
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-953X
ISSN (Online) : 2788-9548
Scar endometriosis is a rare but significant complication of cesarean section, resulting from the iatrogenic implantation of endometrial cells into the surgical wound. It often presents as a painful, progressively enlarging mass at the incision site, leading to frequent misdiagnosis as a hernia, neuroma, or ovarian pathology. We report a case of a 29-year-old woman with a history of cesarean section (4 years prior) who presented with persistent lower abdominal pain and a firm, tender suprapubic mass (6×6 cm). Initially misdiagnosed as a twisted ovarian cyst, ultrasonography revealed a heterogeneous, hypoechoic mass (5×3×4 cm) within the rectus abdominis muscle, raising suspicion for scar endometriosis. Due to uncertain diagnosis and worsening pain, an exploratory laparotomy was performed, revealing a 6×4 cm jumbled-up mass comprising the rectus sheath, rectus muscle, and parietal peritoneum, containing chocolate-colored fluid, characteristic of endometriotic cysts. Complete surgical excision was performed, and histopathology confirmed endometriotic glands and stroma with hemosiderin-laden macrophages, establishing the diagnosis. Postoperatively, the patient received Medroxyprogesterone acetate (500 mg monthly for 3 months) to reduce recurrence risk and remained asymptomatic at 6-month follow-up. This case highlights the importance of considering scar endometriosis in women presenting with localized pain over prior surgical scars. Given its potential for misdiagnosis, early clinical suspicion, imaging, and histopathological confirmation are essential. Complete surgical excision remains the gold standard treatment, ensuring long-term relief and preventing recurrence.
Endometriosis is a chronic gynecological disorder characterized by the presence and proliferation of ectopic endometrial tissue outside the uterine cavity. It is estimated to affect 5-10% of reproductive-age women worldwide, often leading to chronic pelvic pain, dysmenorrhea, dyspareunia, and infertility.1,2 While the most common sites of endometriotic implants include the ovaries, peritoneum, and fallopian tubes, scar endometriosis (SE) is a rare yet increasingly recognized form of the disease, occurring in less than 1% of endometriosis cases [3,4].
Scar endometriosis is defined as the implantation of endometrial tissue within a surgical scar, most commonly cesarean section or laparotomy incisions. The most widely accepted etiology is iatrogenic transplantation, wherein endometrial cells are inadvertently introduced into the wound during pelvic surgery and subsequently proliferate under hormonal influence.5,6 Clinically, scar endometriosis presents as a tender, firm mass within or adjacent to the surgical scar, often exhibiting cyclical changes in size and pain intensity in relation to the menstrual cycle. However, in some cases, these cyclical variations may be absent, leading to diagnostic uncertainty and potential misdiagnosis as a hernia, hematoma, neuroma, abscess, lipoma, or even metastatic carcinoma [6-8].
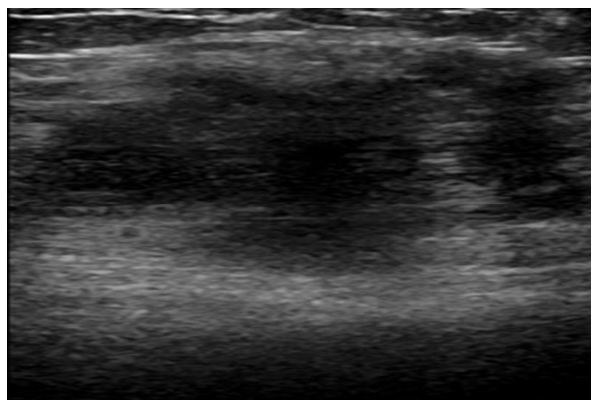
Figure 1: Heterogenous Hypoechoic Mass at Sonography
The incidence of scar endometriosis ranges from 0.03% to 0.15% of all endometriosis cases, making it a rare but important differential diagnosis in womenpresenting with persistent abdominal pain at previous surgical sites. Due to its atypical presentation and low prevalence, preoperative diagnosis remains challenging, with studies suggesting that only 20-50% of cases are accurately diagnosed before surgical intervention. Ultrasonography (USG) serves as the primary imaging modality, often revealing a heterogeneous, hypoechoic mass, while histopathological examination of excised tissue remains the gold standard for confirmation [9-11].
Management of scar endometriosis involves both medical and surgical approaches. Hormonal therapy with progestins, oral contraceptives, or GnRH analogs may offer symptomatic relief; however, it is often ineffective in completely resolving the condition.12,13 Wide surgical excision with clear margins is considered the definitive treatment, reducing the risk of recurrence and ensuring symptom resolution. Notably, 14-26% of patients with scar endometriosis also have concomitant pelvic endometriosis, necessitating thorough intraoperative evaluation and long-term follow-up [13,14].
Given the increasing number of cesarean sections performed worldwide, the incidence of scar endometriosis is likely to rise, underscoring the need for heightened clinical awareness, early diagnosis, and prompt intervention. This article presents a comprehensive case study of cesarean scar endometriosis, detailing its diagnosis, surgical management, and histopathological findings, while also discussing the broader implications for clinical practice and future research.
Patient Profile and Clinical History
A 29-year-old woman, para 1, presented with complaints of acute lower abdominal pain for the past 15 days, localized to the suprapubic region near her previous cesarean section scar. The pain was progressive, dull, and aching, with occasional sharp exacerbations. She had undergone an uncomplicated cesarean section 4 years ago via a Pfannenstiel incision for fetal distress at term. Additionally, she had a history of cholecystectomy 2 years prior, with no residual complications. For the past two years, she had been experiencing progressive dysmenorrhea, but denied any menorrhagia or intermenstrual bleeding. She initially sought care at a peripheral hospital, where she was misdiagnosed with a twisted ovarian cyst and referred to our institution for further evaluation and management.
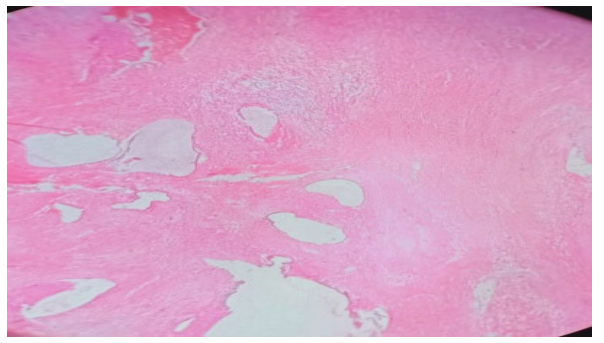
Figure 2: Histopathology showing endometriotic gland and stroma in subcutaneous tissue
Clinical Examination and Initial Evaluation
On examination, the patient was in moderate distress due to persistent lower abdominal pain. General physical examination revealed stable vital signs with no systemic manifestations. Abdominal examination showed a well-healed Pfannenstiel cesarean scar, with an underlying ill-defined, firm, and tender mass measuring 6×6 cm on the right suprapubic region, lateral to the midline. The mass was fixed with restricted mobility, and tenderness was significantly exacerbated on deep palpation. There were no signs of overlying skin changes, abscess formation, or sinus discharge. Per speculum examination revealed a healthy cervix and vaginal mucosa, with no abnormal vaginal discharge. Per vaginal examination confirmed the presence of a firm, non-mobile, and tender suprapubic mass that was separate from the uterus and adnexa.
Imaging and Preoperative Diagnosis
Transabdominal ultrasonography (USG) revealed a heterogeneous, hypoechoic, oval-shaped mass measuring 5×3×4 cm within the right rectus abdominis muscle, with internal cystic areas but no vascular flow on Doppler imaging. The uterus and ovaries appeared normal, ruling out ovarian pathology. Given the uncertain preoperative diagnosis and the progressive nature of the patient’s symptoms, a decision was made to proceed with exploratory laparotomy for definitive diagnosis and management.
Surgical Management and Intraoperative Findings
A transverse incision was made to provide optimal exposure of the anterior abdominal wall. Intraoperatively, a jumbled-up mass measuring 6×4 cm was identified, comprising rectus sheath, rectus muscle, and parietal peritoneum. The mass was firmly adherent to the surrounding tissues and contained chocolate-colored fluid, which is a characteristic feature suggestive of endometriotic cyst formation. Sharp dissection was performed to separate the mass from the peritoneum, and complete excision of the lesion was undertaken. The rectus sheath was reconstructed using Prolene 1-0 sutures to restore anatomical integrity. The excised specimen was sent for histopathological examination to confirm the diagnosis.

Figure 3(a): Excised Mass Showing Brown Colored Area
Histopathological Findings
Microscopic examination of the excised specimen showed endometriotic glands and stroma embedded within the subcutaneous and muscle tissues, confirming the diagnosis of scar endometriosis. The presence of hemosiderin-laden macrophages indicated chronic hemorrhage and recurrent cyclical bleeding within the lesion. Additional findings included chronic inflammatory infiltrates and fibrosis, suggestive of long-standing disease. There was no evidence of malignant transformation or atypical cellular changes.
Postoperative Recovery and Follow-Up
The patient’s immediate postoperative course was uneventful, with appropriate pain management and prophylactic antibiotics administered. She was mobilized early and discharged on postoperative day 4 with instructions for wound care and pain management. To reduce the risk of recurrence, she was initiated on Medroxyprogesterone acetate 500 mg once monthly for 3 months as adjunctive hormonal therapy. At the 6-month follow-up visit, the patient reported complete resolution of pain, with no recurrence of the mass or new-onset symptoms. She remained asymptomatic during follow-up, confirming the effectiveness of surgical excision as definitive treatment.
Scar endometriosis, though rare, is an important differential diagnosis in women presenting with localized pain and a palpable mass at previous surgical incision sites, particularly following cesarean section or pelvic surgeries. This case exemplifies the diagnostic challenges associated with the condition, as the patient was initially misdiagnosed with a twisted ovarian cyst, delaying appropriate treatment. The absence of classical cyclical pain, which is typically observed in pelvic endometriosis, further complicated early recognition. This highlights the need for heightened clinical awareness and a high index of suspicion in patients presenting with persistent pain and a progressively enlarging mass over a previous surgical scar.
Pathogenesis and Etiology
The iatrogenic transplantation theory remains the most widely accepted explanation for the development of scar endometriosis. During cesarean section, endometrial cells may inadvertently be deposited within the surgical wound while closing the uterine incision. These ectopic endometrial cells then proliferate and establish functional endometriotic implants in the rectus abdominis muscle, rectus sheath, or subcutaneous tissue, leading to the characteristic clinical manifestations of scar endometriosis. Other proposed mechanisms, such as lymphatic or vascular dissemination and coelomic metaplasia, are less likely in the absence of concomitant pelvic endometriosis [14-16].
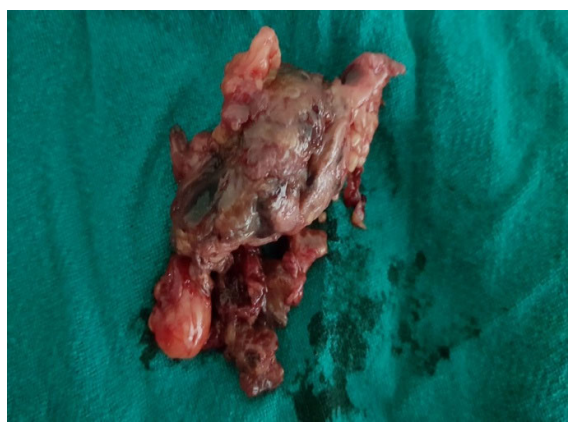
Figure 3(b): Excised Mass Showing Brown Colored Area
In this case, the patient developed symptoms four years after her cesarean section, which is consistent with the literature reporting a typical latency period of 3–4 years. The progression of pain and mass enlargement over time aligns with the gradual proliferation of ectopic endometrial tissue, repeated episodes of microhemorrhage, and resultant fibrotic tissue formation. The fact that she had no history of prior symptoms suggests that subclinical implantation of endometrial cells occurred intraoperatively, which only became symptomatic as the lesion enlarged.
Clinical Presentation and Diagnostic Challenges
The clinical presentation of scar endometriosis is often insidious, with patients initially reporting mild discomfort over the incision site, which progressively worsens. The classic feature of cyclical pain, which is observed in up to 50% of cases, was absent in our patient, making diagnosis more difficult. The presence of a firm, ill-defined, tender mass at the suprapubic region raised suspicion for several differential diagnoses, including hernia, hematoma, neuroma, abscess, or lipoma, delaying definitive diagnosis [7,17,18].
A notable observation in this case was the restricted mobility of the mass on palpation, which suggested involvement of deeper structures, including the rectus muscle and parietal peritoneum. The mass was misdiagnosed at the peripheral hospital as a twisted ovarian cyst, emphasizing the importance of considering non-gynecological causes of acute lower abdominal pain, particularly in post-cesarean patients.
Role of Imaging in Diagnosis
Imaging plays a crucial role in the evaluation of scar endometriosis, though no single modality provides definitive confirmation. Ultrasonography (USG) is often the first-line imaging tool, given its accessibility and ability to detect heterogeneous, hypoechoic masses with internal cystic components, as was seen in this case. However, USG lacks specificity, and additional imaging techniques, such as magnetic resonance imaging (MRI), may be required for deep or complex lesions [6,7,19,20].
In this patient, transabdominal USG revealed a 5×3×4 cm heterogeneous, oval-shaped mass within the rectus abdominis muscle, a typical finding in scar endometriosis. Despite this, the diagnosis remained uncertain due to the overlapping radiologic features with other soft tissue pathologies. The definitive diagnosis was only confirmed intraoperatively and through histopathological examination.
Surgical Excision: The Definitive Treatment
The gold standard treatment for scar endometriosis is complete surgical excision with clear margins, as medical therapy alone is insufficient for long-term symptom resolution. Hormonal suppression with progestins, GnRH analogs, or oral contraceptives may offer temporary relief by suppressing ectopic endometrial tissue activity, but lesions frequently recur after discontinuation of therapy, making surgery the preferred approach [6,21,22].
In this case, exploratory laparotomy was performed due to the unclear preoperative diagnosis and worsening symptoms. Intraoperatively, a 6×4 cm well-encapsulated mass was found within the rectus sheath, rectus muscle, and parietal peritoneum, containing chocolate-colored fluid, a characteristic feature of endometriotic cysts. The firm adherence of the mass to surrounding structures necessitated meticulous dissection to ensure complete removal, and the rectus sheath was repaired with Prolene 1-0 sutures to restore abdominal wall integrity.
Histopathological Confirmation
Histopathological examination of the excised mass remains the gold standard for definitive diagnosis. In this case, microscopic analysis confirmed the presence of endometriotic glands and stroma within the subcutaneous and muscular layers, along with hemosiderin-laden macrophages, consistent with repeated episodes of localized hemorrhage and fibrosis. The absence of malignant transformation was reassuring, as rare cases of endometrioid carcinoma or clear cell carcinoma arising from scar endometriosis have been reported in the literature [23-25].
Postoperative Prognosis and Risk of Recurrence
Following complete surgical excision, the prognosis for scar endometriosis is excellent, with low recurrence rates when negative margins are achieved. In cases where excision is incomplete, recurrence rates can be as high as 10-15%, necessitating reoperation. In our patient, postoperative recovery was uneventful, and she was discharged on postoperative day 4 with no residual pain or complications [26,27].
To minimize the risk of recurrence, adjunctive hormonal therapy with Medroxyprogesterone acetate (500 mg once monthly for three months) was prescribed, though the necessity of postoperative medical treatment remains controversial. At the 6-month follow-up, the patient remained asymptomatic, with no evidence of mass recurrence, confirming the efficacy of definitive surgical excision.
Concomitant Pelvic Endometriosis Consideration
An important consideration in scar endometriosis cases is the potential coexistence of pelvic endometriosis, which has been reported in 14-26% of patients. Although our patient had no intraoperative evidence of pelvic endometriosis, the possibility of microscopic implants elsewhere in the pelvis cannot be completely ruled out. This underscores the need for long-term follow-up and continued surveillance for the development of new symptoms suggestive of pelvic disease [7,21,15,28].
Clinical Implications and Future Considerations
This case highlights the importance of maintaining a high index of suspicion for scar endometriosis in women presenting with pain localized to previous surgical scars, particularly following cesarean delivery. Early recognition, timely imaging, and definitive surgical excision can prevent unnecessary diagnostic delays and improve patient outcomes. Given the rising global cesarean section rates, the incidence of scar endometriosis is expected to increase, necessitating greater awareness among gynecologists, general surgeons, and radiologists.
Future research should focus on improving preoperative diagnostic accuracy, potentially through advanced imaging techniques or biomarker-based approaches, to differentiate scar endometriosis from other abdominal wall masses. Additionally, surgical techniques that minimize iatrogenic implantation of endometrial tissue during cesarean section, such as copious peritoneal lavage before abdominal closure, warrant further exploration.
By raising clinical awareness and emphasizing early intervention, cases of scar endometriosis can be identified and managed effectively, ensuring better patient outcomes and preventing prolonged morbidity associated with delayed or missed diagnoses.
Scar endometriosis is a rare but significant complication following cesarean section, often presenting as a progressively enlarging, painful mass at the incision site, sometimes years after surgery. The diagnostic challenge arises from its variable presentation, with many cases lacking the classical cyclical pain associated with endometriosis, leading to frequent misdiagnosis as hernias, hematomas, or neoplastic lesions. Imaging, particularly ultrasonography, plays a key role in initial assessment, but definitive diagnosis relies on histopathological confirmation following surgical excision. As seen in this case, wide surgical excision with clear margins remains the gold standard treatment, ensuring complete symptom resolution and minimizing recurrence risk. Given the increasing global cesarean section rates, awareness of scar endometriosis among clinicians is crucial for early recognition, timely intervention, and improved patient outcomes.
Smolarz, Beata, et al. “Endometriosis: Epidemiology, classification, pathogenesis, treatment and genetics (review of literature).” International Journal of Molecular Sciences, vol. 22, no. 19, September 2021. http://dx.doi.org/10.3390/ijms221910554.
Cano-Herrera, Gabriela, et al. “Endometriosis: A comprehensive analysis of the pathophysiology, treatment, and nutritional aspects, and its repercussions on the quality of life of patients.” Biomedicines, vol. 12, no. 7, July 2024. http://dx.doi.org/10.3390/biomedicines12071476.
Hill, Christopher J., et al. “Endometriosis and the fallopian tubes: Theories of origin and clinical implications.” Journal of Clinical Medicine, vol. 9, no. 6, June 2020. http://dx.doi.org/10.3390/jcm9061905.
Machairiotis, Nikolaos, et al. “Extrapelvic endometriosis: A rare entity or an under diagnosed condition?.” Diagnostic Pathology, vol. 8, no. 1, December 2013. http://dx.doi.org/10.1186/1746-1596-8-194.
Poudel, Diptee, et al. “A case of scar endometriosis in cesarean scar: A rare case report.” International Journal of Surgery Case Reports, vol. 102, January 2023. http://dx.doi.org/10.1016/j.ijscr.2022.107852.
Durairaj, Anitha, et al. “Surgical scar endometriosis: An emerging enigma.” Cureus, vol. 15, no. 2, February 2023. http://dx.doi.org/10.7759/cureus.35089.
anielpour, Payman J, et al. “Scar endometriosis – a rare cause for a painful scar: A case report and review of the literature.” Canadian Journal of Plastic Surgery, vol. 18, no. 1, March 2010, pp. 19-20. http://dx.doi.org/10.1177/229255031001800110.
Kapoor, Deepa, et al. “Scar endometriosis in a patient with previous caesarean scar - a case report.” The New Indian Journal of OBGYN, vol. 4, no. 1, July 2017, pp. 90-93. http://dx.doi.org/10.21276/obgyn.2017.4.1.19.
Kotdawala, Kanan P, et al. “Scar endometriosis: A case report of a rare complication of laparotomy for ectopic pregnancy.” Journal of South Asian Federation of Obstetrics and Gynaecology, vol. 13, no. 1, February 2021, pp. 68-70. http://dx.doi.org/10.5005/jp-journals-10006-1866.
Minaglia, Steven et al. “Incisional endometriomas after Cesarean section: a case series.” The Journal of reproductive medicine, vol. 52, no. 7, 2007, pp. 630-634. https://pubmed.ncbi.nlm.nih.gov/17847762/.
Rao, C. V. Lakshmi, et al. “Scar ENDOMETRIOSIS: A case series and review of literature.” International Journal of Scientific Study, July 2015 vol. 3, no. 4, pp. 180-183. https://www.ijss-sn.com/uploads/2/0/1/5/20153321/ijss_jul_cr05.pdf.
Al Hussaini, Hussam Al Deen, et al. “Management of endometriosis-related pain: Comparing the effectiveness of hormonal therapy, surgical interventions, and complementary therapies.” Cureus, vol. 16, no. 12, December 2024. http://dx.doi.org/10.7759/cureus.75590.
Rafique, SAIMA, and ALAN H. Decherney. “Medical management of endometriosis.” Clinical Obstetrics & Gynecology, vol. 60, no. 3, September 2017, pp. 485-496. http://dx.doi.org/10.1097/grf.0000000000000292.
Uçar, Mustafa Gazi, et al. “Surgical treatment of scar endometriosis following cesarean section, a series of 12 cases.” Indian Journal of Surgery, vol. 77, no. S2, September 2013, pp. 682-686. http://dx.doi.org/10.1007/s12262-013-0978-1.
Adriaanse, B. M. E., et al. “Scar endometriosis after a caesarean section: A perhaps underestimated complication.” Gynecological Surgery, vol. 10, no. 4, August 2013, pp. 279-284. http://dx.doi.org/10.1007/s10397-013-0807-3.
Adriaanse, B. M. E., et al. “Scar endometriosis after a caesarean section: A perhaps underestimated complication.” Gynecological Surgery, vol. 10, no. 4, August 2013, pp. 279-284. http://dx.doi.org/10.1007/s10397-013-0807-3.
Kocher, Madison Rush, et al. “Cesarean-section scar endometrioma: A case report and review of the literature.” Journal of Radiology Case Reports, vol. 11, no. 12, December 2017, pp. 16-26. http://dx.doi.org/10.3941/jrcr.v11i12.3178.
Nepali, Rohit, et al. “Scar endometriosis: A rare cause of abdominal pain.” Dermatopathology, vol. 9, no. 2, May 2022, pp. 158-163. http://dx.doi.org/10.3390/dermatopathology9020020.
Roi, Dylan Paul, et al. “Scar endometriosis: A mimic of acute abdominal emergencies.” BJR|case reports, vol. 3, no. 3, September 2017. http://dx.doi.org/10.1259/bjrcr.20170019.
Quesada, Juan, et al. “Endometriosis: A multimodal imaging review.” European Journal of Radiology, vol. 158, January 2023. http://dx.doi.org/10.1016/j.ejrad.2022.110610.
Furness, Susan, et al. “Pre and post-operative medical therapy for endometriosis surgery.” Cochrane Database of Systematic Reviews, vol. 2004, no. 3, July 2004. http://dx.doi.org/10.1002/14651858.cd003678.pub2.
Khanna, Vidisha, et al. “Caesarean scar endometriosis: A case report.” Indian Journal of Obstetrics and Gynecology Research, vol. 9, no. 2, May 2022, pp. 292-295. http://dx.doi.org/10.18231/j.ijogr.2022.054.
Nisenblat, Vicki, et al. “Imaging modalities for the non-invasive diagnosis of endometriosis.” Cochrane Database of Systematic Reviews, vol. 2016, no. 2, February 2016. http://dx.doi.org/10.1002/14651858.cd009591.pub2.
Bhat, Shubha P., et al. “Endometriosis: A clinicopathological study in a tertiary care hospital.” Journal of Laboratory Physicians, vol. 12, no. 03, November 2020, pp. 184-190. http://dx.doi.org/10.1055/s-0040-1720946.
Pathade, Sumedha, et al. “Scar endometriosis: An uncommon surgical aftermath.” International Journal of Reproduction, Contraception, Obstetrics and Gynecology, vol. 11, no. 3, February 2022, pp. 947-950. http://dx.doi.org/10.18203/2320-1770.ijrcog20220584.
Zhong, Qiyu, et al. “Risk factors for postoperative recurrence of cesarean scar endometriosis.” AJOG Global Reports, vol. 4, no. 2, May 2024. http://dx.doi.org/10.1016/j.xagr.2024.100349.
Zakhari, Andrew, et al. “Endometriosis recurrence following post-operative hormonal suppression: A systematic review and meta-analysis.” Human Reproduction Update, vol. 27, no. 1, October 2020, pp. 96-107. http://dx.doi.org/10.1093/humupd/dmaa033.
Malutan, Andrei Mihai, et al. “Surgical scar endometriosis: A series of 14 patients and brief review of literature.” Medicine and Pharmacy Reports, vol. 90, no. 4, October 2017, pp. 411-415. http://dx.doi.org/10.15386/cjmed-743.
