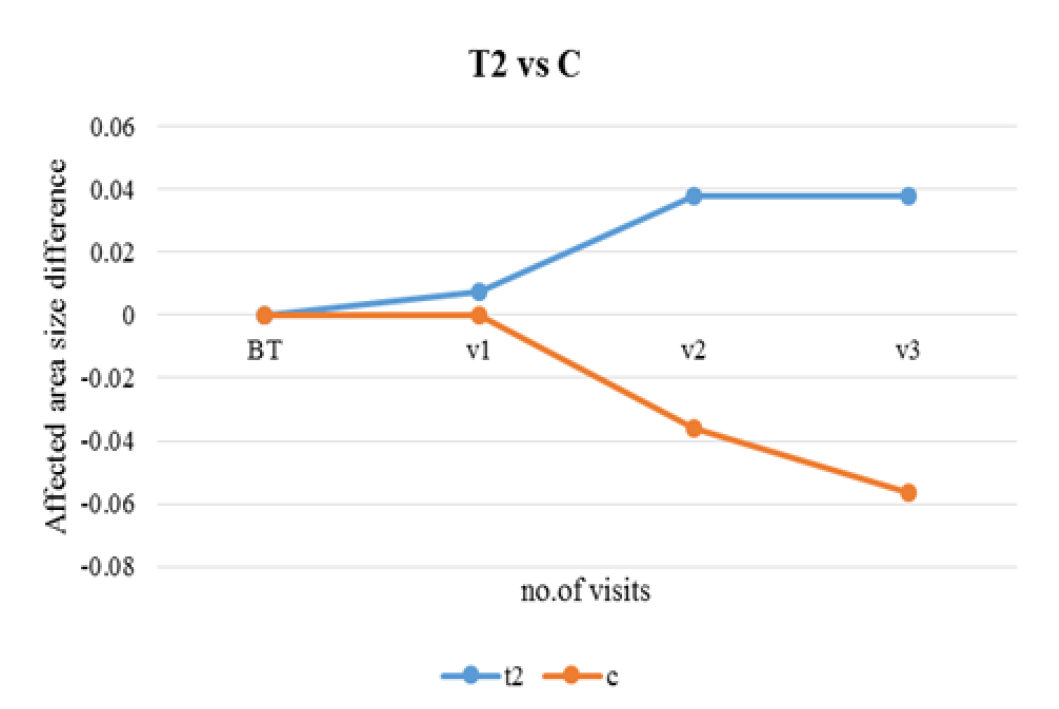
Figure 12: Area Difference Between T2 and C
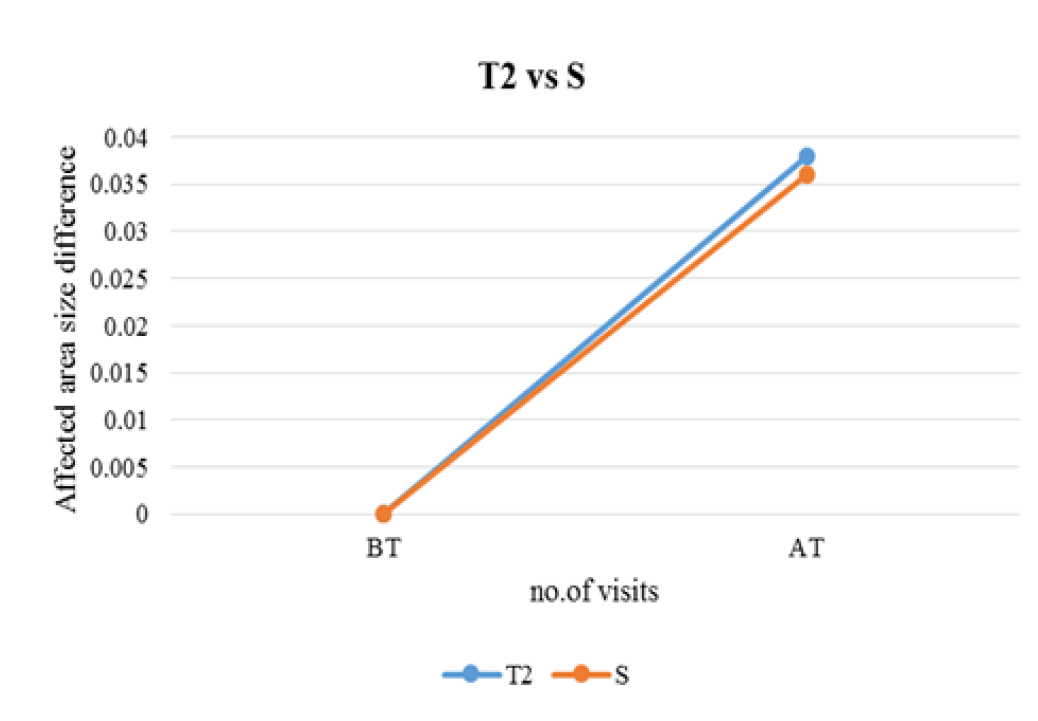
Figure13: Area Difference Between T2 and S

Figure 14: Area Difference Between T1 and T2
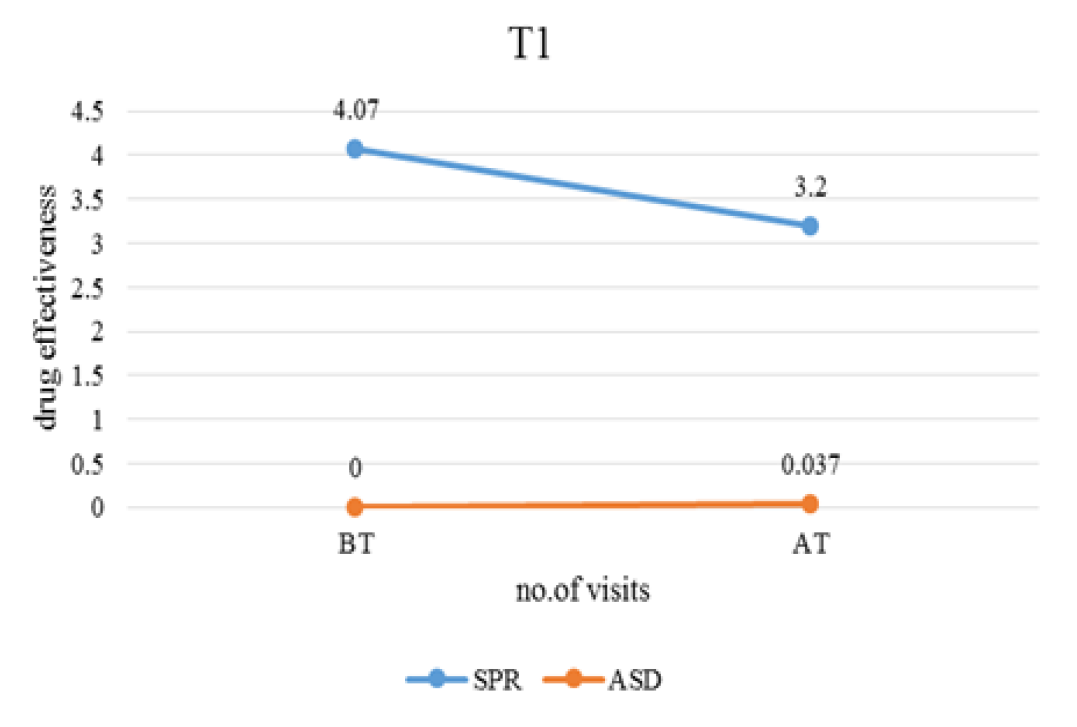
Figure 15: Drug Effectiveness of T1 Before and After the Treatment
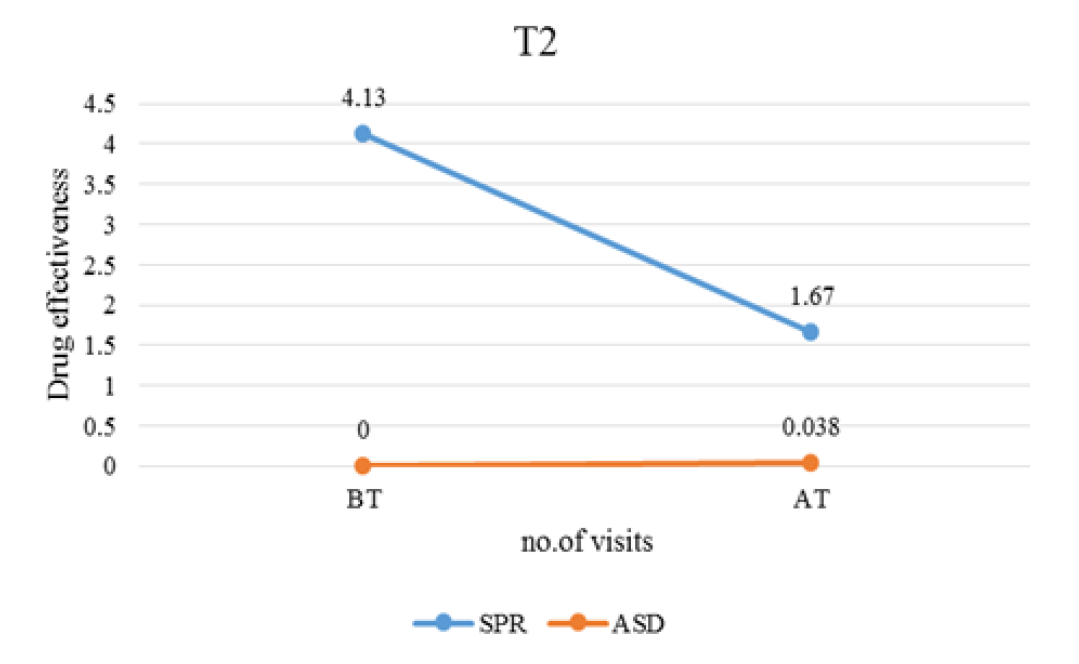
Figure 16: Drug Effectiveness of T2 Before and After the Treatment
Pityriasis (tinea) versicolor is a common disorder that affects people of all age groups, but is most commonly seen in adults. Infants and children can also be affected, but often have an atypical presentation. This disease is typically worse in geographic areas with tropical ambient temperatures. Multiple factors are known to contribute to its pathogenesis [7]. It is a mild, chronic infection of skin caused by Malassezia yeasts and characterized by discrete confluent, scaly, discolored or de-pigmented areas, mainly on the upper trunk. Colonization by these species is especially dense in the scalp, the upper trunk and flexures, areas rich in sebaceous glands and their secretions. The characteristic changes include hyperkeratosis, parakeratosis, acanthosis and a mild inflammatory infiltrate [8].
Yeasts of the Malassezia genus usually start colonization at puberty. Through androgen stimulation, sebaceous glands, peak at this stage and this would explain the higher incidence of Pityriasis versicolor in adolescence and adulthood. This incidence significantly drops at age extremes [9]. In the present study, the most common affected group was 20-30 years followed by 31-40 years. Similar findings were given by Kaur et al. [10], (age group 20- 30 years), Shah et al. [11] (age group 21-30 years). There were 19 (63.33%) males and 11 (36.67%) females who were clinically suspected of having pityriasis versicolor which is in agreement with studies by Ghosh et al. [12], Krishnan and Thappa [13], Rao et al. [14]. This may be due to major involvement of males in outdoor activities with maximum exposure to high temperature and humidity [15]. Kaur et al. [10], showed both sexes are equally prone to develop Pityriasis versicolor.
The lesions of the Pityriasis versicolor can be hypo-pigmented, hyper-pigmented, both or erythematous [11]. The type of lesions seen in the study were more of hypo-pigmented followed by hyper-pigmented and mixed types in 83.33%, 10% and 6.67% respectively, which correlated with the findings made by Shah et al. [11], (hypo-pigmented (84.17%), hyper-pigmented (8.63%), mixed (7.19%), Krishnan et al. [13], (Hypo-pigmented (84%), hyper-pigmented (9%), mixed (6%)), Kabbin et al. [16], (hypo-pigmented (67%), hyper-pigmented (31%), mixed (2%), while Rao et al. [14], observed mixed variety in 16.6%, hyper-pigmented in 8.30%. This variation in the morphological appearance of lesions may be due to differences in climatic conditions and different study population.
The most common involvement was neck, back and chest followed by arm and axilla. Similar findings are also noted by Dutta et al. [17], Rao et al. [14] and Tarazooie et al. [18], with chest, back and neck as most commonly involved sites. The distribution of lesions coincides with the density of sebaceous glands distribution with highest occurrence on chest and back [15].
P. pinnata is a medicinal plant used for treating many diseases. According to Murugesa Mudaliyar, the seeds of P. pinnata can be used in the management of Pityriasis versicolor. It possesses Karangin which has the antiseptic and insecticide properties. So it can be used for the skin conditions such as chronic eczema, psoriasis, scabies, ringworm and pityriasis [5]. In the present study, change of skin pigmentation was observed in the two different concentrations of the test drug. According to the table 5-4, almost clear pigmentation was observed in 6.7% of the patients in the test group 1 (T1) and 20% clear pigmentation in the test group 2 (T2) (Table 4). Clear pigmentation in 26.7% and 20% almost clear pigmentation in Standard Group (S) was observed (Table 5). There was no pigmentation reduction in the control group while increase density of the pigmentation was noted (Table 6). The p-value for pigmentation variation of the test group 1 was 0.003 and it was 0.000 for the test group 2 and standard group while p-value of the control group was 0.104. It showed that the pigmentation reduction in both test groups were significant and it is highly significant in the test group 2. The T2 and S group’s p-value are same and it shows similar reduction. But in the control group instead of the reduction, there was an increase of the skin pigmentation during the treatment period.
The mean values of the affected area size difference of the test group 1 and test group 2 increased (Table 7). Hence the reduction of pigmentation has increased along with the area size reduction. A negative mean value of the area reduction of control group implies that the affected area size is getting increased (Table 8). The p-values for the test1, test 2, standard and control are 0.001, 0.001, 0.000 and 0.153. So the area size reduction of the two test groups is similar and more effect on standard while increase of the size of the lesion was present in the control group.
According to the siddha text by Kuppusami Muthliyar [19], the Kapha become prominent in the pundareeka kuttam. Additionally, it is also mentioned in Kanthasami Muthaliyar [20], that at the severe stage of the disease condition the body becomes oedematous. The seed of P. pinnata posseses the suvai (taste) astringent and bitter, viriyum (potency) hot and vipakam (output) pungent. The panchaboothic composition of Kapha dosha is Earth and water and that of astringent and bitter taste is, air + earth and air + space respectively. Hence, the seed part of the P. pinnta can be used in the management of Pityriasis versicolor (themal) by balancing the vitiated Kapha dosha. The Table 9 shows the effectiveness of the drug before and after the treatment which was calculated based on the skin pigmentation reduction and area size difference. Based on the skin pigmentation, effectiveness can be shown as from the total patients in the group how many patients has reduced the pigmentation. So it is 6.66 % in T1 and 20% in T2. Based on affected area size difference, drug effectiveness can be taken as how much of the pigmentation was reduced by comparing the mean values before and after the treatment. So it is 22.4 % in T1 and 27.5% in T2. According to the table 4-1 mild to moderate effectiveness of action of the drug could be seen. The overall effectiveness of the drug is good.
Drug effectiveness based on skin pigmentation reduction in T1 is 6.7% and T2 is 20%. Effectiveness based on area size difference of T1 is 22.4% and T2 is 27.5%. Therefore, the overall effectiveness of the drug is good. And 10% ointment is better than the 5% ointment in the skin pigmentation reduction and area size difference of the lesion. Hence the seed powder of P. pinnata shows effectiveness on Pityriasis versicolor.
Perera, A. et al. “Prevalence of skin diseases in suburban Sri Lanka.” Ceylon Medical Journal, 2000. https://cmj.sljol.info/articles/.
Anandan, A.R. Special Medicine in Siddha. 1st ed., Department of Indian Medicine and Homeopathy, 2009, pp. 240.
Kumar, R.S.A.S. et al. “Study of Pongamia pinnata flower and seed for their antioxidant and antibacterial activity.” 2016. http://www.researchgate.net/publication/309556790.
Murugesamudaliyar, K.S. Siddha Materia Medica (Medicinal Plants Division). 9th ed., Indian Maruthuvam Homeopathy, 2013, pp. 691–693.
Jayaweera, D.M.A. Medicinal Plants (Indigenous and Exotic) Used in Ceylon. Part III, M.D. Gunasena & Co., 2006, pp. 228–229.
Warrier, P.K. et al. Indian Medicinal Plants: A Compendium of 500 Species. Vol. 4, Orient Longman, 1995, pp. 339–344.
Elewski, B.E. et al. “Guidelines of care for superficial mycotic infections of the skin: Pityriasis (Tinea) versicolor.” 1993. http://www.life-worldwide.org/assets/uploads/files/Guidelines_of_care_for_superficial_mycotic_infections.pdf.
Pramanik, S.B. et al. “A study of prevalence of different species of malassezia causing pityriasis versicolor and sites of distribution of lesions in a tertiary care hospital in Kolkata, India.” 2014. http://www.google.lk/.
Framil, V.M.S. et al. “New aspects in the clinical course of pityriasis versicolor.” 2011. http://www.scielo.br/.
Kaur, M. et al. “Study of distribution of malassezia species in pityriasis versicolor and healthy individuals in a tertiary care hospital, punjab.” 2013. http://www.google.lk/search.
Shah, A. et al. “Identification and speciation of malassezia in patients clinically suspected of having pityriasis versicolor.” 2013. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3667295.
Ghosh, S.K. et al. “Pityriasis versicolor: A clinicomycological and epidemiological study from a tertiary care hospital.” 2008. https://www.ncbi.nlm.nih.gov/pubmed/.
Krishnan, A. and D.M. Thapa. “Morphological and pigmentary variations of tinea versicolor in south Indian patients.” 2003. http://www.researchgate.net/publication/45263436.
Rao, G.S. et al. “Clinicoepidemiological studies on tinea versicolor.” 2002. https://www.ncbi.nlm.nih.gov/pubmed/.
Nazeema, T. et al. “Clinico-epidemiological study of pityriasis versicolor in a rural tertiary care hospital.” 2014. Available at https://doi.org/.
Kabbin, J.S. et al. “Clinicomycological study of pityriasis versicolor with special reference to the calcofluor white.” 2011. http://citeseerx.ist.psu.edu/viewdoc/download.
Dutta, S. et al. “Pityriasis versicolor: Socioeconomic and clinico-mycologic study in India.” 2002. http://www.researchgate.net/publication.
Tarazooie, B. et al. “Distribution of Malassezia species in patients with pityriasis versicolor and healthy individuals in Tehran, Iran.” 2004. https://www.ncbi.nlm.nih.gov/pubmed/.
Kuppusami Muthaliyar, K.N. Siddha Maruthuvam (Pothu). 8th ed., India Maruthuvam Homeopathy Thurai, 2016, pp. 686–687.
Kanthasamy Mudaliyar, K. Pathinen Siththar Arulich Seitha Nadi Saththiram. B. Rathnayaka & Sons, 2012, pp. 6.
