
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9475
ISSN (Online) : 2788-9483
Utilisation of Tuberculosis (TB) Manyatta centre (an inpatient TB centre based treatment model for nomads) by the Turkana nomadic population has been one of the TB control strategies implemented by the Kenyan government to accommodate TB infected nomadic patients in order to reduce TB morbidity and mortality. The utilization of this centre has been declining; this has prompted to find out what has led to this low utilization? The study aimed at identifying factors associated with the low utilization of TB Manyatta centre by Turkana nomadic pastoralists and the literature review was undertaken in objective to establish the potential contributing factors to the low uptake of Manyatta. Quantitative observational case control design was used and the study population the researcher was interested were TB patients admitted in Lodwar Hospital TB program from January 2008 to December 2012. The information from TB registers, TB Manyatta register and TB reports were accessed, and a total of 1382 TB patients sampled. The systematic sampling method produced 526 TB patients that utilized Manyatta and 856 for not used. The Univariate Odd ratios (OR) for each variable were calculated, and multivariate analysis performed indicated that gender, distance, marital status and education level as demographic factors that influenced the like hood of utilization of Manyatta. The study find out that The Multivariate odds ratio for educated patient was at 0.35 (95% CI 0.13 - 0.94), the 0-50km distance 0.25(95%0. 10-0.72), male gender 3.14(95% CI 1.98-4.97) and married patients OR being 0.17(95%0. 06 -0.47). These variables showed a statistical significance. The researcher recommends the Kenyan ministry of health to intensify health education on TB treatment literacy, construct Manyatta nearer to nomadic dwellings, roll out health generic strategies within nomadic pastoralists population that promote health among the female population, work against cultures that prohibit accessibility of TB services by non-married women and ensure services are women-friendly.
Tuberculosis (TB) has remained the single most infectious disease, with high mortality and morbidity worldwide, and its control and management has persisted as a tremendous challenge in the sub-Saharan African Countries [1], thus forming a vital public health problem that retards development in low-income settings [2]. TB care and its management are further complicated by the presence of a large untreated population who seek treatment late or don’t come for treatment and go undetected [2], therefore presenting a reservoir of infection.
One of these risk groups is the migratory population: the nomadic pastoralists with a mobile lifestyle who move across the volatile borders of different countries looking for grass and water for their livestock. The WHO recommended direct observation treatment (DOT) strategy for TB management [3] had been impractical in nomadic pastoralist settings [4-5]. Therefore, finding other innovative TB care strategies for this mobile population, like use of TB Manyatta centre (a centre based treatment model for nomads), that ensures prompt adherence to treatment is vital to ensure better TB patient and programme outcomes.
Tuberculosis was the first infectious disease declared by WHO as a global health emergency according to Kochi [6] and it has remained a public health problem in many low-income nations [7]. By 2007, Africa alone constituted 86% of all cases of TB [3]. According to WHO [8], 6.1 million cases of TB were reported in 2013 to WHO with an estimated 9 million people having developed the disease and 1.5 million deaths reported. Because TB has an enormous public health impact to the population, it has remained among the three top communicable diseases targeted on millennium development goals (MDGs) according to WHO [2], therefore different national TB programs have intensified their efforts in developing strategies on a wider scale to ensure the improvement TB care, although the challenge has remained in containing TB in pastoralist nomadic population who lag behind according to Tanner [9].
Despite the Kenya division of Leprosy, TB and Lung disease (DLTLD) department implementing a comprehensive TB control strategy in place [10-11], an average of 10% increase in incident TB cases has been observed over the last decade in Kenya and is associated mainly with poverty according to Gillespie et al. [12]. WHO [13] suggests that this poverty remain the primary cause of global disease burden, mortality and enormous health inequalities between and within countries. Kenya is an eastern African country, having a population close to 40 million people [14] with about 60% of its population living in remote parts of the nation. It’s an ethnically diverse with 42 ethnic groups according to Mgomella et al. [15]. In 2010, the new constitution enabled the creation of the total 47 counties in Kenya to decentralize public services.
Kenya ranks 13th out of the 22 most burdened countries with TB in the world [1]. By 2012, incidence of TB in Kenya was at 66/100,000 persons while that of Turkana county (a larger county bordering Uganda, Ethiopia and South Sudan in the northwest part of Kenya) was at 79/100000, thus a high TB incidence in a setting where the nomadic population struggle to gain access to TB care according to WHO [1]. Stephen suggests that pastoralists constitute about 70% of the total population in the Horn of Africa while USAID [16] estimates 20% of the Kenyan population to be nomadic pastoralists, with that of Ethiopia being 12%, South Sudan 60% and 70% of the Somalia population. In such settings where the nomads move across the borders, access to essential health services according to Cambanis et al. [17] is reduced, hence TB care is ultimately compromised and nearly absent [18].
Many nomadic TB patients do live far from the available treatment centres [19], therefore, they do not go for treatment when sick according to Bam et al. [20] and instead opt for accessible traditional healer’s treatment according to Chatterjee et al. Turkana County in North West of Kenya (the research setting) with a mobile population has a population estimated to be 939,080 people [21] of whom 90% of its population live in the remote rural areas that lack infrastructure and practice a nomadic pastoralist way of life. Such nomadic communities according to Melaku, et al. is usually geographically isolated and often lacks awareness, a factor that affect their health seeking behaviour.
The above trend has been seen in many TB control programs with the nomadic pastoralist communities in the horn of Africa including Kenya, who have never recognized this risky mobile population as a priority [22], while the health of this group is usually inadequate. Therefore, the Stop TB Partnership targets of a 50% reduction by 2015 [8] cannot be quickly realized. The post-2015 Global TB strategy aiming at cutting new TB cases by 90% between 2015 -2035 and reducing TB death by 95% [8,23] cannot also be realized if no attention is focused on this mobile population with TB.
The Kenyan ministry of health is administered from top down in a hierarchical structure [24], where at the lower level there are dispensaries, followed by health centres, district hospital, provincial then finally the national hospital in that order. There is a pyramidal referral system from lowest peripheral clinic level in the rural areas of the highest national referral hospital [25]. By 2008, the Kenyan government owned about 71% of health facilities and the rest remained in faith-based organisations with funding of the public health sector ranging between 6-8% of total government spending according to annual health sector statistics report [26]. This Kenyan public financing is far less than the 2000 Abuja Declaration target of 15% [27-28].
Therefore, to get closer to the above goal, WHO [1] and Gothi [19] have both proposed and supported the TB strategies like Manyatta centres utilization, a wider involvement of community health workers, private practitioners’ participation and proper management of drug-resistant TB.TB care in Kenya is a vertical program with treatment and follow-up being done in TB clinics, and any TB suspected patient is usually seen by a clinician and if TB is diagnosed by chest x-ray or laboratory test, then the TB sick patient is referred to TB clinic for further management per TB guidelines [30].
In strengthening DOTS strategy, TB in Turkana with a nomadic pastoral population integrates the Manyatta strategy introduced by the Kenyan government between 1984 -1986 according to Zachariah, et al. [31]. Nomadic pastoralists with TB are expected to stay within this Manyatta centre during the initial phase of treatment; complete their treatments plans without a break in the treatment protocol and later are discharged to the nearest peripheral TB treatment centres during the continuation phase [32].
Though the peripheral health structures in Turkana do provide free TB treatment, they are far from the mobile populations and their migratory routes, are not well equipped; suffer frequent TB drugs shortage and tests, no TB isolation facilities and are poorly staffed with no proper supervision for TB programs and coordinated referral systems. Moreover, available medical mobile clinics aiming to reach the mobile population in isolated settings are faith-based owned and charge patients for medical consultations and referrals and provide no TB services. TB Manyatta centre (the only available in Turkana County) at the same time according to Ndirangu [33] has been poorly coordinated, especially in the areas of admissions of patients, diagnosis, and referral and counter reference to the treatment centres. Manyatta centre is separated from the rest of Lodwar district hospital departments.
TB-infected Pastoralists patients are managed using DOTS together with TB Manyatta centre strategies [32].
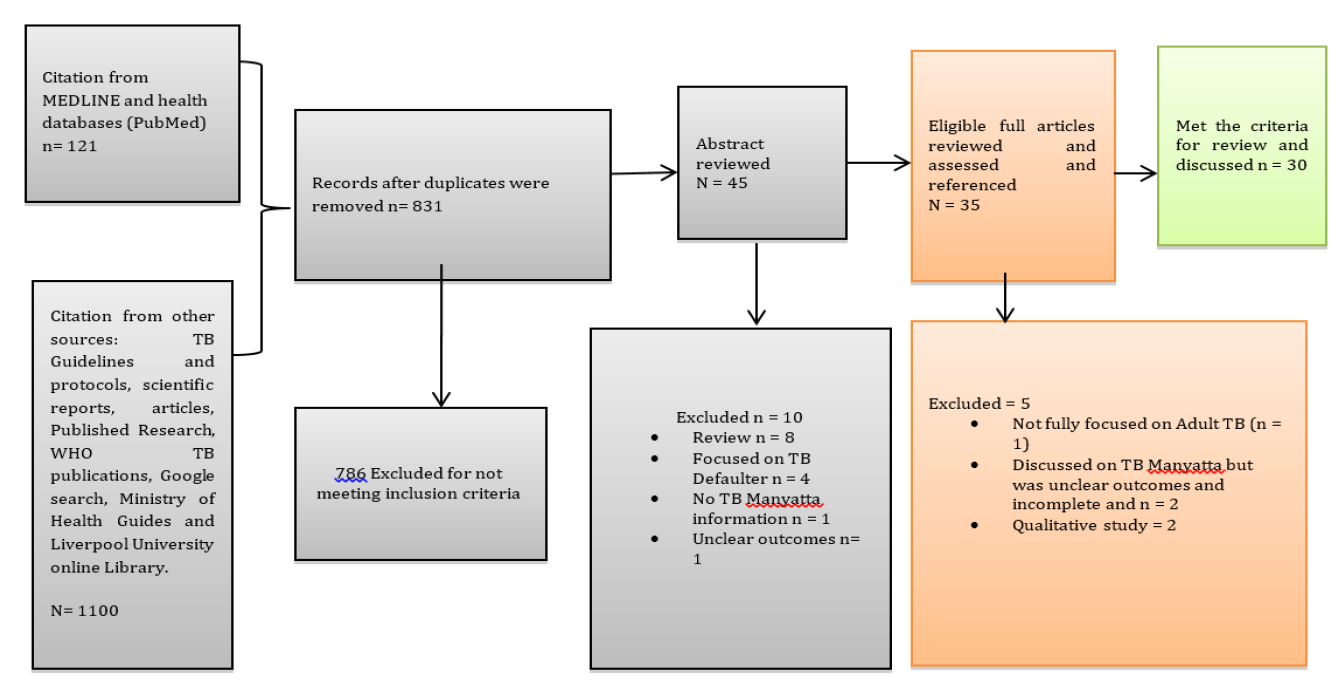
Figure 1: Flow Diagram of Study Identification, Screening, Eligibility, and Inclusion Process
Other aspects of the TB Manyatta centre focus on the provision of opportunities for counselling, health education, treatment compliance and food [31]. However, the above TB Manyatta centre in Lodwar (the capital of the Turkana County) admitted 1525 TB patients [32] between January 2008 and December 2012, and the scale of admissions decreased towards 2012 (358 TB patients in 2008, 435 in the year 2009, 415 in 2010 and 213 in 2011 and 86 TB patients in 2012). The total number of health workers in Lodwar district hospital is below 250 staff, the number recommended by WHO [8] for a population of 100,000 people.
Public health sees the affected community as a patient and focuses on ensuring that its health needs are adhered to [34]. This requires according to Wright [35] involvement in all aspects of health (both medical care for treatment and prevention of illness, physical, environmental, social and mental health) and taking health as a fundamental human right, and confirming health for all concepts that every country has an obligation to its population regarding public health. According to Hmama [36], TB affects millions of people and if left untreated, a pulmonary sputum positive TB patient can infect close to about 15 other persons in a year, therefore making this infectious disease an important public health problem to tackle.
The Turkana TB infected nomadic patients frequently move across volatile borders and rarely access health care services because they are far [19]. Access to TB treatment in such settings according to Zachariah, et al. [31] is usually compromised and, or absent, interrupted and not completed if a patient had started it. The nomadic pastoral TB patients, therefore, remains the reservoir of infection and continuous transmission of the disease across the borders. TB-infected nomadic patients, with a mobile lifestyle according to Melaku, et al. can then continue to infect many if untreated. Therefore, inadequate utilisations of TB care strategies within this mobile population are worthy of study.
Moreover, the TB Manyatta strategy started for this mobile population has seen a severe decline in attendance. Therefore, the researcher prompted to ask and find out what has led to this low utilization of TB Manyatta centre by the Turkana nomadic TB patients?
As Burns and Grove [37] suggests, the primary purpose of literature review, first of all, is to notify the researcher on what is already known about the topic in order to avoid repetition, thus maximizing the available resources. The retrieval of the literature review was done to find out the contributing factors to low utilization of TB Manyatta centre and the search was conducted for documents available only in English. Other varied literature studies on TB Manyatta taken from different countries for comparison purposes were also considered and explored. Moreover, in order to receive and utilise a more up to date research, the inclusion criteria were literature in TB care for nomadic pastoralists, recent TB publications from 2005– 2015, TB Manyatta publications from 1995 –2015 and other adult TB studies ethically approved. An exclusion criterion was language, as only literature in English was explored.
The literature review therefore, integrated and synthesized evidence from empirical TB studies, scientific reports, published research, scientific reports and several other sources consulted including WHO TB publications, PubMed health databases, Turkana county quarterly and annual TB reports, Google scholar and Internet, several ministry of health TB protocols and guidelines, TB publications, research and medical books, latest relevant TB journals and Liverpool University online library utilizing the key terminologies (Annex 3) but mainly on nomads TB care and Manyatta strategy. The web reviewed to illustrate different indicators was for WHO, Medicines Sans Frontiers (MSF), Kenya demographic health data and Kenya health information system (KIHS).The literature produced a vast, number of publications on Tuberculosis. Duplicates were removed, and abstracts reviewed with eligible full articles being retrieved and assessed, and to ameliorate the precision of the search, a combination of terms was used.
This strategy produced 1221 results of which 25 articles, 3 international and national reports and 2 reports met the inclusion criteria for review (for the reason of little research on the Manyatta strategy) as indicated in the Figure 1 and the rest of articles (1191) dropped.
The Process of Literature Review Study Selection
Little literature is available online and documented on TB Manyatta strategy, and this strategy has been implemented mainly in Kenya, south Sudan and Ethiopia through humanitarian organisations [31]. The Turkana TB Manyatta strategy by the Kenyan government has never been investigated at all or researched both for its impact or what need to be improved since its establishment and this gap of knowledge on its utilization outcome prompts an investigation into its recent decline in usage.
Nevertheless, a descriptive study in a similar context with nomads in South Sudan where Medicines Sans Frontiers (MSF) implemented the TB Manyatta strategy, the study concluded that many of the TB patients preferred to stay outside the TB Manyatta centre and only attended for treatment and food ratios [38]. The recommendation from the study focused mainly on understanding TB Manyatta utilization approach in another context than South Sudan, therefore this study formed a credible base to understand and consider other alternatives or adaptations to a centre based treatment model for nomads (TB Manyatta centre) that are inpatient in nature. Estifanos et al. conducted an extensive experimental study using a community randomized trial to find out TB case finding within the community, concluded that it was not possible to determine the extent of case finding for smear-positive TB patient but rather the speed of knowing the smear-positive patients was evident in such communities.
Ndirangu [33] later conducted a survey in seven DOTS centres in Turkana County to investigate causes of late TB treatment seeking in nomads, and found factors relating to stigma amongst 71% of them. The study recommended that an assessment be undertaken to determine how the TB case detection barriers among the pastoralist nomadic population could be reduced. In a cross-sectional study by Gele and Bjune [18] on armed conflict impact on spread of TB in the Somali regional state (SRS) of Ethiopia with similar nomadic population showed that TB patients in conflict zones of the SRS of Ethiopia have a higher rate of delay in diagnosis of TB and self-treatment before diagnosis than patients from non-conflict areas. They recommended user-friendly DOTs in conflict zones through local communities’ empowerment and acceptance of medical humanitarian organisations to access such volatile regions to ensure access to TB care services. These study findings and recommendations are convincing and practical given that DOT strategy is impractical for the mobile population, similar to the study context.
However, a more recent descriptive study by Zachariah, et al. [31] that investigated the experience of implementing a TB village for pastoralist populations in Cherrati in Ethiopia, found out that nomads preferred pastoralist’s lifestyle adapted TB village structures and to live together with their animals around the TB centre, thus were more likely to attend the centre. Their recommendations included an analysis of a TB Manyatta approach to determine resource requirements how best to maximize outputs. This study discussed on all aspects of TB village (similar to TB Manyatta) implementation framework and lessons expected during its implementation in any given setting, thus a chance to understand holistically what a TB village entails.
A similar quantitative study by Melaku et al. on pastoralist’s community perception of Tuberculosis in Shinille area of Ethiopia concluded also that small knowledge about TB among pastoral community affects the uptake of TB services and advised the regional health bureau to discover ways of ameliorating pastoral education on TB and create positive attitudes to avoid discrimination of infected individuals within the community. The different factors that may contribute to low utilization and outputs in terms of the levels of TB patients receiving services from the TB Manyatta centre in the Turkana nomadic pastoralism context have not been explored as mentioned above. Therefore there is a need to assess if socio-demographic factors, clinical characteristics such as adherence, drug side effects and the type of TB (relapse, failure, treatment after default) are associated with the utilization of services and the reported decline.
The above Ndirangu [33] study, in the same research context, was mainly qualitative; it was never discussed much in the nomadic population setting and never mentioned the Manyatta strategy. It however, identifies the methodology of the study as only a cross-sectional survey without indicating clearly the study design. The method of choice of the sampled seven DOTS centres was, however unclear, the data collection process and analysis were mixed between qualitative and quantitative making it confusing for the findings of the research. No information on research approval was mentioned with study findings and results are unable to be verified. Thus, making the study findings risky to be utilized. Despite the flaws identified in this study, the results of this study are the only indication that we have had a TB research in the study setting.
Similarly, the above Zachariah et al. [31] study in TB village in nomadic setting of Ethiopia also applied qualitative method of study by analysing secondary data; nevertheless, the researcher strongly apprehends this study because the design and methodology utilized was appropriate for the research aim, researchers obtained an approval of research and did correct analysis. However, though the sample frame and sampling method was not clear, the data were valid with the results and discussions entirely touching on Manyatta. A future study was also proposed, and the objective of the research was met. Therefore, due to the large sample size, the validated data collection and the precise sampling strategy, the findings of this study are convincing and acceptable; however, the time limitation of the study means that further investigation is still required .The results of the study, therefore, are firm because the study was without major flaws.
Gele and Bjune [18] and Melaku et al. studies on armed conflict impact on spread of TB in the Somali regional state (SRS) of Ethiopia were cross-sectional studies, utilized structured questionnaires, obtained research approval and did correct analysis. It further provided a recommendation. Though the study mainly discussed on the TB care challenges within the pastoral community and less of TB Manyatta strategy. The findings should still be accepted despite the flaws identified in the study because the large sample size, validated data collection and an explicit sampling plan were utilized. The results are convincing and further identified the exact cause of delay to treatment in a nomadic pastoral setting (similar to the research setting of Turkana). However, the time limitation of the study means that further investigation is still essential.
The study findings by Estifanos et al. discussed smear-positive TB patient and never touched on any aspect of TB Manyatta strategy. The study utilized experimental study design that applied randomized control trials with no specific information if the research consent was obtained or not, and it, however, used a selected population with no clear sampling strategy. The recommendation provided was not clear enough to be adapted. Therefore, these findings are not convincing, and they should be ignored. The literature review therefore strongly supports and recommends the use of TB Manyatta that can at the same time fill the gap where access to TB care is a problem [31,5]. Determining the cost of running Manyatta to maximize its output has been recommended by Zachariah et al. [31] but due to time and budget limits, this recommendation could not be followed and researched.
Nonetheless, in understanding the limitations of many of the studies [39] including incorrect process of sampling and lack of study approval followed (particularly in Ndirangu study discussed above), only one side of the behaviour influences was mainly assessed, making it difficult to understand the research question for contributing factors to low utilization TB Manyatta by Turkana nomadic TB patients [40]. No single one indicator, therefore, can be used to all the setting and it will be advisable then to find out setting specific causes of the low uptake of Manyatta [41]. At the same time, studies included in the literature review were mainly qualitative, and they did not quantify the usage of the Manyatta.
From the above literature review, little is known, researched and documented on TB Manyatta strategy globally and for Turkana TB Manyatta centre. Manyatta concepts about the nomadic pastoralist community’s perception practice regarding TB and social-cultural beliefs according to Ndirangu [33] have not been well documented and evaluated in Kenya. With an exception to Ethiopian, TB Village discussed above having similar characteristics to TB Manyatta centre, not much literature is available on this Manyatta concept. Therefore, better understanding of Turkana nomadic pastoralist population perception and specific context barriers to the utilization of the TB Manyatta centre through research investigation is required. This will not only provide a broader picture of TB control activity in the Turkana County, but also be of immense value in the planning and implementation of TB control programs [18]. It will further help and enhance the development of strategies and policies that are aimed at improving the quality of TB services within this complex setting of the nomadic population.
Despite the fact that the above literature review strongly supports use of TB Manyatta that can fill the gap where access to TB care is a problem [31], with all the literature reviews on TB Manyatta strategy, there is an enormous lack of accurate information on factors that lead to decline of utilization of Turkana Manyatta, this is mainly because no investigation has ever been done on this Turkana TB Manyatta centre thus an enormous gap in knowledge and practice. Therefore, being the first study of the kind in the setting, the author would like to find out what has then caused this decline in utilization of TB Manyatta centre?
The Question, Aim, Objective and Epistemological Approach
Research Question, Epistemological Approach and Positionality: The research question was on what factors determine the low utilization of the TB Manyatta center by the Turkana nomadic TB patients, as measured by the differences in the levels of TB patients, admitted to TB Manyatta center and those entered in the TB program in Turkana County? The assumption of this research was that social, cultural demographic factors of the mobile population lead to low uptake of TB Manyatta.
The study uses positivist epistemology approach that assumes there is an external objective reality that can be measured without influence of the researcher, using a quantitative method to measure the determinants of the low utilization of TB Manyatta by the nomadic pastoralist TB patients. According to Williams, this approach assumes that there is an existence of an observable reality, which can be revealed through statistical analysis of existing data. Therefore, this study strives to investigate a mathematical relationship between utilization of TB Manyatta strategy in Turkana and individual characteristics of the environment and individuals [42], hence appropriateness of this quantitative methodology. This study, therefore, assumes that the objectives regarding the differences observed in the utilization of TB Manyatta strategy in Turkana can be derived through analysis of statistics on TB Manyatta utilization and chosen environmental and individual factors.
Nevertheless, as the uses of ecological approaches that utilize cumulative information provide only data on groups of interest and not to the individuals that constitute the group according to Spicker, the ecological fallacy can result, thus they are not appropriate to use. This result that can be that any relationship seen from aggregated data may not certainly exist at the individual level [42]. Williams and Bryman [43] further suggests that this approach does not reveal causality but rather only associations. For instance, quantitative ecology studies according to Adamu [44] only indicate the strength of associations between gender and use of TB Manyatta centre; this is because the association cannot be presented. This will then require a further study of qualitative nature to determine the ‘why and how’.
The qualitative approach can be an option and utilized in this topic related to behaviour and choice but the selection of this positivisms epistemology here is to quantify the utilization of the TB Manyatta and unlike in interpretive epistemology which according to Green and Thorogood [45] will not quantify the use of TB Manyatta by just observing the situation, perceiving it or by just taking note. The interpretivism epistemology approach according to Bruce et al. [42] is based on the idea that reality is based on the views of individuals and changes and not the case of this quantitative research.
To study aimed to study the factors associated with the utilization of TB Manyatta centre by nomadic pastoralists in Lodwar district hospital, Turkana County in Kenya to determine potential contributing factors to low uptake.
Objectives
The specific objectives of this study were to undertake the literature review on nomadic pastoralist TB care and establish potential contributing factors to the low uptake of TB control programs within pastoralism nomadic context , to collect secondary data on TB patients utilizing TB Manyatta and those not utilizing it and analyse demographic and clinical TB data of both nomadic pastoralist TB patients in the Manyatta and from every TB patient admitted to Lodwar district hospital , to describe the social, demographic characteristics of the two groups of TB patients using secondary data and their perception and barriers leading to low utilization of TB Manyatta, to undertake inferential analysis to understand patterns in data and relationship between intervention and outcome for both TB patients who utilize and those who do not utilize and to make recommendations on TB Manyatta strategy to Lodwar district hospital management team (DHMT) and Turkana county health authority to improve TB care of nomadic pastoralist TB patients.
Research Outcomes
It is expected that the study will contribute to better understanding of TB Manyatta strategy, current issues surrounding its low utilization and contribute to the policy change for the care of TB nomadic population.
Sampling Procedure, Data Collection Instruments and Data Analysis
Study Design: This quantitative study used observational, case-control design using secondary data to assess the factors for the low uptake of TB Manyatta strategy by the Turkana nomadic TB patients in Turkana County. Though case-control design has a problem to collect information on past exposures, the rationale for the choice of this model was mainly because it is both faster and cheaper to conduct according to Bland, [46] and Gordis.
Study Setting and Population
The population forms the individual the researcher is interested in studying [37] and in this study they are TB patients who utilized the TB Manyatta centre and those who did not utilize Manyatta in Lodwar district hospital.
Sample Procedure, Sample Frame, and Sample Size
Sampling involved selecting individuals from a population to be studied [37]. The procedure included all 6909 TB adult (>18 years) patients admitted to Turkana TB program from January 2008 to December 2012 (data dates) as inclusion criterion because Turkana Manyatta centre lacks children’s facilities.
The sampling frame according to De Vos et al. [47] is purely the whole list of members of a population from which the study participants can be selected and in this study; it is the full details of TB patient’s data available in the TB reports and the TB register of Lodwar district hospital. Particulars in the TB register included TB patient name, age, sex, when treatment started and stopped date, whether admitted into TB Manyatta centre, origin to indicate the distance to Manyatta centre, religion, ethnic group, employment status, classification of TB, treatment available or not, marital status, family support, education level, status of HIV, TB type, results of sputum examination in different month.
Larger sample sizes increases chances of precision [37] and the researcher followed the recommendation by De Vos et al. [47] that cited in Stoker’s guidelines for sampling and sample size that the sample need to be between 20%-32% for populations of 200-500. Therefore, taking a minimum of sample size of 20% of the 6909 patients admitted into TB program of Lodwar district hospital, a total of 1382 TB patients were sampled and systematic sampling method was utilized by picking every 5th record. This produced 526 (38%) for those who used TB Manyatta centre and 856 (62%) for those who did not utilize. This method of sampling according to Black [48] saves cost, time and is simple to use, with the researcher sure of the target study population being eventually sampled.
Data Collection Procedure
The source of information was accessed from Lodwar county TB register, TB Manyatta centre register and Turkana district TB reports obtained directly by the researcher by visiting the sites after being given the permission to conduct the study by the hospital authority. Data information on variables recorded and was ready for cleaning and analysis. The Figure 2 indicates the procedure followed during the data collection, and it occurred over two weeks from 3rd March 2014 to 20th March 2014.
As this study uses a secondary data based approach, there was some difficulty in ascertaining how the data components were initially gathered and inserted in the TB register. The secondary data collection choice was because the merits of the data; they provide a faster, cheaper and easier means of obtaining required larger samples.
The study data was only collected from good quality and well-kept instruments (TB register, TB Manyatta register and the TB reports), officially used by Lodwar district hospital to transmit data to higher government level. These instruments were accurate in the content, consistent, efficient and could be replicated. Therefore, the data collected was adequate and relied on because it measured its intended purpose [49]. Stommel and Wills [50] suggest that such instruments if valid are efficient for the researcher to make acceptable judgements. This reliability according to Makhanu [51] is essential for any effective data collecting procedure.
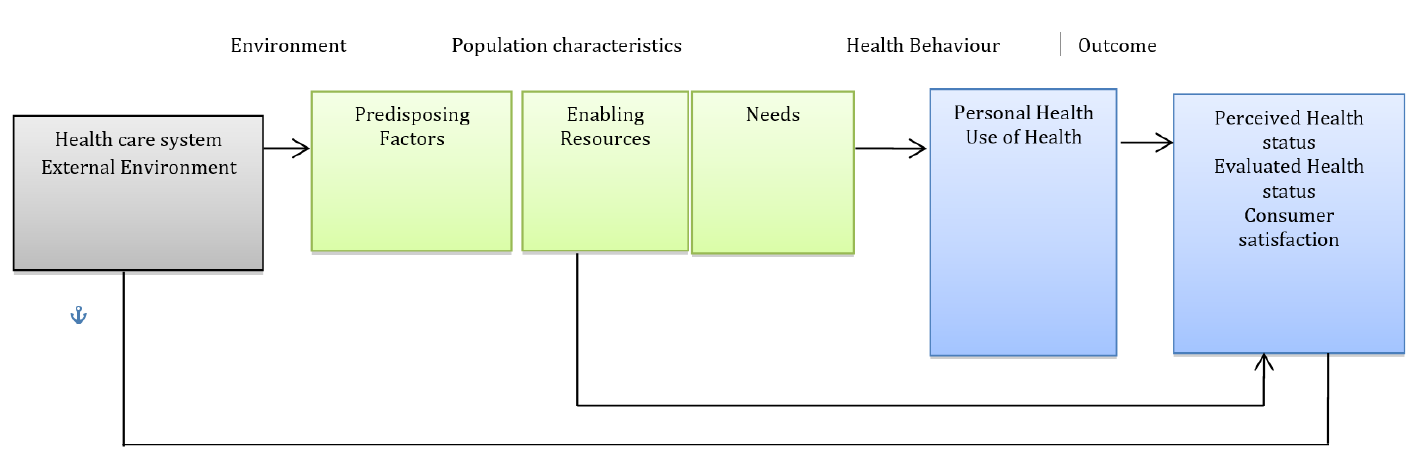
Figure 2: Andersen and Newman Framework of Health Services Utilization
Ethical Consideration and Approval
Ethical approval for this study was granted by University of Liverpool and later from Lodwar district hospital (annexes 2). Confidentiality ensured by not revealing the identity of any TB patient’s file or persons, data was de-identified before transferring into the computer, and the data will be kept for five years. The right of TB patients whose data was collected was not violated, and the researcher observed strict ethical standards as required in the study according to Burns and Groove [37].
Conceptual Framework
The patient’s non-utilization of the Manyatta is a complex behavioural issue involving multiple factors ranging from the interaction of personal, social to health care factors according to Andersen [52]. This study used Andersen and Newman Framework of health services utilization [53], on which they suggested that utilization of a health service could be seen as a type of individual health behaviour and that the primary purpose of this framework is to try to discover the conditions that either facilitates or impedes utilization of services, in this case, utilization of TB Manyatta care, and the framework assures access to this medical care. The choice of this framework among others is mainly because it analyses the differences in health care services utilization from a social, demographic perspective [44]. Therefore, this framework is the best applicable for this medical problem.
People’s access and their utilization of health services are regarded to be a functioning of three elements namely predisposing, enabling and finally need factors, according to Andersen [52].
Predisposing factors according Andersen [52] form purely social cultural characteristic of individuals that exists prior to illness for example health belief, values or knowledge of population on TB, the existing social structure like education background of the patient, occupation, gender, age, ethnicity, social interaction and the culture of the population.
Enabling factors include the logistics issues of obtaining the care according to Andersen [52] and this form issues like patient means of accessing health care, their income, availability of health personnel and community available resources e.g. the numbers of health facilities available for the TB patients. Other issues in the community include origin of patient; this is because local norms and values in the community do affect individual behaviour towards use of health service Andersen [52], therefore, an important aspect and characteristics to be considered.
Andersen [52] elaborates need factor as the most immediate source of health service that comes from a health that are categorized either as perceived or evaluated needs. Perceived needs according to the author helps to understand how people view own general health, thus it relates to kind of treatment that will be provided when the TB patient’s presents to the healthcare provider and in the study it represents the kind of healthcare they will receive in the Manyatta centre.
Nonetheless, the definitive objective of this research remains to establish the contributing factors to low utilization of TB Manyatta centre by the Turkana nomadic TB patients within the Turkana nomadic context. The findings of this research will be directly in operational line for an improved TB control program on a pastoralism nomadic setting and provide a framework for better understanding Manyatta strategy.
The flow and the structure of the above framework were systematically applied when the data was collected, analysed and discussed starting with the predisposing factors, health-related factors and finally enabling factors.
Data Cleaning Missed Data and Analysis
No statistician was involved, and data collected from the instruments were arranged, tabulated and put into an Excel worksheet besides some information of some variables being collapsed because they were in excess of the study requirements. This includes, for example, the TB patient’s level of education and the employment status. TB patient employment status was written in the register as no money, own small business, wealthy and employed were collapsed into two levels by combining no money and own small business to reflect patient being not employed, and wealthy and employed to form the employed. Education was subsequently collapsed to range from non-educated, only lower primary, completed class eight and attended some secondary school, completed secondary and colleges to two levels namely educated and not educated. Using check codes in the database, data entry error were then minimized as the data was cleaned to ensure proper consistency (Table1-2).
TB patients’ information need to be systematically documented in the TB registers and reported in reports used in data collection this requires prompt supervision as also discussed in that the recommendations below.
Data on the drug side effects of all 1382 sampled patients missed and was not documented in the data collecting tools and only found in the individual patient files. The researcher reported it as absent hence was not accounted for any analysis. The unrecorded data was attributed to negligence. As the missing data could still be available (in the patient’s file), the researcher had not much time and cost to cross check all the files, the other data available was still valid.
Table 1: Different Dependent Variables
| Variable | Description | Type of Data variable |
| Number of health care providers | Number of health care providers available to TB patients. | Continuous |
| Availability of treatment | Yes or No. If TB patients received treatment or Not | Categorical |
| Family support or accompanied for | Yes or No. If the TB was accompanied to and during the treatment | Categorical |
| Drugs side effects | Yes or No. Proportion of patient who got any side effect during TB treatment | Categorical |
| Duration of Treatment | Mean duration of months the TB patients was on TB treatment. | Continuous |
| Number of Visits | Number of times the TB patient visited the TB Manyatta for treatment or retreatment | Categorical |
| Type of TB | Proportion of TB patient with either pulmonary or extra pulmonary | Categorical |
| Geographical distance (Kilometres’- km) | Coding of the distance in to Categories of the distance the TB patients covers to the TB Manyatta centre. | Continuous
|
| Number of reference to other centres | Mean number of referrals made from TB Manyatta to other treatment centres. | Continuous |
| Number of houses adapted to nomadic lifestyles | Numbers of houses build like traditional nomadic houses.
| Continuous |
| Classification of TB | TB classified as Pulmonary smears Positive and Extra Pulmonary TB and a Pulmonary smear Negative and Pulmonary smear Unknown. | Categorical |
Table 2: Different Independent Variables
| No | Variable | Description | Type of Data Variable |
| 1 | Age | Age Coding done in two cohorts of 18 – 50 years and > 51 years | Categorical |
| 2 | Gender | Coded for either male or female | Categorical |
| 3 | Patient Economic status | Coded as employed and not employed, | Categorical |
| 4 | Education Level | TB patient level of education Coded in order of Educated and Not educated | Categorical |
| 5. | Religion | Categorized as either Christian or Non-Christian. | Categorical |
| 6. | Ethnicity | Either as Turkana or Non Turkana | Categorical |
| 7 | Marital status | Coded as either married or Not Married. | Categorical |
Descriptive Analysis
By utilising the statistical package for social sciences (SPSS, version 21), the researcher utilized frequency and proportion to describe categorical variables to include age, gender, family support, availability of treatment, side effects, marital status, type and classification of TB, employment status and education level. The mean was used to describe continuous variables such as geographic distance to Manyatta, duration of treatment and structures adapted to nomadic lifestyle and time on treatment. Frequency tables generated from the above variables and bar charts were utilized to assist in the visual appreciation of social, demographic characteristics of TB patients for those utilizing and not using the centre.
The inferential analysis took place to observe if the pattern in the data analysis was due to intervention effects or not. Normality test was applied first for every continuous variable to examine their distribution [53]. To compare categorical variables mentioned above in two groups (utilized and not utilized), chi-square test was applied and was used to verify if two or more percentages are different [47]. However, in cases where the expected frequencies were also to satisfy assumptions of Chi-square, in the number of visits to TB Manyatta then Fisher’s Exact Test was applied.
Pearson Correlation test was undertaken for continuous variables (Porta [54] to assess the linear association between geographic distance and time for treatment. However some continuous variables that had small numbers like for health care staff, the number of reference to other centres and number of houses adapted to nomadic lifestyles could not be analysed. Univariate Odds ratio (OR) for each separate variable was calculated and a Multivariate logistic regression (MLR) model was applied to independent variables that were found to be statistical significant to include gender, ethnic group, and education level and employment status in order to provide with an adjusted odds ratios for each variable.
Positionality
Positionality of a researcher is one of the vital aspects to be taken into account in any research [55], this is because the investigator acceptance and own characteristics can have a far-reaching impact on research outcome [56]. The researcher in this study considered his own positionality; this according to Homfray [57] and Sultana [58] helped to check whether his characteristics affected the research or not, plus understanding the similarities and differences that existed between the researcher and the participants of the research. Nevertheless, the researcher of this study comes from the study setting, and the outcome could have been less accurate if the researcher were not from Turkana or even from the ethnic group of the study population.
Demographic Characteristics and Clinical Patients Data
One thousand and eighty-two TB patients were sampled for this study. The social-demographic and Clinical TB data factors included age, sex, ethnic group, marital status, religion, TB classification and Type of TB patient.
Table 3 shows a total of 38.1% utilization rate of Manyatta centre that is small and matches the study question of establishing why use is low. The table indicated that the older the TB patient, the higher the rate of utilization. More elderly patients had more utilization rate than the younger patient (41.3% for the patient above 51 years and 35.5% for patients of ages between 18 -50 years. The 18 -50 years old age Odd ratio (OR) was at 0.7816 (95% CI 0.6283 - 0.9724). The less < 1 OR for age variable indicated a negative association between Age variable and Utilization at the 5% significance level.
Female TB patients in the Table 3 utilized less Manyatta than male TB patients (33.5% for female and 41.1% for male). OR for the male category variable was at 1.39(95% CI 1.11-1.74) showing a statistical significance because it did not contain a 95% confidence interval for the OR 1.0 and male were 1.39 times more likely to use TB Manyatta than female.
Table 3: Indicating a Summary of Utilisation Rate and Univariate Odds Ratios (OR) of TB Manyatta among Groups According to Background Characteristics of TB Patients
| Background Characteristics | Utilized | Not Utilized | Total | Utilization Rate % | Univariate Odds Ratios and 95% Confidence Interval | |
| Number | Number | Percentage | Odd Ratios | CI | ||
| Age | ||||||
| 18 - 50 yrs. | 274 | 498 | 772 | 35.5 | 0.78
| *0.63-0.97
|
| > 51 yrs. ® | 252 | 358 | 610 | 41.3 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Gender | ||||||
| Male | 339 | 485 | 824 | 41.1 | 1.39
| *1.11-1.74
|
| Female® | 187 | 371 | 558 | 33.5 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Distance to Manyatta | ||||||
| 0 - 50 km | 401 | 236 | 637 | 63.0 | 8.42
| *6.55-10.83
|
| > 50 km ® | 125 | 620 | 745 | 16.8 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Marital Status | ||||||
| Married | 84 | 120 | 204 | 41.2 | 1.17
| 0.86-1.58
|
| Not Married ® | 442 | 736 | 1178 | 37.5 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Religion | ||||||
| Christian | 125 | 328 | 453 | 27.6 | 0.51
| * 0.39-0.64
|
| Non - Christian® | 401 | 528 | 929 | 43.2 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Education Level | ||||||
| Educated | 170 | 121 | 291 | 58.4 | 2.90
| * 1.03 - 2.71
|
| Not-Educated® | 356 | 735 | 1091 | 32.6 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Ethnic Group | ||||||
| Turkana | 518 | 844 | 1362 | 38.0 | 0.90 | 0.37 - 2.27
|
| Non Turkana ® | 8 | 12 | 20 | 40.0 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Type of TB | ||||||
| Relapse and Failures | 180 | 233 | 413 | 43.6 | 1.39
| * 1.10 -1.76
|
| New ® | 346 | 623 | 969 | 35.7 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Classification of TB diagnosis | ||||||
| Pulmonary smear + and Extra Pulmonary | 524 | 772 | 1296 | 40.4 | 28.51
| * 6.98 -116.38
|
| Pulmonary Smear - and Smear Unknown® | 2 | 84 | 86 | 2.3 | ||
| Total | 526 | 856 | 1382 | |||
| Availability of Treatment | ||||||
| Yes | 525 | 825 | 1350 | 38.9 | 19.72
| * 2.69 - 144.95
|
| No® | 1 | 31 | 32 | 3.1 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Family Support | ||||||
| Yes | 520 | 812 | 1332 | 39.0 | 4.70
| * 1.99 - 11.09
|
| No® | 6 | 44 | 50 | 12.0 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
| Employment status | ||||||
| Employed | 103 | 107 | 210 | 49.0 | 1.70
| * 1.27 - 2.29
|
| Not Employed® | 423 | 749 | 1172 | 36.1 | ||
| Total | 526 | 856 | 1382 | 38.1 | ||
® Reference category and * show statistical significance
Table 4: Multivariate Logistic Regression Analysis Showing Odds Ratios and Statistical Significance of Independent Variable
| Parameter Estimates | ||||||||
| Background Characteristics | B | Std. Error | Wald | Df | Sig. | Odds Ratios | Multivariate Odds Ratios And 95% Confidence Interval | |
| Age | ||||||||
| Age 18 - 50 Years | -1.66 | 0.68 | 5.98 | 1.00 | * 0.01 | 0.19 | 0.05-0.72
| |
| Age Above 51 Years ® | - | - | - | 0.00 | - | - | ||
| Gender | ||||||||
| Male | -0.18 | 0.48 | 0.14 | 1.00 | * 0.00 | 3.14 | 1.98- 4.97 | |
| Female® | 0.00 | - | - | |||||
| Marital Status | ||||||||
| Married | -1.77 | 0.52 | 11.70 | 1.00 | * 0.00 | 0.17 | 0.06-0.47 | |
| Not Married® | - | - | - | 0.00 | - | - | ||
| Education Level | ||||||||
| Educated | -1.04 | 0.50 | 4.31 | 1.00 | * 0.04 | 0.35 | 0.13-0.94 | |
| Not Educated® | - | - | - | 0.00 | - | - | ||
| Support Received | ||||||||
| Supported | 1.53 | 1.20 | 1.62 | 1.00 | 0.20 | 4.62 | 0.44-48.99 | |
| Non Supported® | - | - | - | 0.00 | - | - | ||
| Employment Level | ||||||||
| Employed | -1.42 | 0.45 | 9.90 | 1.00 | * 0.00 | 0.24 | 0.10-0.59 | |
| Not Employed ® | - | - | - | 0.00 | - | - | ||
| Distance Covered | ||||||||
| Distance 0-50km | -1.39 | 0.54 | 6.68 | 1 | * 0.01 | 0.25 | 0.10-0.72 | |
| Distance > 51km ® | - | - | - | 0 | - | - | ||
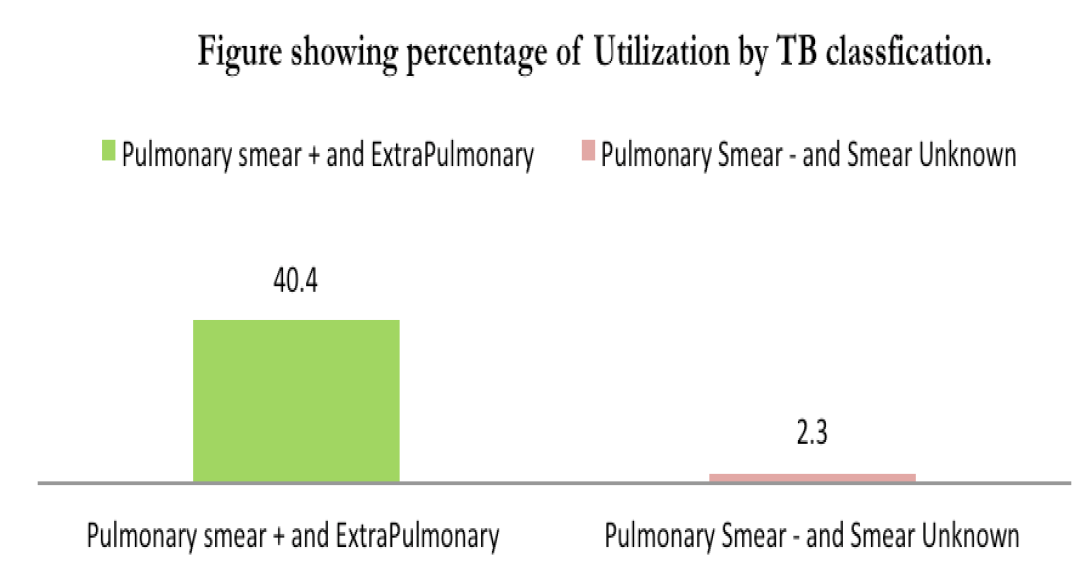
Figure 3: Showing the Utilization Rate for TB Patients by Classification of TB
Married patients in Table 3 above show a higher utilisation rate of Manyatta than non-married (41.1 % for married and 37.5% of nonmarried patients) with multivariate OR of married TB patient category (Figure 4) being at 0.17 (95% CI 0.06 - 0.47). The married TB patients were 1.17 times more likely to use Manyatta than non-married and showed a statistical significance between the two groups.
TB patient religious status usage rate for Christian patients (27.6%) was lower than that of non-Christian patients (43.2%) with an OR of non-Christian being 1.99(95% CI 1.56 - 2.54). The OR did not contain 1.0 a 95% confidence interval for the OR and, therefore, the association was significant. Turkana ethnic group utilization was lower than non-Turkana (38% for Turkana and 40% for Non-Turkana).
Non-educated TB patients had a lower utilization rate than educated patients (32.6% for non-educated and 58.4% for educated TB patients). Educated TB patients utilised Manyatta 2.9 times more than non-educated. The OR for the educated category was at 2.90(95% CI 2.23 - 3.78) that showed a statistical significance.
Patients with pulmonary smear -positive and extra-pulmonary TB had higher utilization rates (40.4 %) than those of pulmonary smear-negative and smear unknown (2.3%). This high percentage of pulmonary smear-positive patient utilisation corresponded to the admission criteria for Manyatta admission. The OR for Pulmonary smear + and the extra-pulmonary category was at 28.51(95% CI 6.98- 116.38) that was also significant statistically. TB patients admitted with relapse and failure had a higher utilization rate than new patients (43.6% for relapse and failure and 35.7% of new TB patients).
The rate of use of TB patients with relapse and failed treatment was more than new admissions (43.6% for relapse and failure and 35.7% of new patients). The OR for new entry category was at 0.05 (95% CI 0.01-0.37). Therefore, this less < 1 OR for this category indicated a negative association between type of patient variable and utilization at the 5% significance level.
The Multivariate logistics regression (Table 4) showed that patient gender, distance to Manyatta, marital status and education level to be predictors of TB Manyatta centre utilization. Gender OR was at 3.14 (95% CI 0.05-0.72); Marital status OR was at 0.17(95% CI 0.06 -0.47); distance OR was at 0.25 (95% CI 010-0.72); Education level being at 0.35 (95% CI 1.98-4.97). They all showed a statistical significance because they did not contain a 95% confidence interval for the OR 1.0. Therefore, they were statistically significant. The results of these variables further indicated a statistical significant difference in the two groups with their p-values being less than p< 0.05 (Age p = 0.01, Marital status p <0.005, Education level p = 0.04.
The overall statistics for the above Multivariate logistic regression model for the educated patients, the distance of 0-50km, male gender, employed TB patients and married patients did not contain a 95% confidence interval for the OR 1.0, thus were statistically significant.
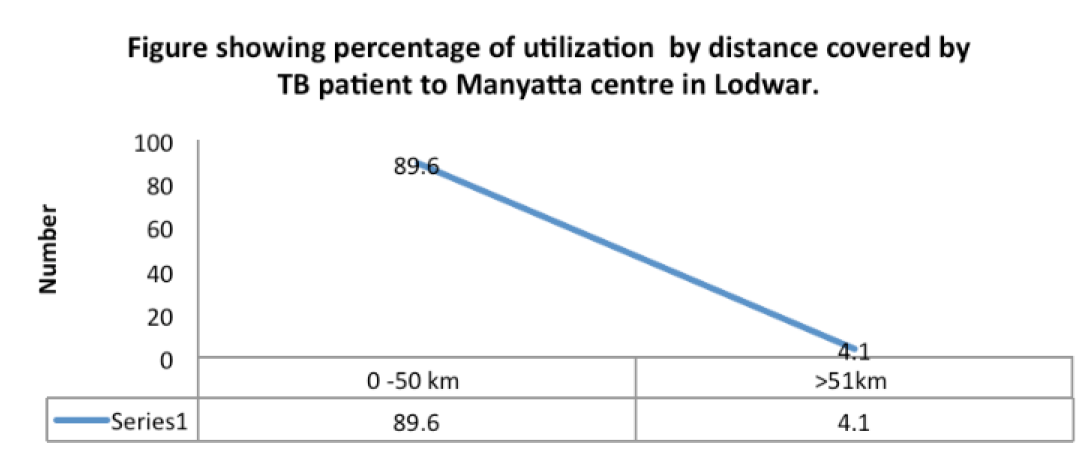
Figure 4: Showing Utilisation Rate by Distance Covered by TB Patient to Manyatta Centre
Figure 5: Showing the Percentage of Utilization by Employment Status of TB Patient
Health Care System Related Factors
This health care system related factors included distance to Manyatta, Healthcare provider’s numbers, and availability of treatment and Manyatta structures.
Table 3 above showed a higher utilization rates (63%) among the TB patients coming from nearer places as superior to those from >50km. The univariate Odd ratio (OR) of distance was for the patient coming from near places was at 8.42(95% CI 6.55 – 10.82) showing patients coming from near places were 8.42 times likely to use Manyatta. There was an existence of statistical significance (It did not contain a 95% confidence interval for the OR 1.0) (Figure 5).
TB patients were having the indication of accessibility to TB treatment in the Manyatta as a factor leading to use had higher utilisation rate (38.9%) than those on no available treatment (3.1%). The OR for TB patients indicating the presence of availability of treatment was 19.73(95% CI 2.68 - 144.95) showing statistical significance.
Lodwar county TB reports indicated that only two health staff works in TB chest clinic for all TB patients and one in the TB Manyatta with Manyatta centre having ten cemented modern houses and with no structures adapted to traditional nomadic structures.
Social, Economic Factors
The social –economic factors described include TB patient employment status and family support.
Figure 6 indicates a higher percentage of utilization of Manyatta by employed patients (58%). Multivariate OR for employment (Table 4) was at 0.24(95% CI 0.10 – 0.59) that showed employment reduced the likelihood of attendance while univariate OR (Figure 3) was at 1.17(95% CI 1.27 - 2.29) indicating a statistical significance. This was opposite, but, in essence, confounding caused the univariate results.
Odd ratios for patients that received supported (Figure 3) were at (OR) of 4.46(95% CI 1.99 - 11.10) that showed a positive association between support and utilisation and a statistical significance. Meanwhile, the meantime on treatment for TB patients who utilized TB Manyatta centre were two month, and those who did not utilize TB Manyatta were an average of four months on a regime of the 6-month regime of treatment. The mean number of referred patients during the period of the 5 years was 105 for those who utilized Manyatta, meaning 99, 8% (525/526 TB patients) of all admissions to the Manyatta centre were referred after initial period of treatment.
The Overall Summary of Results
Only one health staff worked in Manyatta centre, and health personnel never documented the side effects of drugs and were considered absent. Male TB patients utilized more Manyatta than female while TB patients of older age, coming from nearer places, educated, having pulmonary smear-positive and extra-pulmonary, employed and family support used more TB Manyatta centre than rest of the TB patients in their respective category. The variables of gender of patient, distance to Manyatta, employment status, family support, education level, availability of Treatment, classification of TB, type of TB and patient marital status from univariate OR calculations showed a positive association between them and the utilization outcome because of their lower bound confidence interval was greater than 1, meaning they were more likely to use TB Manyatta and they did not contain a 95% confidence interval for the odd ratio (OR) 1.0; therefore they were statistically significant.
WHO [1] argues that Tuberculosis is responsible for about 26% of all the avoidable adult death in many developing countries and this deadliest infectious disease has remained an enormous public health threat despite many efforts and strategies to tackle it. In Kenya, it is estimated that about 200 TB patients die daily [32] and trend has been getting worse in presence of undetected and untreated TB among the mobile, nomadic pastoralists population [8]. TB has been, therefore, maintained among the three top communicable diseases targeted in the millennium development goals (MDGs) according to WHO [2].
The study results provided the response to the research question on what led to the low utilization of TB Manyatta centre by the Turkana nomadic TB patients in Turkana County. These factors were identified, described and analysed, the findings further provided an opportunity to study these factors associated with low utilization of TB Manyatta, and thus the study aim and objectives were met. The flow and the structure of Andersen and Newman Framework of Health Services Utilization (discussed above) were systematically applied when the data results were discussed.
Social Demographic and Clinical Characteristics
Male TB patients utilized TB Manyatta more than the female patient (41.1% for male and 33.5% for female). Multivariate analysis indicates gender OR being 3.14 (95% CI 1.98-4.97) which was statistically significant. Female patients are then considered a risky group to TB Manyatta utilization in Turkana culture because they have to borrow permission. Though many cultural differences exist across many African communities, a cross-sectional study results on use of health care services by Karima et al. [59] indicated that women must acquire permission from their husbands in order to attend any medical services. Women do bear high burden of stigmatization according to Chani [60] and descriptive studies in Nepal by Mathema, et al. [61] and Yamasaki-Nakagawa, et al. [62] and in Bangladesh by Ahsan et al. [63] indicated that fear of social isolation and stigmatization from community among females is a key factor contributing to delay to seek TB treatment. However, this is contrary to a descriptive study from South Africa that mentioned that most of the TB patients who don’t follow any TB treatment intervention are mainly men because they are involved in work [64] and a descriptive study in Peru discusses that men are more proactively employed than women [60].
TB patient marital status according to Mishra et al. [65] has an enormous influence on the uptake of any TB services. Married TB patients utilized more Manyatta than those not married (41.2% for married and 36.5% for non-married). Multivariate OR for marital status was at 0.17 (95% CI 0.06 -0.47) showing the existence of statistical significance. A survey conducted in the study setting by Ndirangu [33] discussed that Turkana culture practices prohibits unmarried women to be far from their families and that being married is more associated to being responsible and trusted than being unmarried.
Lodwar District health staffs did not document drugs side effects on data collection tools but instead mentioned briefly in the TB patient file. This was attributed to negligence. Therefore, no information on TB drug side effects was collected and analysed. However, Similar quantitative studies by Chani [60], Janakan and Seneviratne [66] and Okanurak et al. [67] have all found out that TB drugs side effects play a fundamental role in ensuring that TB patients continue to seek treatment or not, hence, can affect the utilization of Manyatta. Tessema et al. [68] have further advised on proper documentation of all side effects of drugs and manage them wisely by informing the TB patients to anticipate them.
Health care System Related Factors
The utilisation rate of patients coming from nearer places (0-50km) in the figure was higher than those coming from far areas of >50 km. An Odd ratio of distance was 8.42 (95% CI 6.55 -10.83) showing the existence of statistical significance. This finding corresponds to similar descriptive studies by Date et al. [69], Bam et al. [20] and Omar [70] suggested that population close to TB services do utilise the service in more than those living in far areas. It therefore, indicated that the further the distance, the less utilization of TB Manyatta centre. Hence, far patients according to Chatterjee et al. Hasker et al. [71] and Duba et al. [72] will prefer accessible traditional healer’s treatment than travel far. It is for this reason of living far from treatment centres that Liefooghe et al. [73], Maalim [74], and Gele et al. [75] have suggested for development of a shorter TB drugs regime that could fit the nomadic lifestyle and establishment TB care centres in the strategic villages and predictable routes during different nomad’s migratory seasons where these nomads pass. In this study, the author can argue that distance had contributed to the low uptake of TB Manyatta services.
Lodwar county TB reports further indicate that Manyatta centre have ten cemented modern houses with no fence and structures not adapted to traditional nomadic structures. A descriptive study of TB village (similar to Manyatta) in Ethiopia by Zachariah et al. [31] indicated that adapting the living conditions of TB nomad’s patients to their traditional lifestyles motivated the TB patients to stay in during their entire period of treatment.
The workload is high to this few staffs found to be working in the TB program and compromised the contact needed to the TB patients and health care providers [8]. Lack of connections does jeopardize the motivation and trust required by TB patients to continue treatment [2]. Similar cross-sectional studies by Jaiswal et al [76] in India and Pozsik [77] and Volmik [78] demonstrated that lack of attention by health worker to TB patients increases chances of low uptake of TB services because real relationship influence better uptake TB services [1].
Social –Economic Factors
Benatar and Upshur [79] have argued that TB hinders economies especially when the head of the family is affected, and cash is lost. The univariate analysis and multivariate analysis association were opposite for employment in the two types of analysis. Multivariate OR being at 0.24(95% CI 0.10 – 0.59) and that of univariate analysis OR at 1.70(95% 1.27-2.29). Univariately, employment leads to more attendance, whereas in multivariate it reduces the likelihood of attendance. Meaning unemployed are more likely to use Manyatta, and that the univariate results were caused by confounding. The influence was probably because far more men than women (above) utilised the service, and there is more employment among men. A case-controlled approach study by Hasker et al. [71] indicated that employment statuses of the TB patients have the tremendous effect on the way TB programs are taken. Contrast to the findings, Hasker et al. [71] argues that being employed is more associated with better social, economic status that enables one to afford health care fees, and cost of transport thus raises the chance of treatment compliance. A cross-sectional study by O’Boyle et al. further identified that providing the travelling cost to a treatment centre contributes maximally to treatment compliance but the author argues that this can be unpractical in poor settings and cannot offer a long-term solution.
According to Ndirangu [33], the culture of Turkana community encourages family unity in illness, and this is clearly demonstrated in the findings where TB patients with family support utilized more Manyatta than those non-supported (39% for being supported and 12% for not supported). A quantitative study in Colombia showed that unsupported TB patients were likely not able to comply with any TB care option [80] while those who receive support from their families do adhere to any TB program services according to Dembele et al. [81].
Enabling Factors and Predisposing Factors
Cohen [19] has argued that nomadic population do lag behind in education, and it affects their acceptability to any health services. Educated patients used more Manyatta than non-educated (58.4% for educated and 32.6% for non-educated), and OR was at 2.9007(95% CI 2.2248 - 3.7818) that showed a statistical significance. A quantitative study in Tanzania found out that the inadequate education of TB patients does influence the acceptance of TB services [82]. Limited knowledge on TB, on the other hand, encourages TB patients to seek traditional alternative medicine according to Ndirangu [33]. Descriptive studies by Date et al. [69] and Mishra et al. [65] have all suggested that TB patient level education have a tremendous contribution to any TB treatment compliance and a cross-sectional study in Thailand by Okanurak, Kitayaporn and Akarasewi aimed at determining the predicting factors for successful TB treatment further found out that, the higher the TB patient education levels, the better the compliance to TB treatment and eventual treatment success.
This study has therefore identified female TB patient to be a risky group to the utilization of TB Manyatta services; marital status, family support, employment status of patient, TB patient knowledge on the disease and education and distance to Manyatta centre from study discussion of findings played a key role in ensuring utilization of Manyatta and were statistically significant, for the reason that, less of any of these factors resulted in less use of Manyatta. Lack of adapted Manyatta structures to nomadic lifestyle and number of staffs in Manyatta on another hand negatively affected the acceptability of Manyatta.
Discussion of the Research Process, Limitation and Lessons Learned
The study identified and investigated on the problem of the low utilization of TB Manyatta centre by the nomadic population, reviewed and evaluated well the literature available on TB Manyatta concept. The study considered the ethical issues by obtaining approval and study written consent while ensuring study Positionality is put into consideration. Answerable study question through investigation was clear and different variables were identified, described and analysed.
As large sample sizes increases the chances of precision according to Ghyoot [83], the author applied this and utilized the De Vos et al. [47] recommendation on a sample size that produced enough samples to investigate the research question. Biases were minimised, and a sound research methodology was applied with secondary data being examined and discussed. It was then accurately interpreted to answer the study question with the final feedbacks of the study to be handed to the hospital authority for action.
However, despite the critical appraisal of research process steps discussed and the merits and the choice of this study methodology, a few other restraints need to be taken into account; the study utilized secondary data that the researcher didn't know how it was inserted in the data collection instruments and whether there was a manipulated or not. Hence, the researcher considers that the study question could have been probably responded well by use of a questionnaire.
Consequently, for this study being the first research in the setting of the researcher knowledge and literature review, the actual concrete facts about TB care and practices in the Turkana nomadic settings is therefore limited, nonetheless, with the researcher positional and coming from study context, it was then easy to carry out the study.
Although the TB registers and reports were used mainly as sample framework to collect data with only one element that was completely not recorded (side effects of drugs) and found in the individual TB patients file, for the possible reasons mentioned above, the author had no other option but to collect the data as it was. The secondary data collection method had difficulty in understanding how the data components were initially gathered and inserted in the TB register and TB reports. However, significant weight lies on the merits of these secondary data collection choice because they are fast, cheap and easy to get a larger sample that increases the chances of better precision [37].
The missing data found only in the patient file could put a question mark on the validity of the sample frame utilized but the validity of findings was more concerned with the generalization of the study findings and research design used. The choice of sampling that was adequate for the study ensured that the validity and any threats in the study was reduced by utilization and selection of cross-sectional study stated above as the measure was done at one point in time only thus reducing the possibility of attrition by research participants that could have otherwise compromised the validity [37]. All required elements from study are included and a good 20% sample size from the sample frame being utilized, getting data from validated government tools and avoiding manipulations thus improving external validity and reducing the biases according to Joubert et al. [84].
Some of the probable co-founders associated with low uptake of TB Manyatta that could have affected the validity of the finding if they could not have been well identified and analysed were employment status and gender and these variables were measured and examined to check if there was any independent relation with low uptake of TB Manyatta.
With no other completed specific studies and information about Lodwar Manyatta centre, to complement the information needed, certain literature from populations with alike characterizes were utilized and individual errors have to be accepted and as shown above in the literature review, the only available study in the Turkana setting was that of Ndirangu [33] that did not touch Manyatta centre. This study was restricted to Turkana nomadic population setting; therefore, the results cannot be generalized beyond the Turkana context to other Kenyan nomadic population.
The implementation of TB Manyatta strategy for the Turkana mobile population has been thought to give a solution, but Manyatta itself has never been explored in the setting, thus low utilization by nomadic population. The study objective, therefore, was to undertake a literature review on nomadic pastoralists TB care to establish the contributing factors to the low uptake of TB Manyatta services using secondary data that was collected and anal ysed.
Public health sees community as a patient [34] and needs treatment, within this mobile community in the study where access to TB care across the volatile borders has been an enormous struggle amid weak peripheral health care, then, TB remains a challenging public health problem to tackle within this migratory population. Therefore proposed strategies like Manyatta that motivate, ensure prompt accessibility and compliance with TB treatments need to be encouraged and supported at all levels.
With the strength and the weakness seen in this research findings (some factors to include age with no association to utilization), this study opens a window for further investigations and a needs that govern the development of specific TB guidelines and policies for mobile populations in risky settings and encourage further improvement of TB Manyatta idea within the Lodwar county and Kenyan National Tuberculosis strategic planning as a whole.
TB Manyatta centre bridges the gap where access to TB care is a struggle [31] and within the mobile population, this centre ensures that TB treatment is accessible and adhered to with greater compliance. Thus, helps in achievement of better overall TB outcomes. Therefore, Manyatta usage within the mobile population needs to be encouraged; ensuring that the structures are well adapted to the nomadic lifestyle, services are promoted, and nomadic population educated on TB and encouraged to participate on health issues proactively. The participation empowers them to take care of own health and improve confidence to utilize the TB Manyatta services.
In this study, findings indicated that marital status, gender, and education level of patient, distance to Manyatta and structure of Manyatta were statistically significant and associated with uptake of low utilisation of Manyatta and, therefore, they formed the most important factors. Age, employment status and ethnic group were less significant statistically while classification of TB diagnosis, ethnic group, availability of treatment and family support were less important. These important factors answered the study question on what factors determine the low utilization of the TB Manyatta center by the Turkana nomadic TB patients. Study literature review, findings and discussions toiled around understanding Manyatta strategy and its current issues of low utilization, and it is, therefore; worth to say that TB Manyatta strategy and TB care among mobile population as a whole, need to be well developed, improved and explored. The understanding of the Manyatta strategy will not only assist in ameliorating the TB care in complex settings but also identify and challenge the TB care using strategies that attract its compliance.
One of the other issues to be addressed is change of policy in management of TB within nomadic population to include community empowerment in the care of TB, and sharing of ideas and strategies on TB control in population at risk across the border countries where TB nomadic pastoralist’s population migrate. The researcher recommends for the formulation of a policy that govern the management of TB across borders and TB management of the migratory population. This policy can not only act as a perfect catalyst in motivating the nomadic population to remove taboos and cultural practices that hinder TB care accessibility but also ensure the community ownership in managing own health problems.
This study further challenges the Kenyan Ministry of Health to develop TB Manyatta care guidelines and Manyatta services utilization models that are missing, because little from the literature is known about TB Manyatta in Turkana and in general and TB control activities across the borders. Through the TB national program, the researcher further recommends the Kenyan ministry of health to work with other regional TB programs to tackle TB disease across the borders. The exchange of ideas and collaboration will not only assist in borrowing the technical know-how on developing new mobile population TB care policies but also help in improving the existing policies on TB management of the risk society.
Recommendation
Finding indicated that women were less likely to utilise Manyatta then men. The researcher recommend the Kenyan ministry of health to roll out health generic strategies within nomadic pastoralists population that promote health among the female population, work against cultures that prohibits accessibility of TB services by non-married women and ensure that the services are more woman-friendly. This will then promote health among women and encourage utilisation of TB Manyatta services.
As the drug side effects data missed, this study recommends for an improvement of data collection process in Lodwar TB program by ensuring that there is correct, systematic and accurate documentation of patient data, both clinical and demographic information. The data collection process the researcher argues will, therefore; require training, improvement of medical curriculums in TB care and importance of data. The researcher further recommends the hospital management team to strengthen supervision of the data management in TB Manyatta.
Findings showed that TB patients living far from Manyatta used less Manyatta unlike those from near places and this study recommends for decentralisation of Manyatta, to be constructed nearer to the nomadic dwelling places and or along the predictable routes where nomadic pastoralists pass during different seasons in order to capture more mobile, nomadic TB patients to utilise and reduce infection transmission.
Lack of nomadic pastoralist lifestyle adapted TB Manyatta structures in Lodwar have been found and discussed to shy away TB pastoralist patients because they are all built modern houses. The researcher recommends for the renovation and getting the structures look more adapted to traditional nomadic structures. This pastoralist lifestyle changed structures will attract usage.
Based on the research findings, shortages of staff issue needs to be addressed at all levels, both in the hospital and the county level. The researcher recommends, therefore, the need for hospital management team to balance the number of health workers in other department and sent some to TB Manyatta centre. The Turkana county government, on the other hand, can further employ more health personnel that can be posted to Manyatta. This will not only motivate the staff, improve the quality of TB care in Manyatta but also cultivates a friendlier attitude, trusts and contact atmosphere in Manyatta between health workers and TB patients and consequently motivates in continuity of Manyatta utilization.
TB patients that received family support utilized more Manyatta than those not supported, and this indicated an existence of strong nomadic pastoral community family ties. This study recommends the Kenyan ministry of health to utilise this advantage to roll out and decentralise programs that are designed to strengthen and encourage community TB advocacy within the nomadic population. These programs will aim to promote the utilisation of TB Manyatta that supplement the WHO recommended DOT strategy, thus prompt adherence to treatment.
Educated TB patients utilized more Manyatta than not educated and patient level of education has been found in the study to influence uptake of Manyatta, therefore, this study advocates for intensification of nomadic pastoralists TB patient health education on treatment literacy that would assist not educated nomads to understand more about the disease and prompt uptake of the TB Manyatta services.
At the end of the study, full research copy will be handed over to Lodwar district hospital management team, and Turkana County and hopefully the results and the recommendations of this study will be implemented and followed carefully.
Recommendations for Further Studies
Having the demerits of utilizing secondary data, a further use of questionnaire- interview study is needed to check the reasons for low uptake of the TB Manyatta. Furthermore, in order to understand the Turkana nomadic pastoralist’s behaviour, practice regarding TB and social-cultural beliefs for low uptake of TB Manyatta, a qualitative study on the above topic can be repeated in order to provide maximum in depth information.
World Health Organization. Tuberculosis fact sheet no. 104. November 2010.
World Health Organization. Global tuberculosis control 2011. 2012.
World Health Organization. Stop TB partnership: Tuberculosis fact 2009 update. 2009.
Volmink, J. et al. Directly observed therapy for treating tuberculosis. Cochrane Database of Systematic Reviews, no. 4, 2007, CD003343.
Zinsstag, J. et al. Health of nomadic pastoralists: New approaches towards equity effectiveness. Tropical Medicine and International Health, vol. 11, no. 5, May 2006, pp. 565–568.
Kochi, A. The global tuberculosis situation and the new control strategy of the World Health Organization. Tubercle, vol. 71, 1991, pp. 1–6.
AMREF. Calls for greater synergy and investment to reach, treat and cure every TB case. 2015.
World Health Organization. Global strategy and targets for tuberculosis prevention, care and control after 2015. 2014.
Tanner, M. Strengthening district health systems. Bulletin of the World Health Organization, 2005.
Muga, R. et al. Overview of the health system in Kenya. 2004.
Wangui, P. et al. Risk factors in the transmission of tuberculosis in Nairobi: A descriptive epidemiology study. Advances in Microbiology, 2013.
Gillespie, S. et al. Is poverty or wealth driving HIV transmission? AIDS, vol. 21, suppl. 7, 2007, pp. S5–S16.
World Health Organization. World health statistics 2010. 2010.
Kenya National Bureau of Statistics. Kenya census 2009. 2009.
Mgomella, G.S. et al. HIV mortality in urban slums of Nairobi, Kenya 2003–2010: A period effect analysis. BMC Public Health, 2013.
USAID. Horn of Africa pastoral interventions. 2005.
Cambanis, A. et al. Rural poverty and delayed presentation to tuberculosis services in Ethiopia. Tropical Medicine and International Health, vol. 10, no. 4, 2005, pp. 330–335.
Gele, A.A. et al. Barriers to tuberculosis care: A qualitative study among Somali pastoralists in Ethiopia. BMC Research Notes, vol. 3, 2010, pp. 86.
Cohen, D. Providing nomadic people with health care. British Medical Journal, vol. 331, 2005, pp. 720.
Bam, T.S. et al. Factors responsible for non-compliance among TB patients in Kailali district, Nepal. Journal of Nepal Health Research Council, vol. 3, no. 2, 2005, pp. 51–57.
Kenya National Bureau of Statistics et al. Kenya demographic and health survey 2008–09. 2009.
Hehenkamp, A. et al. Tuberculosis treatment in complex emergencies: South Sudan. The Lancet, vol. 362, suppl., 2003, pp. S30–S31.
Weyer, K. Discovery, innovation and new frontiers in tuberculosis diagnostics: Reflections and expectations. Journal of Infectious Diseases, 2015.
Kenyan health systems hierarchy. Health care utilization. 2014.
Opiyo, P. et al. Perceptions and attitudes of health professionals in Kenya on national health care resource allocation mechanisms: A structural equation modelling. PLoS ONE, 2015.
Division of Health Management Information Systems. Kenya annual health sector statistics report. Ministry of Public Health and Sanitation, 2008.
Abuja declaration. Abuja declaration on HIV/AIDS, tuberculosis and other related infectious diseases. 2001.
Family Planning Conference. Abuja conference declaration. 2009.
Gothi, D. Resistant TB: Newer drugs and community approach. Recent Patents on Anti-Infective Drug Discovery, 2011.
Ministry of Public Health and Sanitation. National health sector strategic plan II (2008–2012). 2012.
Zachariah, R. et al. The experience of implementing a TB village for a pastoralist population in Cherrati, Ethiopia. Médecins Sans Frontières, 2011.
Kenya health information system. Turkana county TB data. 2013.
Ndirangu, W.M. Determinants of inequalities in timeliness of tuberculosis care between nomadic and settled people in Turkana district, Kenya. 2009.
Naidoo, J. et al. Assessing health needs. Foundations for Health Promotion, 2009.
Wright, J. Assessing health needs. Oxford Handbook of Public Health Practice, 2001.
Hmama, Z. Management of drug resistant TB. Tuberculosis: Current Issues in Diagnosis and Management, 2013.
Burns, N. et al. The practice of nursing research: Conduct, critique, and utilization. 5th ed., Elsevier Saunders, 2005.
Médecins Sans Frontières Holland. TB manyatta. 1995.
Jackson, M. et al. A survey of health professions students for knowledge, attitudes, and confidence about tuberculosis. BMC Public Health, vol. 7, 2007.
Centers for Disease Control and Prevention. Tuberculosis behavioral and social science research forum: Proceedings. 2005.
World Health Organization. Anti-TB medication side effects contribute major factors for poor adherence to TB treatment. Bulletin of the World Health Organization, vol. 86, no. 3, 2008.
Bruce, N. et al. Quantitative research methods in public health: A practical, interactive guide. J. Wiley and Sons, 2007.
Bryman, A. Social research methods. Oxford University Press, 2001.
Adamu, H.S. Utilization of maternal health care services in Nigeria: An analysis of regional differences in the patterns and determinants of maternal health care use. University of Liverpool, 2011.
Green, J. et al. Qualitative methods for health research. Sage, 2009.
Bland, M. An introduction to medical statistics. 3rd ed., Oxford University Press, 2001.
De Vos, A.S. et al. Research at grass roots. 3rd ed., Van Schaik, 2007.
Black, K. Business statistics for contemporary decision-making. 4th ed., Wiley-India, 2004.
Babbie, E.R. The practice of social research. 10th ed., Thomson/Wadsworth, 2004.
Stommel, M. et al. Clinical research: Concepts and principles for advanced practice nurses. Lippincott Williams and Wilkins, 2004.
Makhanu, E. Principals’ literacy in ICT: Towards improving secondary school performance in Kenya. University of South Africa, 2010.
Andersen, R.M. Revisiting the behavioural model and access to medical care: Does it matter? Journal of Health and Social Behavior, vol. 36, 1995, pp. 1–10.
Altman, D.G. Practical statistics for medical research. Chapman and Hall, 1991.
Porta, M. A dictionary of epidemiology. 5th ed., Oxford University Press, 2008.
Peach, C. Social geography: New religion and ethnoburbs. Contrasts with cultural geography. Progress in Human Geography, vol. 26, no. 2, 2002, pp. 252–260.
Hopkins, P.E. Positionalities and knowledge: Negotiating ethics in practice. 2007.
Homfray, M. Standpoint, objectivity, and social construction: Reflections from the study of gay and lesbian communities. Sociological Research Online, vol. 13, no. 1, 2008.
Sultana, F. Reflexivity, positionality and participatory ethics: Negotiating fieldwork dilemmas in international research. ACME, vol. 6, no. 3, 2007, pp. 374–385.
Karima, F. et al. Female–male differences at various clinical steps of TB treatment. International Journal of Tuberculosis and Lung Disease, vol. 12, no. 11, 2008, pp. 1336–1339.
Chani, K. Factors affecting compliance to tuberculosis treatment in Andara Kavango region, Namibia. University of South Africa, 2010.
Mathema, B. et al. Tuberculosis treatment in Nepal: A rapid assessment of government centers using different types of patient supervision. International Journal of Tuberculosis and Lung Disease, vol. 5, no. 10, 2001, pp. 912–919.
Yamasaki-Nakagawa, M. et al. Gender difference in delays to diagnosis and health care seeking behavior in a rural area of Nepal. International Journal of Tuberculosis and Lung Disease, vol. 5, no. 4, 2001, pp. 1072–1074.
Ahsan, G. et al. Gender difference in treatment seeking behaviors of tuberculosis cases in rural communities of Bangladesh. Southeast Asian Journal of Tropical Medicine and Public Health, vol. 35, no. 1, 2004, pp. 126–135.
Connolly, C. et al. Who fails to complete tuberculosis treatment? Risk factors for treatment interruption in a community-based directly observed therapy programme in rural South Africa. International Journal of Tuberculosis and Lung Disease, vol. 3, no. 12, 1999, pp. 1081–1087.
Mishra, P. et al. Socio-economic status and adherence to tuberculosis treatment: A case control study in a district in Nepal. International Journal for Tuberculosis and Lung Disease, vol. 9, 2005, pp. 1134–1139.
Janakan, N. et al. Factors contributing to medication noncompliance of newly diagnosed smear positive pulmonary tuberculosis patients in the district of Colombo, Sri Lanka. Asia-Pacific Journal of Public Health, vol. 20, no. 3, 2008, pp. 214–223.
Okanurak, K. et al. Factors contributing to treatment success among tuberculosis patients: A prospective cohort study in Bangkok. International Journal for Tuberculosis and Lung Disease, vol. 12, no. 10, 2008, pp. 1160–1165.
Tessema, B. et al. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia: A five-year retrospective study. BMC Public Health, vol. 9, 2009, pp. 1–8.
Date, J. et al. Gender and literacy: Factors related to diagnostic delay and unsuccessful treatment of tuberculosis in the mountainous area of Yemen. International Journal for Tuberculosis and Lung Disease, vol. 9, 2005, pp. 680–685.
Omar, M.A. Health cares for nomads too, please. World Health Forum, vol. 13, no. 4, 1992, pp. 307–310.
Hasker, E. et al. Default from tuberculosis treatment in Tashkent, Uzbekistan: Who are these defaulters and why do they default? BMC Infectious Diseases, vol. 8, 2008, pp. 97.
Duba, H.H. et al. Pastoralist health care in Kenya. International Journal of Integrated Care, vol. 1, 2001, e13.
Liefooghe, R. et al. Perception and social consequences of tuberculosis: A focus group study of tuberculosis patients in Sialkot, Pakistan. Social Science and Medicine, vol. 41, 1995, pp. 1685–1692.
Maalim, A. Participatory rural appraisal techniques in disenfranchised communities: A Kenyan case study. International Nursing Review, vol. 53, no. 3, 2006, pp. 178–188.
Gele, A.A. et al. Armed conflicts have an impact on the spread of tuberculosis: The case of the Somali Regional State of Ethiopia. Conflict and Health, vol. 4, 2010, pp. 1.
Jaiswal, A. et al. Adherence to tuberculosis treatment: Lessons from the urban setting of Delhi, India. Tropical Medicine and International Health, vol. 8, no. 7, 2003, pp. 625–633.
Pozsik, C.J. Human behavior as a factor in the treatment of tuberculosis. Improving Tuberculosis Treatment and Control: An Agenda for Behavior, Social and Health Services Research, 1995.
Volmink, J. et al. Directly observed therapy and treatment adherence. The Lancet, vol. 356, no. 9234, 2000, pp. 1032.
Benatar, S.R. et al. Tuberculosis and poverty: What could (and should) be done? International Journal of Tuberculosis and Lung Disease, vol. 14, no. 10, 2010, pp. 1215–1221.
Mateus-Solarte, J.C. et al. Factors predictive of adherence to tuberculosis treatment, Valle del Cauca, Colombia. International Journal for Tuberculosis and Lung Disease, vol. 12, no. 5, 2008, pp. 520–526.
Dembele, M. et al. An exploration of the concept of directly observed treatment (DOT) for tuberculosis patients: From a uniform to a customized approach. International Journal of Tuberculosis and Lung Disease, vol. 7, 2003, pp. 103–109.
Mfinanga, S.G. et al. Patient knowledge, practices and challenges to health care system in early diagnosis of mycobacterial adenitis. East African Medical Journal, vol. 82, no. 4, 2005, pp. 173–180.
Ghyoot, V.G. Property marketing III: Study guide 3. National Property Education Committee, 1994.
Joubert, G. et al. Epidemiology: A research manual for South Africa. 2nd ed., Oxford University Press, 2008.
