
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3239
ISSN (Online) : 2709-3220
HHV-6 constitutes a widely spread viral infection among young children population with a seroprevalence of > 80% in children > 2 years of age [1]. HHV-6 is an enveloped DNA virus belongs to the β-herpes virus family and, together with its closest homologue HHV-7, forms the roseoloviruses subfamily (2). A wide range of clinical manifestation of HHV-6 has been described which may vary with age and immune status of a child including acute febrile illness with or without rash, Roseola Infantum, febrile convulsion, meningo-encephalitis, hepatitis and mononucleosis-like illness, etc. Here we report the case of a 2 years old boy previously healthy who presented with fever, lethargy, decreased level of consciousness and with neck stiffness, diagnosed clinically with severe meningo-encephalitis and confirmed on brain MRI. Human Herpes Virus 6 was the etiology of his encephalitis, verified by his blood neuro-9 PCR.
Meningo-Encephalitis defined as an inflammatory condition of the brain parenchyma and the membranes surrounding the brain and spinal cord, has been associated with serious side effects and constitutes a life threatening condition if untreated in the right way. Despite the introduction of vaccines against mumps, rubella, measles, chickenpox and poliovirus which had decreased the rate of encephalitis, viruses remain the main causative agent of meningo-encephalitis throughout childhood. Viruses can invade the CNS via viremia by crossing the blood-brain barrier (e.g. Arboviruses) or by a retrograde axonal transport (e.g. Rabies virus) and it may infect neurons leading to cytotoxicity (e.g. herpes simplex virus; HSV) [2]. Reported HSV encephalitis cases with subsequent or concurrent antibodies against brain antigens like anti-N-methyl-D-aspartate receptor (anti-NMDAR) antibodies have been cited [2]. Meningo-encephalitis can rarely occur as a complication of HHV-6 or as the primary manifestation of HHV-6 infection in otherwise immunocompetent hosts. The high tropism of HHV-6 towards the T cells may explain its ability to be the cause of persistent infection in different tissues including the salivary glands, in addition to its ability to the complement-regulatory trans membrane protein CD46 constitutes the only identified cellular receptor, this protein is ubiquitously expressed in humans, allowing the viruses to infect a wide range of cells and tissues, including cells from the central nervous system (CNS) [3]. In this article we report a case of HHV-6 meningo-encephalitis in a 2 year old previously healthy boy presented with clinical acute meningo-encephalitis confirmed by brain MRI, complicated by right hemiplegia, treated with full course of 21 days antiviral and antibacterial therapy and showed complete neurologic improvement without any sequalae.
Case Description
We present the case of an almost two years old boy previously healthy, born by cesarean section with no ICN admission, his past medical and surgical histories are negative, no previous hospitalization or recurrent infections.
The child had normal neurodevelopmental history (no delay in milestones), vaccination history was up to date (according to his age). He presented with a history of somnolence, change in level of consciousness and high grade fever that developed progressively over the last three days. In the ED he was febrile, tachycardic, normotensive, and lethargic with hyperextended neck. His physical exam was significant for neck stiffness, normally reactive pupils, poorly responsive baby; his Glasgow Coma Scale was 11-12. Urgently first dose of Ceftriaxone, Vancomycin and Amikacin were given and CT brain done showing total enfacement of the brain tissue with no evidence of the sulcal pattern Figure 1, CRP was elevated associated with left shift leukocytosis. The patient was admitted to PICU, infectious disease specialist and neurologist were consulted, IV antibiotics meningeal dose continued, acyclovir added, lumbar puncture was contraindicated because of brain edema, methylprednisolone added to treatment. 48 hours after admission, clinical improvement started to show with reduced neck stiffness and slowly recovering mental status (he started to follow command by eye movements according to the corresponding direction with slight neck deviation, good muscle strength and slight improvement in swallowing). Repeated CT brain revealed a large area of focal hypo density involving the left fronto-parietal lobe and Sylvian fissure, focal densities were also noted involving the left thalamus and retro thalamic area with persistence of the effacement of the brain tissue and compression of the ventricular system, Mannitol was started and MRI brain was scheduled.
However patient suddenly deteriorated on the same day with acute onset of right hemiparesis, abnormal movements of upper and lower extremities, so an urgent MRI showed findings compatible with meningoencephalitis including ischemic components associated with thrombophlebitis (partial vein thrombosis) involving the superior dural sagittal venous sinus and internal cerebral vein near the great vein of Galen Figure 2.
Neurosurgeon was consulted and phenytoin started. EEG was abnormal revealing Theta waves alternating with polymorphic Alpha waves and consistent with brain injury. MRV was significant for endoluminal filling defect involving the superior sagittal venous sinus consistent with partial vein thrombosis and also mild narrowing at the union of great vein of Galen and internal cerebral vein, coagulation studies came back normal. The patient was kept under close observation and monitoring in PICU, he was on room air with no respiratory distress, stable hemodynamically with persistent fever, echocardiography, abdominal CT scan were normal. Neurologically, the patient improved gradually over the following 2 weeks and regained his normal level of consciousness and most of his sensory and motor power on the right side. MRI repeated after 12 days showed partial regression of the previous findings. Although clinical improvement was obvious, fever persisted, viral meningitis panel (whole blood multiplex real time PCR) was positive for Human Herpes Virus 6. Table 1
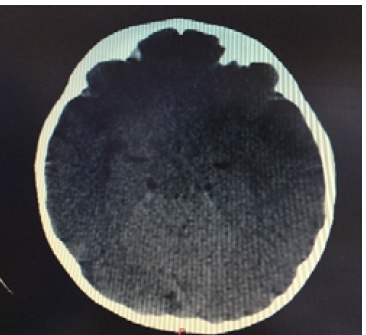
Figure 1: CT Scan of Brain Showing Total Enfacement of the Brain Tissue with no Evidence of the Sulcal Pattern

Figure 2: MRI Brain Showing Findings Compatible with Meningoencephalitis Including Ischemic Components Associated with Thrombophlebitis (Partial Vein Thrombosis) Involving the Superior Dural Sagittal Venous Sinus and Internal Cerebral Vein Near the Great Vein of Galen.
Table 1: Viral meningitis panel (Neuro 9) positive for HHV6
Virus | Presence of Nucleic Acid (+) / Absence of Nucleic Acid (−) |
HSV1 | − |
HSV2 | − |
VZV | − |
EBV | − |
CMV | − |
HHV6 | + |
HHV7 | − |
Adenovirus | − |
Human parvovirus | − |
Human enterovirus | − |
Parvovirus B19 | − |
Patient received 20 days of IV antibiotics and Acyclovir and was discharged home after resorption of fever and almost total recovery of neurological functions.
Viral infection of the brain leads to meningitis, meningo-encephalitis, or encephalitis, in descending order of frequency [2]. Encephalitis is the inflammation of the central nervous system parenchyma and is manifested by neurologic dysfunction with symptoms like altered mental status, behavior, or personality; motor or sensory deficits; speech or movement disorders; seizure; hemiparesis; and paresthesis [4]. Human herpesvirus 6 (HHV-6) is the common collective name for Human betaherpesvirus 6A (HHV-6A) and Human betaherpesvirus 6B (HHV-6B), two of the nine herpesviruses known to have humans as their primary host [5]. They are double stranded DNA viruses within the Betaherpesvirinae subfamily and of the genus Roseolovirus [6]. HHV-6 was identified as the causative agent of the common childhood disease Roseola Infantum (Exanthem Subitum, also called Roseola or sixth disease) [7]. Encephalitis of variable severity can occur as a complication of Roseola or as the primary manifestation of HHV-6 infection in otherwise immunocompetent hosts [8-13]. In immunosuppressed hosts, reactivation is associated with a worse outcome such as encephalitis, hepatitis, or graft rejection. In immunocompetent hosts, this persistent infection is generally of no consequence [14]. However, HHV6 associated meningo-encephalitis in immunocompetent patients has been described in only few case reports with not well-defined incidence and clinical syndrome. A study conducted in 2020 on nine patients positive for HHV-6 showed the following results: three (33.3%) had encephalitis, three (33.3%) had meningitis, one (11.1%) had complex febrile seizures, and two (22.2%) had fever alone. All patients with HHV-6 and encephalitis had neurologic sequelae. Two cases were reported in 2018 and 2020 about pediatric patients who died because of HHV-6 encephalitis due to associated brain edema [15,16]. In 2000, Taferner et al., reported four cases of encephalitis with refractory brain edema treated with craniectomy [17]. To the best of our knowledge, this is the first case of pediatric meningo-encephalitis caused by HHV6 infection, associated with brain ischemia due to thrombophlebitis and with mild neurologic sequelae. Our patient presented with altered mental status and fever and soon after deteriorated with new onset right hemiparesis, imaging showing signs of meningo-encephalitis, brain edema and partial vein thrombosis with normal coagulation studies. All the studies reported that early treatment with antiviral agents and immunomodulatory agents (e.g., steroids, IVIg) [18] and immediate management of brain edema are essential for the survival of the patient affected by HHV6 meningo-encephalitis. The baby in this case improved with treatment consisting of acyclovir, corticosteroids and Mannitol and regained almost normal neurologic function.
HHV6 infection is not always benign and complicated courses of the disease should be considered in children with neurologic symptoms, treatment should be started in early stages to prevent poor outcome.
Ansari, A. et al. “Human Herpesviruses 6 and 7 and Central Nervous System Infection in Children.” Emerging Infectious Diseases, May 2002.
Whitley, R.J. “Viral Encephalitis.” New England Journal of Medicine, vol. 323, no. 4, 1990, pp. 242–250.
Reynaud, J.M. et al. “Human Herpesvirus 6 and Neuroinflammation.” Hindawi International Scholarly Research Notices, 2013, https://doi.org/10.5402/2013/834890.
Cherry, J.D. et al., editors. “Encephalitis and Meningoencephalitis.” Feigin and Cherry’s Textbook of Pediatric Infectious Diseases, 6th ed., Saunders, 2009, p. 504.
Adams, M.J. et al. “Ratification Vote on Taxonomic Proposals to the International Committee on Taxonomy of Viruses (2012).” Archives of Virology, vol. 157, no. 7, 2012, pp. 1411–1422.
Jaworska, J. et al. “Divergent Susceptibilities of Human Herpesvirus 6 Variants to Type I Interferons.” Proceedings of the National Academy of Sciences, vol. 107, no. 18, 2010, pp. 8369–8374.
Yamanishi, K. et al. “Identification of Human Herpesvirus-6 as a Causal Agent for Exanthem Subitum.” The Lancet, vol. 331, no. 8594, 1988, pp. 1065–1067.
Ahtiluoto, S. et al. “In Situ Hybridization Detection of Human Herpesvirus 6 in Brain Tissue from Fatal Encephalitis.” Pediatrics, vol. 105, no. 2, 2000, pp. 431–433.
McCullers, J.A. et al. “Human Herpesvirus 6 Is Associated with Focal Encephalitis.” Clinical Infectious Diseases, vol. 21, no. 3, 1995, pp. 571–576.
Ohsaka, M. et al. “Acute Necrotizing Encephalopathy Associated with Human Herpesvirus-6 Infection.” Pediatric Neurology, vol. 34, no. 2, 2006, pp. 160–163.
Mannonen, L. et al. “Primary Human Herpesvirus-6 Infection in the Central Nervous System Can Cause Severe Disease.” Pediatric Neurology, vol. 37, no. 3, 2007, pp. 186–191.
Crawford, J.R. et al. “Human Herpesvirus 6 Rhombencephalitis in Immunocompetent Children.” Journal of Child Neurology, vol. 22, no. 11, 2007, pp. 1260–1268.
Provenzale, J.M. et al. “Clinical and Imaging Findings Suggesting Human Herpesvirus 6 Encephalitis.” Pediatric Neurology, vol. 42, no. 1, 2010, pp. 32–39.
Marseglia, L. et al. “Human Herpesviruses-6 and-7 Encephalitis in Immunocompetent Infants: Are They Really So Uncommon?” Journal of Biological Regulators and Homeostatic Agents, vol. 30, no. 4, 2016, pp. 1131–1136.
Miyahara, H. et al. “Unique Cell Tropism of HHV-6B in an Infantile Autopsy Case of Primary HHV-6B Encephalitis.” Neuropathology, vol. 38, no. 4, 2018, pp. 400–406.
Sevilla-Acosta, F. et al. “Human Herpesvirus 6 Associated Encephalitis with Fulminant Brain Edema in a Previously Healthy Child.” Cureus, vol. 12, no. 5, 2020.
Taferner, E. et al. “Craniectomy in Severe, Life-Threatening Encephalitis: A Report on Outcome and Long-Term Prognosis of Four Cases.” Intensive Care Medicine, vol. 27, no. 8, 2001, pp. 1426–1428.
You, S.J. “Human Herpesvirus-6 May Be Neurologically Injurious in Some Immunocompetent Children.” Journal of Child Neurology, vol. 35, no. 2, 2020, pp. 132–136.
