
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-953X
ISSN (Online) : 2788-9548
Malignant melanoma (MM) of oral cavity is a rare tumor with incidence ranging from o.2-8% of all melanomas. It is a potentially aggressive tumor of melanocytic origin with high tendency to metastasize. Due to its rarity, asymptomatic presentation, high suspicion for diagnosis and a lack of defined treatment strategies, make it a poor prognostic tumor. Here we are reporting a rare case of oral malignant melanoma in a 63 yr old male undergoing treatment with chemotherapy at our centre.
Case Report
A 63 yr old male patient presented to us with history of a blackish patch over hard palate from last 6 months. It was gradually progressive in size and occasionally associated with mild pain. There is a history of occasional bleeding episodes from the blackish patch site. Patient was a chronic smoker and used to consume alcohol on a daily basis from last 45 years. On examination of the oral cavity a blackish patch was present over hard palate (Figure 1).
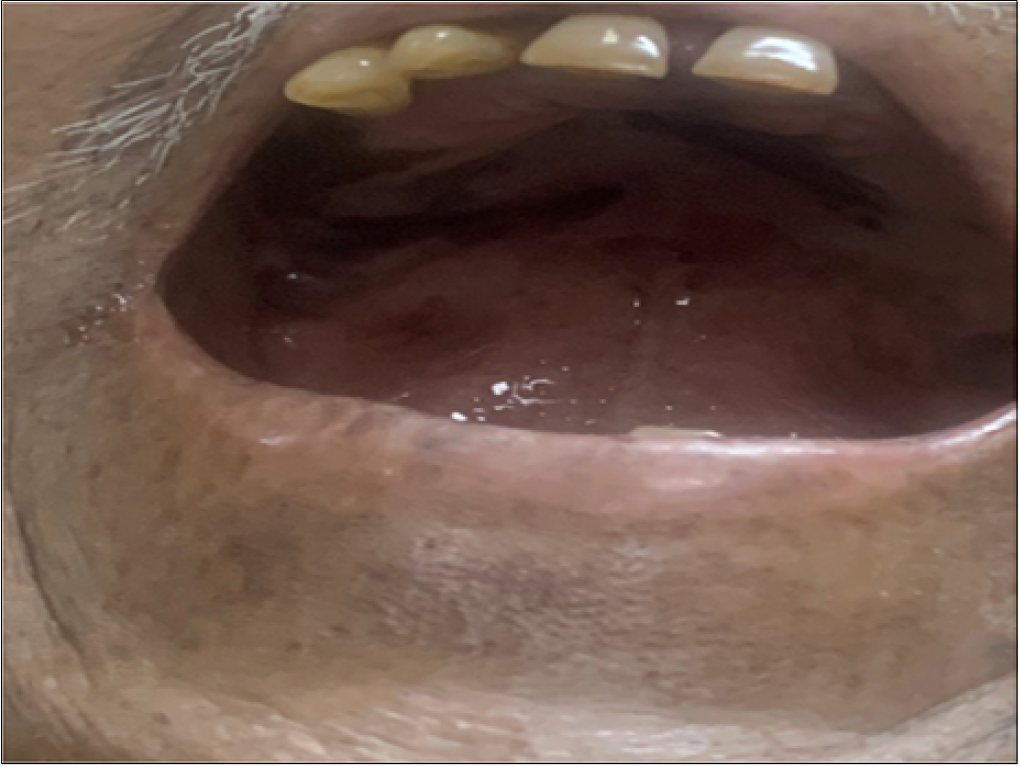
Figure 1: Intraoral View Showing Oral Cavity and Palatal Mucosa
It was a diffuse patch, asymmetrical with irregular borders involving whole of the palate, not involving the gums. On examination of the neck no lymph nodes were palpated. Rest of systemic examination was normal. A CT scan was done from base of skull to T4 vertebral level which showed mucosal thickening heterogeneously enhancing measuring 86x20x27mm. No loco regional soft tissue destruction was seen. Sub centimetric cervical lymph nodes were present. A biopsy was performed from the lesion site. It showed tumor cells in sub epithelium arranged in form of nests and sheets with high nucleo cytoplasmic ratio, prominent nuclei and moderate cytoplasm. Cytoplasm of tumor cells showed melanin pigment (Figure 2).
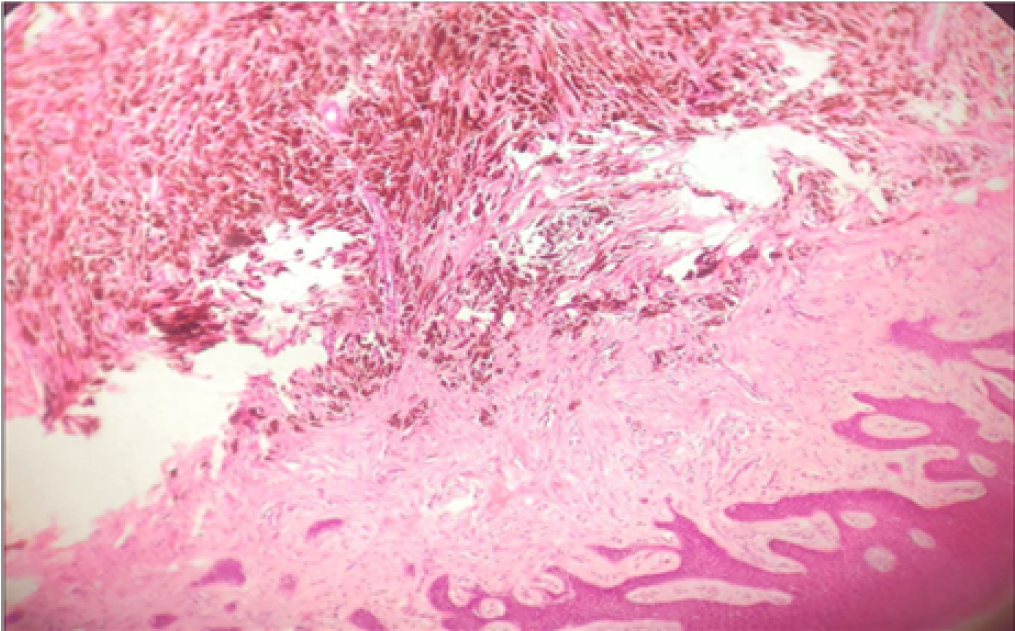
Figure 2: 10x Magnification
On immunohistochemsitry tumor cells stained positive for S-100 and HMB45 and Vimentin. Hence, with above clinical and pathological findings a diagnosis of malignant melanoma of hard palate was made.
Patient and his family were then counseled about the disease and its prognosis. Patient is undergoing chemotherapy at our centre and has completed 3 cycles so far.
Oral malignant melanoma is a rare cancer with incidence of 0.2-8% of all malignant melanomas [1]. It affects adult individuals highest in the sixth decade with a slight male dominance [2]. The risk factors include cigarette smoking, alcohol intake, chronic irritation and ill fitting dentures [2]. In our patient there is history of chronic cigarette smoking and alcohol intake.
Malignant melanoma is diagnosed at a later stage as it is asymptomatic initially. The most common symptoms at presentation are a blackish colored patch, pain, bleeding and tooth misalignment. Satellite foci may be present surrounding the lesion. In our patient a diffuse black patch was present over hard palate with occasional bleeding episodes and pain [4].
The diagnosis of malignant melanoma is established after biopsy. In biopsy atypical nuclear cells arranged as nests and sheets with eosinophilic nuclei and melanin pigment in stroma are present. Greene et al, gave criteria for diagnosis of oral malignant melanoma as 1) demonstration of malignant melanoma in oral cavity 2) presence of junctional activity as melanocytes arranged along the basal layer of surface epithelium 3) Inability to show malignant melanoma at any other primary site [6].
The cells stain positive for S-100, HMB45, Vimentin, Melan-A stains [5]. In our patient the cells stained positive for S-100 and HMB45.
The differential diagnosis includes melanotic macule, smoking associated melanosis, melanoplakia, melanoacanthoma, nevi, post inflammatory pigmentation, Addison’s disease, Peuts-Jeghur syndrome, amalgam tattoo, Kaposi’s sarcoma, azidothymidine induced pigmentation [4]
Treatment of oral malignant melanoma is radical surgery. Radical surgery with wide excision and negative margins is the treatment of choice. Neck dissection is indicated for clinically positive neck nodes. Role of radiotherapy is mainly to achieve enhanced local control and increased relapse free survival. Role of chemotherapy and immunotherapy is very limited in the treatment of oral malignant melanoma and is done mainly in metastatic disease [4].For older adults or individuals where surgery is not possible radical surgery in combination with radiation and chemotherapy or radiotherapy as a sole modality is preferred [2]. OMM has high chances of metastasis due to rich lymphatic and vascular drainage in head and neck region. It metastasise to lungs, liver, vertebrae or brain. Prognosis of oral malignant melanoma is worse than cutaneous one due to chameleonic nature and late diagnosis of oral malignant melanoma. 5 year survival rate of 31% for localized disease and 5.2% if cervical lymphadenopathy is present [6].
Oral Malignant Melanoma of hard palate is a rare tumor which is aggressive and has a high tendency to metastasise. So a prompt early diagnosis with high suspicion followed by effective intervention is warranted.
Pandey M. et al. “Primary malignant mucosal melanoma of the head and neck region: pooled analysis of 60 published cases from India and review of literature.” European Journal of Cancer Prevention, vol. 11, no. 1, 2002, pp. 3–10.
Sabanathan S., Eng J. and Pradhan G.N. “Primary malignant melanoma of the esophagus.” American Journal of Gastroenterology, vol. 84, no. 12, 1989, pp. 1475–1481.
Tanaka N. et al. “Malignant melanoma in the oral region: ultrastructural and immunohistochemical studies.” Medical Electron Microscopy, vol. 34, no. 3, 2001, pp. 198–205.
Zito P.M. and Mazzoni T. “Oral melanoma.” StatPearls, StatPearls Publishing, Treasure Island (FL), 2021. Available at: https://www.ncbi.nlm.nih.gov/books/NBK513276/
Meleti M. et al. “Oral malignant melanoma: the Amsterdam experience.” Journal of Oral and Maxillofacial Surgery, vol. 65, no. 11, 2007, pp. 2181–2186.
Bartkowski S.B. et al. “Primary malignant melanoma of the oral cavity: a review of 20 cases.” American Journal of Surgery, vol. 148, no. 3, 1984, pp. 362–366.
