
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-953X
ISSN (Online) : 2788-9548
This Original research provides a comprehensive overview of transversus abdominis plane (TAP) block, a regional anesthesia technique used for postoperative pain management in abdominal surgeries. The abstract discusses the efficacy of TAP block in reducing postoperative pain and the need for analgesics. It also highlights the potential challenges and considerations when performing TAP block in specific patient populations, such as pregnant patients and those undergoing laparoscopic bariatric surgery. The importance of proper training and proficiency in ultrasound-guided TAP block is emphasized, as it improves procedural success and reduces complications. Ultrasound guidance is shown to enhance the accuracy and safety of TAP block by providing real-time visualization of needle placement. Overall, this abstract emphasizes the need for further research and training in TAP block to optimize its use in clinical practice.
The TAP block is a regional anesthesia technique used for postoperative analgesia in abdominal surgeries. It involves injecting local anesthetic in the neurofascial plane between the internal oblique and transversus abdominis muscles [1,2]. This block targets the abdominal wall nerves, specifically the T7-L1 spinal nerves, to reduce pain [3]. TAP block has been compared to other analgesic techniques and has shown to provide better early postoperative analgesia with almost no complications [4]. It has been found to be equally effective in managing pain after abdominal surgery in pediatric patients [5]. TAP block has also been used successfully in elderly patients undergoing lumboperitoneal shunt surgery, providing quick relief from postoperative abdominal pain. Overall, TAP block is a valuable technique for postoperative pain control in lower abdominal surgeries, offering analgesic benefits and reducing the need for opioids. Local anesthetic systemic toxicity (LAST) is a potential complication of regional blocks, occurring when too high a dose of local anesthetic is accidentally injected intravascularly. It can lead to neurological and cardiovascular manifestations, and early recognition and intervention are crucial for patient management [6]. Patients at extremes of age or with organ dysfunction are at higher risk for LAST [7]. Techniques such as using ultrasound guidance, aspirating prior to injection, and utilizing the minimal local anesthetic dose needed can help reduce the risk of LAST [8]. Intravenous lipid emulsion 20% is the mainstay of treatment for LAST [9]. Complications of local anesthetic systemic toxicity include local anesthetic systemic toxicity, which can occur with peripheral blocks of the hypogastric plexus under fluoroscopy [10]. Local anesthetic systemic toxicity can give rise to neurological symptoms that may or may not be associated with hemodynamic instability. Accidental puncture or trauma to abdominal wall nerves during a transversus abdominis plane (TAP) block can potentially cause temporary or permanent numbness or pain [11].
The Literature Review
This literature review aims to explore and analyze the disadvantages associated with the TAP block procedure and its impact on patient outcomes. By examining existing research studies and clinical trials, we seek to provide a comprehensive overview of the limitations, complications, and challenges related to the TAP block technique.
Potential Complications
One potential disadvantage of the transversus abdominis plane (TAP) block is the risk of nerve injury. Accidental puncture or trauma to abdominal wall nerves during the TAP block procedure can lead to temporary or permanent numbness and pain in the affected areas. Proper ultrasound guidance during needle and catheter placement can help minimize this risk [12,13]. However, nerve injury remains a potential complication of TAP blocks that patients should be aware of. Careful identification of abdominal wall anatomy and avoiding direct nerve contact as much as possible can help reduce the risk of this disadvantageous outcome [14]. Other rare complication is inadvertent puncture of underlying organs, such as the liver or intestines, during needle insertion for the block [15]. This can lead to issues like bleeding, infection, or organ injury. Another potential complication is catheter dislodgement when using a catheter infusion technique for continuous pain relief [16]. If the catheter becomes displaced, it can interrupt the intended pain relief from the local anesthetic infusion. To minimize these risks, practitioners should take precautions such as proper patient selection, use of ultrasound guidance, careful needle and catheter placement, and secure fixation [17]. It is important for patients to be aware of these potential complications to provide informed consent for the procedure [18].
Limitations in Analgesic Effect
The TAP block has a shorter duration of analgesia compared to epidural analgesia. Studies have shown that the analgesic effect of a TAP block lasts for an average of 6-12 hours, while epidural analgesia can provide pain relief for 24 hours or longer [19,20]. The inconsistent spread of local anesthetic during a TAP block is a limitation due to anatomical variability, making it difficult to reliably block all the nerves innervating the anterior abdominal wall. As a result, some areas may still experience postoperative pain despite the block [21]. The TAP block primarily targets the nerves of the anterior abdominal wall and may not provide deep visceral analgesia like epidural analgesia. It does not penetrate deeply enough to block nerves supplying the internal organs and posterior abdominal wall [22,23,24].
Patient Factors
The transversus abdominis plane (TAP) block is a regional anesthesia technique that can provide effective pain relief after abdominal surgery. However, in obese patients, needle placement for TAP block can be more difficult due to excessive subcutaneous fat. This can lead to inadequate needle positioning, failed regional analgesia, and possible related risks [25]. TAP block with coagulopathy can increase the risk of bleeding with needle insertion, which is a concern for patients on antithrombotic drugs. Bleeding complications after peripheral nerve blocks (PNBs) in patients treated with antithrombotic agents are rare but can result in significant morbidity and may require interventions [26]. The risks of bleeding after PNBs depend on various factors such as block depth, associated comorbidities, anticoagulation status, and technical factors [27]. In the context of image-guided core-needle breast and axillary biopsy (CNB), bleeding is a common complication, and the management of antithrombotic therapy in these patients is still not standardized [28]. A joint guideline from the European Society of Anaesthesiology and Intensive Care and the European Society of Regional Anaesthesia recommends specific time intervals for the administration of antithrombotic drugs before and after nerve blocks to reduce the risk of hematoma formation [29]. The efficacy of TAP block in morbidly obese patients undergoing laparoscopic bariatric surgery is still under discussion, considering the challenges in ultrasound visualization due to excessive subcutaneous fat [30]. In patients on dual antiplatelet therapy or direct-acting oral anticoagulants undergoing high-bleeding risk cardiovascular surgery, bleeding rates range from 18% to 41%, and various potential solutions to mitigate bleeding complications are being explored. TAP block is a method of providing postoperative analgesia after abdominal surgeries, including caesarean section (CS) [31,32]. It has been shown to be effective in reducing postoperative pain and the need for analgesics [33]. However, in pregnant patients, there are concerns about the effects of local anesthetic on the fetus, and the use of TAP block during obstetrical paracervical block anesthesia is contraindicated due to the risk of fetal bradycardia and death [34]. Therefore, it is important to weigh the benefits and risks of TAP block in these patient populations and to consider alternative pain management strategies when necessary [35].
Skill and Training Required
Training programs, workshops, and hands-on practice are essential for clinicians to acquire the necessary skills and knowledge to perform TAP blocks effectively and safely [36]. Clinicians must develop proficiency in using ultrasound equipment, interpreting ultrasound images, and accurately identifying the relevant anatomical structures [37]. Inexperienced users can teach themselves to gain significant procedural skills, but participating in training courses or practicing with experts can enhance the outcomes [38]. Learning to perform TAP blocks with ultrasound guidance has a learning curve, and clinicians need to understand the indications, clinical pearls, and pitfalls of each procedure to avoid potential complications [39]. Residents demonstrated improvement in ultrasound-guided procedural skills and reported increased comfort performing these procedures after training on an agar model [40]. Ultrasound increases the first-attempt success rate for vascular access, and competency on ultrasound-guided peripheral intravenous cannulation can be achieved after following a brief training in a fixed curriculum. In the absence of ultrasound guidance, accurate needle placement during TAP blocks can be challenging, leading to suboptimal pain relief or block failure. Without visualizing the target nerves and adjacent structures, clinicians may struggle to locate the neurovascular plane accurately, resulting in inadvertent needle placement into unintended tissues or structures [41]. Ultrasound-guided nerve blocks provide real-time visualization of needle placement, allowing for accurate drug injection around the nerve or into the nerve in some cases [42].
This technique is considered safer and more accurate than the conventional landmark-based technique, particularly for less experienced clinicians [43]. Ultrasound guidance improves the success rate of nerve blocks by improving block operating efficiency, decreasing placement complications, and reducing patient discomfort [44]. To mitigate the risks associated with performing TAP blocks without ultrasound guidance, alternative techniques such as landmark-based approaches or nerve stimulation can be employed. These techniques rely on anatomical landmarks or nerve stimulation to guide needle placement. However, they are generally considered less reliable and have a higher risk of incomplete or inaccurate blocks [45,46,47]. Ultrasound guidance technique, on the other hand, allows for real-time visualization of needle placement and accurate drug injection around the nerve, resulting in improved success rates and safety [48,49]. Ultrasound-guided nerve blocks provide direct visualization of the target nerve and deposition of local anesthetic, improving block operating efficiency while decreasing placement complications and patient discomfort. Therefore, ultrasound guidance is considered the gold standard for regional anesthesia, particularly for lower extremity blocks. Ultrasound guidance is recommended for performing transversus abdominis plane (TAP) blocks as it reduces the risk of incomplete or inaccurate needle placement, improvingthe effectiveness and safety of the block [50,51]. However, clinicians need to undergo training and gain proficiency in ultrasound imaging and needle guidance to perform TAP blocks accurately [52]. Without ultrasound, there is an increased risk of complications and compromised block efficacy [53]. Clinicians should consider the benefits and limitations of different techniques for TAP blocks and choose the approach that aligns with their skills and resources [54].
Data Collection Samples
A regular random probabilistic sample was used in the records of resting patients out of 120 patients after dividing the total community by 3 = 40 samples were selected to represent the study community in the Hall of Al Shifa General Hospital to study the condition of patients after conducting modern editing TAP block technology, which contributes to exploring the desired results of modern methods of anesthesia.
Statistical Analysis
The statistical analysis in this research involved the use of descriptive statistics to summarize the demographic data and other variables of interest, Frequencies and percentages were calculated to describe the distribution of gender, age, marital status, and the presence of chronic diseases among the participants. In addition, inferential statistics were used to analyze the relationship between certain variables. For example, percentage and frequency tests were conducted to examine the association between bleeding after using the TAP block due to anticoagulant drugs and the presence of chronic diseases (Table 1).
Table 1: Stated Statistical Analysis of Demographic Data and Check List of 40 Samples
Demographic Data | Categories | Freq. | Percentage |
| male | 16 | 40 |
female | 24 | 60 | |
| 19-29 years | 13 | 33 |
29-39 years | 20 | 50 | |
39-49 years | 7 | 17 | |
| single | 10 | 25 |
married | 26 | 65 | |
widow | 1 | 2.5 | |
divorced | 3 | 7.5 | |
| Yes | 11 | 27.5 |
No | 29 | 72.5 | |
| 6 hours | 31 | 77.5 |
12 hours | 8 | 20 | |
24 hours | 1 | 2.5 | |
| Temporary | 23 | 57.5 |
Permanent numbness | 17 | 42.5 | |
| Yes | 4 | 10 |
No | 36 | 90 | |
| Yes | 21 | 52.5 |
No | 19 | 47.5 | |
| Yes | 10 | 25 |
No | 30 | 75 | |
| Yes | 31 | 77.5 |
No | 9 | 22.5 | |
| Yes | 22 | 55 |
No | 18 | 45 |
The results of the study showed that out of the 40 participants, 16 were male (40%) and 24 were female (60%). In terms of age, 13 participants were between 19-29 years old (33%), 20 participants were between 29-39 years old (50%), and 7 participants were between 39-49 years old (17%). Regarding marital status, 10 participants were single (25%), 26 participants were married (65%), 1 participant was a widow (2.5%), and 3 participants were divorced (7.5%) [3]. In terms of chronic diseases, 11 participants reported having chronic diseases (27.5%), while 29 participants did not have any chronic diseases (72.5%). When asked about the duration of analgesia after the TAP block, 31 participants reported a duration of 6 hours (77.5%). In terms of bleeding after using the TAP block due to anticoagulant drugs, 21 participants reported experiencing bleeding (52.5%), while 19 participants did not (47.5%) as show in Figure 1. Regarding the use of ultrasound guidelines, careful needle and catheter placement, and safe fixation, only 10 participants reported that these guidelines were followed (25%), while 30 participants reported that they were not (75%). Additionally, 31 participants were obese, making the needle insertion for a TAP block more difficult due to excess subcutaneous fat (77.5%), while 9 participants were not obese (22.5%). Overall, the study found that there were some complications associated with the TAP block, such as bleeding, infection, or organ injury, 21 participants reported experiencing these complications (52.5%), while 19 participants did not (47.5%). It is important to note that the study cited several references to support its findings. These references include studies on ultrasound-guided nerve blocks [48], the efficacy of ultrasound and nerve stimulation guidance in peripheral nerve blocks [49], evidence-based management of postoperative pain [50] and preparing for ultrasound-guided biopsy [51].
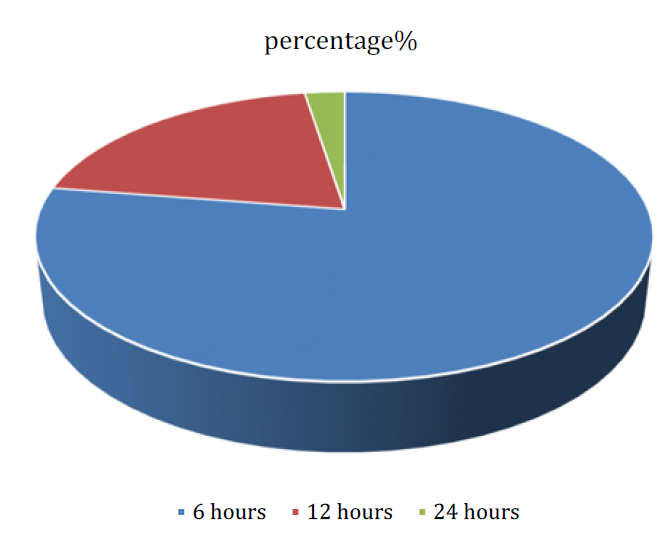
Figure 1: The Duration of Analgesia after the TAP Block of the Samples
The conclusion of the study on transversus abdominis plane (TAP) block highlighted several key disadvantages and complications associated with the procedure. These included bleeding, infection, and organ injury [2]. The study found that 52.5% of participants reported experiencing these complications, while 47.5% did not [2]. Additionally, only 25% of participants reported following ultrasound guidelines for needle and catheter placement and safe fixation [2]. Furthermore, 77.5% of participants were obese, which can make needle insertion for a TAP block more challenging due to excess subcutaneous fat [2]. Based on these findings, it is important to consider alternative techniques when the disadvantages of TAP block outweigh the benefits. Alternative techniques may be preferable in cases where there is a higher risk of complications, such as bleeding, infection, or organ injury. For example, alternative regional anesthesia techniques, such as epidural or spinal anesthesia, may be considered in certain surgical procedures to provide effective pain relief while minimizing the risk of complications [1].
In addition, the use of ultrasound guidance for nerve blocks and other procedures should be encouraged to improve accuracy and reduce the risk of complications [4] [5]. Ultrasound guidance has been shown to enhance the success rate and safety of various procedures, including nerve blocks and lumbar punctures. Therefore, incorporating ultrasound training and education into the curriculum for healthcare professionals, particularly residents, can help improve their proficiency in performing ultrasound-guided procedures [5]. Furthermore, it is crucial to carefully assess the patient's individual characteristics and medical history before deciding on the appropriate analgesic technique. Factors such as obesity, chronic diseases, and the use of anticoagulant drugs should be taken into consideration to minimize the risk of complications and optimize patient outcomes [2,4].
In conclusion, while TAP block can provide effective analgesia, it is important to be aware of the potential disadvantages and complications associated with the procedure. Alternative techniques, such as epidural or spinal anesthesia, should be considered when the risks outweigh the benefits. Incorporating ultrasound guidance into practice and individualizing the choice of analgesic technique based on patient characteristics can help improve safety and outcomes in pain management.
Das, A.K. et al. “Ultrasound-guided posterior transversus abdominis plane block versus epidural analgesia for postoperative pain relief in lower abdominal surgeries.” Journal of Medical Sciences, 2023. doi:10.4103/jmedsci.jmedsci_11_22.
El Aidy, A. et al. “Blockade of thoracoabdominal nerves through perichondrial approach (TAPA) versus transversus abdominis plane block for postoperative analgesia in pediatric abdominal surgeries.” International Journal of Health Sciences, 2022. doi:10.53730/ijhs.v6ns7.11451.
Cho, J. et al. “Transversus abdominis plane block for lumboperitoneal shunt surgery in idiopathic normal pressure hydrocephalus: a case report.” Journal of Surgical Case Reports, 2021. doi:10.1093/jscr/rjab123.
Mavarez, A.C. and Ahmed, A.A. “Transabdominal plane block.” 2020.
Tekelioglu, U.Y. et al. “Colostomy with transversus abdominis plane block.” Turkish Journal of Anesthesia and Reanimation, 2019. doi:10.5152/TJAR.2015.89410.
Malhotra, R.V. et al. “Acute local anesthetic systemic toxicity from hypogastric nerve block for chronic pelvic pain.” Neuromodulation, 2023. doi:10.1016/j.neurom.2023.04.430.
Antel, R. and Ingelmo, P. “Local anesthetic systemic toxicity.” Canadian Medical Association Journal, 2022. doi:10.1503/cmaj.220835.
López Ruiz, R. et al. “Systemic toxicity secondary to local anesthetic infiltration.” Revista de Neurología, 2022. doi:10.33588/rn.7505.2021280.
Long, B. et al. “Local anesthetic systemic toxicity: a narrative review for emergency clinicians.” American Journal of Emergency Medicine, 2022. doi:10.1016/j.ajem.2022.06.017.
Lungonyonyi, R.K. et al. “Local anesthetic systemic toxicity after local infiltration analgesia following a total knee arthroplasty.” Cureus, 2022. doi:10.7759/cureus.26224.
Nguyen, A.T. et al. “Transversus abdominis plane block in the treatment of chronic postsurgical abdominal wall pain improves patient quality of life.” Pain Physician, 2023.
Hang, D. et al. “Severe abdominal wall infection after subcostal transversus abdominis plane block: A case report.” 2021. doi:10.1213/XAA.0000000000001531.
Mavarez, A.C. and Ahmed, A.A. “Transabdominal plane block.” 2020.
Hammi, C. and Ahn, K. “Transversus abdominis plane block.” 2019.
Jinfeng, W. and Qiang, H. “Comment to: the transversus abdominis plane block reduces the cumulative need of analgesic medication following inguinal hernia repair.” Hernia, 2020. doi:10.1007/S10029-020-02206-6.
Khurana, J. et al. “Surgically inserted transversus abdominis plane catheters for flank incisions.” Canadian Journal of Urology, 2018.
Mittal, T. et al. “Efficacy of ultrasound-guided transversus abdominis plane block for postoperative analgesia in laparoscopic gastric sleeve resection.” Surgical Endoscopy, 2018. doi:10.1007/S00464-018-6261-6.
Bakshi, S.G. et al. “Transversus abdominis plane catheters for postoperative pain relief in pediatric patients.” Journal of Anaesthesiology Clinical Pharmacology, 2017. doi:10.4103/0970-9185.202187.
Das, A.K. et al. “Ultrasound-guided posterior transversus abdominis plane block versus epidural analgesia for postoperative pain relief in lower abdominal surgeries.” Journal of Medical Sciences, 2023. doi:10.4103/jmedsci.jmedsci_11_22.
Liu, H. et al. “Femoral nerve block and local instillation analgesia associated with more reliable efficacy following anterior cruciate ligament reconstruction.” Arthroscopy, 2023. doi:10.1016/j.arthro.2022.12.014.
Narasimhulu, D.M. et al. “A randomized trial comparing surgeon-administered intraoperative transversus abdominis plane block with anesthesiologist-administered transcutaneous block.” International Journal of Obstetric Anesthesia, 2018. doi:10.1016/J.IJOA.2018.04.007.
Das, A.K. et al. “Ultrasound-guided posterior transversus abdominis plane block versus epidural analgesia for postoperative pain relief in lower abdominal surgeries.” Journal of Medical Sciences, 2023. doi:10.4103/jmedsci.jmedsci_11_22.
Ahmed, M. et al. “The analgesic efficacy of transversus abdominis plane block versus epidural analgesia in laparoscopic lower abdominal surgeries in adults.” Global Journal for Research Analysis, 2023. doi:10.36106/gjra/0713396.
Thakkar, J.M. et al. “Efficacy of ultrasound-guided transversus abdominis plane block versus epidural block for postoperative analgesia following lower abdominal cancer surgeries.” Journal of Clinical and Diagnostic Research, 2023. doi:10.7860/jcdr/2023/60697.17835.
Hang, D. et al. “Severe abdominal wall infection after subcostal transversus abdominis plane block: a case report.” 2021. doi:10.1213/XAA.0000000000001531.
Poredos, P. “Peripheral nerve blocks in patients on antithrombotic drugs.” Acta Clinica Croatica, 2022. doi:10.20471/acc.2022.61.s2.08.
Goudreau, S. et al. “Bleeding complications after breast core-needle biopsy.” Journal of Breast Imaging, 2022. doi:10.1093/jbi/wbac020.
Kietaibl, S. et al. “Regional anaesthesia in patients on antithrombotic drugs.” European Journal of Anaesthesiology, 2022. doi:10.1097/EJA.0000000000001600.
Ruiz-Tovar, J. et al. “The TAP block in obese patients: pros and cons.” Minerva Anestesiologica, 2019. doi:10.23736/S0375-9393.19.13545-6.
Matejic-Spasic, M. et al. “Management of perioperative bleeding risk in patients on antithrombotic medications undergoing cardiac surgery.” Journal of Thoracic Disease, 2022. doi:10.21037/jtd-22-428.
Bakhtawar, J. and Siraj, S. “Anesthetic management and role of TAP block in a pregnant patient with Guillain–Barré syndrome.” Pakistan Journal of Health Sciences, 2023. doi:10.54393/pjhs.v4i06.831.
Prajapati, S. and Brahmbhatt, N. “Analgesic efficacy of ultrasound-guided transversus abdominis plane block after caesarean delivery.” Indian Journal of Clinical Anaesthesia, 2021. doi:10.18231/J.IJCA.2021.038.
Mashal, M.O. et al. “Evaluation of analgesic effect of transversus abdominis plane block after emergency cesarean section.” 2021. doi:10.21608/BJAS.2021.188857.
Shahmoradi, M.K. et al. “Analgesic effects of TAP block among open appendectomy patients.” International Journal of Surgery Open, 2020. doi:10.1016/J.IJSO.2020.11.015.
Narasimhulu, D.M. et al. “A randomized trial comparing surgeon-administered intraoperative transversus abdominis plane block with anesthesiologist-administered transcutaneous block.” International Journal of Obstetric Anesthesia, 2018. doi:10.1016/J.IJOA.2018.04.007.
Kristianto, H. et al. “Neuromuscular taping application opportunities in nursing: a literature review.” 2020. doi:10.15452/CEJNM.2020.11.0018.
van Loon, F.H.J. et al. “Establishing the required components for training in ultrasound-guided peripheral intravenous cannulation.” Medical Ultrasonography, 2019. doi:10.11152/MU-2120.
Charnoff, J. et al. “Resident education of ultrasound-guided procedures.” American Journal of Physical Medicine & Rehabilitation, 2019. doi:10.1097/PHM.0000000000001259.
Millington, S.J. et al. “Better with ultrasound: lumbar puncture.” Chest, 2018. doi:10.1016/J.CHEST.2018.07.010.
Huang, J. et al. “The principles and procedures of ultrasound-guided anesthesia techniques.” Cureus, 2018. doi:10.7759/CUREUS.2980.
Ohseto, K. et al. “Ultrasound-guided method.” 2019. doi:10.1007/978-4-431-54660-3_12.
Puntillo, F. et al. “US-guided nerve blocks: procedure technique.” 2018. doi:10.1007/978-3-319-71020-4_5.
Kirschner, J.S. and Furman, M.B. “Needle techniques.” 2018. doi:10.1016/B978-0-323-40153-1.00002-0.
Orebaugh, S.L. and Bigeleisen, P.E. “Nerve roots, trunks, and the vagaries of ultrasound.” Regional Anesthesia and Pain Medicine, 2017. doi:10.1097/AAP.0000000000000534.
Subramani, S. and Punia, S. “Lower extremity nerve blocks.” 2021. doi:10.1007/978-981-15-9202-7_3.
Ohseto, K. et al. “Ultrasound-guided method.” 2019. doi:10.1007/978-4-431-54660-3_12.
McVicar, J. et al. “Ultrasound-guided upper extremity blocks.” 2018. doi:10.1007/978-1-4939-7754-3_19.
Puntillo, F. et al. “US-guided nerve blocks: procedure technique.” 2018. doi:10.1007/978-3-319-71020-4_5.
Wang, Z.X. et al. “Efficacy of ultrasound and nerve stimulation guidance in peripheral nerve block.” IUBMB Life, 2017. doi:10.1002/IUB.1654.
Joshi, G.P. et al. “Author’s reply: evidence-based management of postoperative pain in adults undergoing laparoscopic sleeve gastrectomy.” World Journal of Surgery, 2020. doi:10.1007/S00268-020-05673-1.
Fornage, B.D. “Preparing for ultrasound-guided biopsy.” 2020. doi:10.1007/978-3-030-20829-5_4.
Hersch, L. et al. “Dispelling myths about antenatal TAPS.” Journal of Clinical Medicine, 2019. doi:10.3390/JCM8070977.
Shahait, M. and Lee, D.I. “Application of TAP block in laparoscopic urological surgery.” Current Urology Reports, 2019. doi:10.1007/S11934-019-0883-7.
Millington, S.J. et al. “Better with ultrasound: lumbar puncture.” Chest, 2018. doi:10.1016/J.CHEST.2018.07.010.
