
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9432
ISSN (Online) : 2788-9440
Background: Giant Lumbar Disc Herniation (GLDH) is a rare condition. Its treatment could be surgical or non-surgical. We describe in this study the surgical management of patients with GLDH in Sylvanus Olympio teaching hospital of Lomé (Togo). Patients and Methods: We conducted a retrospective and descriptive study between September 2017 and October 2020. We included in the study adult patients presented with radicular pain symptoms or cauda equina syndrome, with lumbar disc herniation in the canal superior to 50% of the sagittal diameter of the lumbar spine. Results: Thirteen patients were operated on from a GLDH. This patient population was composed of 9 men (69.2%) and four women (30.8%). The mean age of the patient population was 43.23±6.723 years (range 33-55). The anatomical location of a herniated disc was centrally in 8 patients (61.5%). The level of the GLDH was between L4-L5 in 69.2 % cases (n = 9) and L5-S1 in 30.8% (n = 4). There was no complication during surgery. Evolution was graded as excellent in 76.9 % cases (n = 10) and good in 23.1% (n = 3). Conclusion: GLDH is a distinct entity compared with smaller herniations. Patients can develop cauda equina syndrome. Surgery has good results in our conditions.
Giant or massive disc herniation is a disc occupying more than 50% or 75% of the anterior-posterior diameter of the spinal canal [1-3]. Giant Lumbar Disc Herniation (GLDH) is a rare condition [1,4]. The treatment of GLDH could be surgical or non-surgical [4-7] We describe the surgical management of patients with GLDH in Sylvanus Olympio teaching hospital of Lomé (Togo).
Study Design
Togo is a West African francophone low-income country. The population was 8,082,366 inhabitants in 2019. The Gross Domestic Product (GDP) is USD 5.49 billion in 2019. According to the World Bank, Life expectancy was 61.042 years old in 2019.
We conducted a retrospective and descriptive study at the neurosurgery unit of Sylvanus Olympio teaching hospital in a developing country (Togo) between September 2017 and October 2020. After approval of the hospital's ethics committee, we included in the study adult patients presented with radicular pain symptoms or cauda equina syndrome, with lumbar disc herniation in the canal superior to 50% of the sagittal diameter of the lumbar spine. We excluded patients with: no radicular pain symptoms before back surgery, lumbar canal stenosis, spondylolysis, more than one herniated disc, foraminal lumbar disc herniated, other bones disease and joint disease. Each patient did a CT scan or MRI of the lumbar spine.
Data Collection
We collected clinical and radiological data from medical records. We analyzed the radiologic data of the herniated disc fragment, the time to surgery. The indications of surgery was cauda equina syndrome, progressive motor weakness, intolerable symptoms. We reviewed the intraoperative complications. Surgical results were evaluated at 1 and 6 months postoperatively, using, in addition to the patient evaluation, indices for pain, activities of daily living and working capacity [8]. These results were graded with MacNab’s outcome assessment of patient satisfaction [9].
Data Analysis
Statistical analysis and data processing was performed with the software SPSS version 25. The association between presenting symptoms, time to surgery, patient gender, level of education with the outcomes were determined using the Chi2 test. Variables with a value of p<0.05 were considered statistically significant.
During the period, we did 135 spine surgical procedures. Thirteen patients were operated on from a GLDH. This patient population was composed of 9 men (69.2%) and four women (30.8%). Thus, the sex ratio was 2.25 :1.
The mean age of the patient population was 43.23±6.723 years (range 33-55).
Five patients (38.5%) had an elementary level, 5 (38.5%) a secondary level and 3 (23%) a high level of education.
Three patients (23.1%) were smokers in our study population and 7 (53.8%) had heavy labor.
Seven patients (53.8%; n = 7) presented with a cauda equina syndrome (Table 1).
Table 1: Clinical Presentation of Patients
| Parameters | n (%) |
| Bilateral hyperalgic radicular pain | 1 (7.7) |
| Right hyperalgic radicular symptoms | 2 (15.4) |
| Left radicular symptoms with a deficit | 3 (23.1) |
| Cauda equina syndrome | 7 (53.8) |
Table 2 shows that the anatomical location of a herniated disc was centrally in 8 patients (61.5%). The level of the GLDH was between L4-L5 in 69.2 % cases (n = 9) and L5-S1 in 30.8% (n = 4).
Table 2: Disc Location on MRI or CT Scan
| Location | n (%) |
| Right | 2 (15.4) |
| Left | 3 (23.1) |
| Central | 8 (61.5) |
The mean time to surgery after the development of pain was 14.46±10.055 months (range 3-36). Surgical treatment consisted of full laminectomy and discectomy for all the patients. We never did lumbar fusion. There was no complication during surgery. Evolution was graded as excellent in 76.9 % cases (n = 10) and good in 23.1% (n = 3). The postoperative outcomes were not influenced by clinical characteristics, sociodemographic and image findings (Table 3).
Table 3: Sociodemographic Data, Clinical Characteristics, Image Features and of the Patients
Parameters | Outcomes (n = 13) | p-value
| |
Excellent | Good | ||
| Profession | 0.612 | ||
| Heavy labor | 5 | 2 | - |
| without heavy | 5 | 1 | - |
| Education level | 0.289 | ||
| Primary | 3 | 2 | - |
| Secondary | 5 | 0 | - |
| University | 2 | 1 | - |
| Smokers | 0.631 | ||
| Yes | 2 | 1 | - |
| No | 8 | 2 | - |
| Symptoms | 0.660 | ||
| Bilateral hyperalgic radicular pain | 1 | 0 | - |
Right hyperalgic radicular symptoms | 1 | 1 | - |
Left radicular symptoms with a deficit | 2 | 1 | - |
| Cauda equina syndrome | 6 | 1 | - |
| Disc herniated level | 0.913 | ||
| L4L5 | 7 | 2 | - |
| L5S1 | 3 | 1 | - |
| Anatomic location of LDH | 0.473 | ||
| Right | 1 | 1 | - |
| Left | 2 | 1 | - |
| Central | 1 | 7 | - |
The definition of giant Lumbar Disc Herniation (GLDH) varies among different authors. It includes a herniation affecting more than 8mm, 33%, 40%, 50%, or 75% of the sagittal diameter of the spinal canal, or herniation causing complete spinal canal stenosis [3,10,11]. Our study defined GLDH as a herniated disc that affects more than 50% of the sagittal diameter of the spinal canal (Figure 1,2). Giant lumbar disc herniations are rare than more minor herniations [1]. Therefore, the incidence of GLDH in our study (4.3%) is inferior to the incidence in the literature: 8 to 22% [1,11-13].
The etiopathogenic mechanism of GLDH is unclear. However, heavy labor, traction, spinal manipulation and hypermobility conditions could predispose to that massive disc herniation [1]. In our series, 53.8% of patients did heavy labor.
Patients with GLDH usually have hyperalgic and bilateral radicular pain associated with neurological deficits [1]. Cauda equina syndrome is a frequent complication of GLDH. Halldin et al. described some cases of GLDH with significant compression without neurologic deficits [1,13].
Clinically, there is a risk of preoperatively permanent disability from neural compromise caused by the protrusion itself. Surgically, there are potential iatrogenic risks associated with the standard extradural microdiscectomy technique [2,7].
Surgical treatment is required when the outcome of strict conservative treatments is lacking or when symptoms are aggravated [10,14]. That surgical treatment consists of removal of the compressive lesion through an interlaminar approach. Alternatively, it could be removed by a laminectomy. Many techniques are described in the literature. They go from open microdiscectomy to percutaneous endoscopic discectomy, extradural or transdural discectomy [4,7,11,14-16].
In our series, 61.5% of GLDH had a central location. The management of that location can pose a significant challenge. According to Tulloch et al. [7], clinically, there is a risk of permanent disability from neural compromise caused by the compression itself. Moreover, there are potential iatrogenic risks associated with the standard extradural microdiscectomy. In these cases, transdural discectomy can be used [7]. We performed extradural discectomy in our study. We had no complications.
Lee et al. [11] and Akhaddar et al. [1], reported good surgery results. The goal of the surgery is to decrease pain by relieving the pressure on the nerve root. And, surgery with a well-performed technique on the right patient will often result in a good outcome [17]. In our study, 76.9% of patients had an excellent improvement to full recovery from their symptoms after surgery.
Some evidence factors as sociodemographic factors, including female gender, smoking, increased age, low socioeconomic status and low education level, could be predictors of poor outcomes after the surgery [17]. Some authors reported that the female gender is at risk of poor outcomes [8,18,19]. In our series, we did not find a gender influence in the outcomes. Follow-ups after surgery were worse in patients aged 40 and above [17]
Akhadar et al. [1], had 91.56% of good results after surgery for a population with a mean age of 41.66 ± 9.32 years old. In our study, patients are also young: mean age was 43.23±6.723 years old with good results (excellent in 76.9%). A higher level of education is predictive of a better outcome [20]. In our study, only three patients (23%) had a higher level of education. Smokers had minor leg pain relief after surgery [21].
Duration of pain or symptoms ≥12 months are statistically correlated with a less favorable outcome [22]. The symptoms’ duration in the Akhaddar et al. series was 7.8±5.77 months, with good global results. In our study, the results were good with 14.46±10.055 months of pain duration [1].
A larger disc curettage could explain the low recurrence after surgery for GLDH 1.95% for Akhaddar et al. [1]. Therefore, by using that technique, we had the same result in our study.
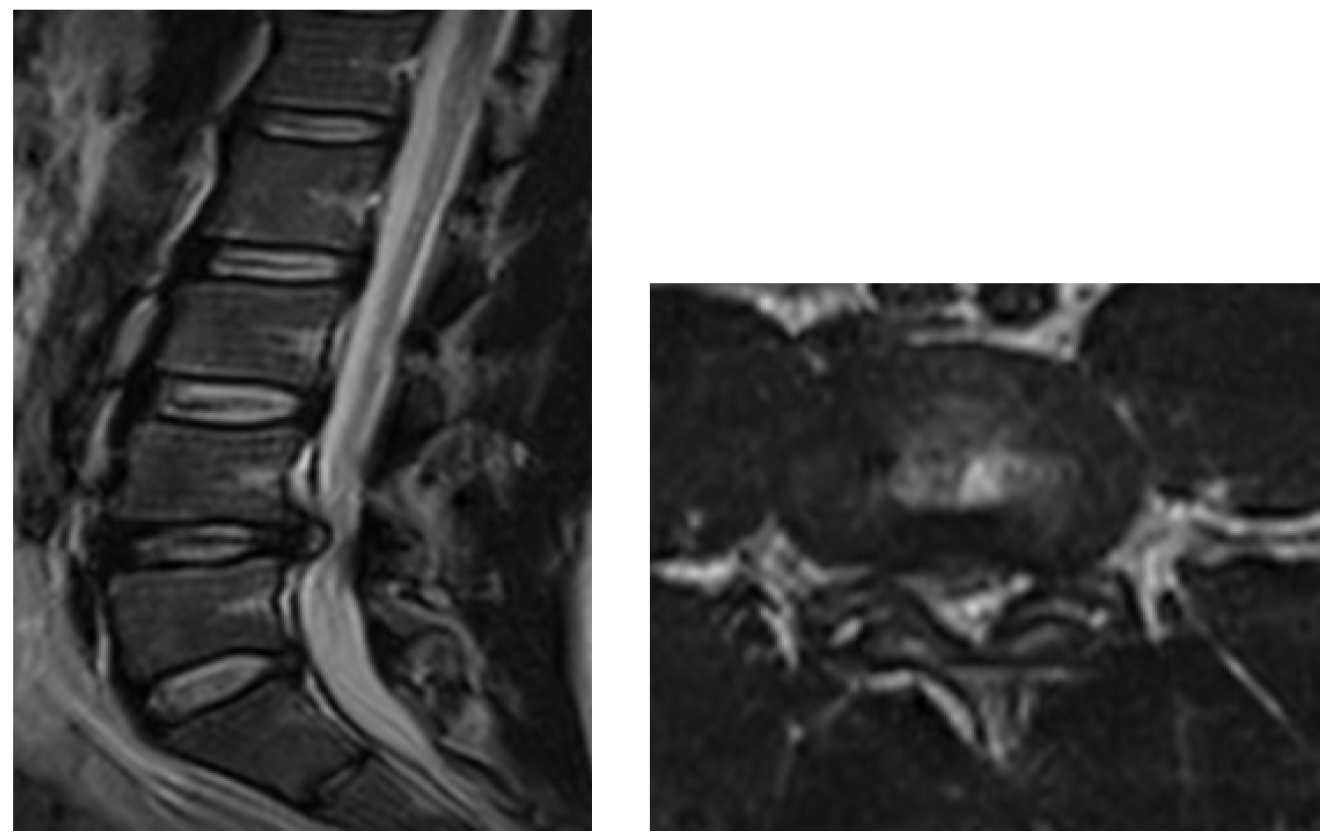
Figure 1: T2-WI Lumbar MRI. Sagittal (Left) and axial (Right) Showing Giant Central Lumbar Disc Herniation at L4L5 Level
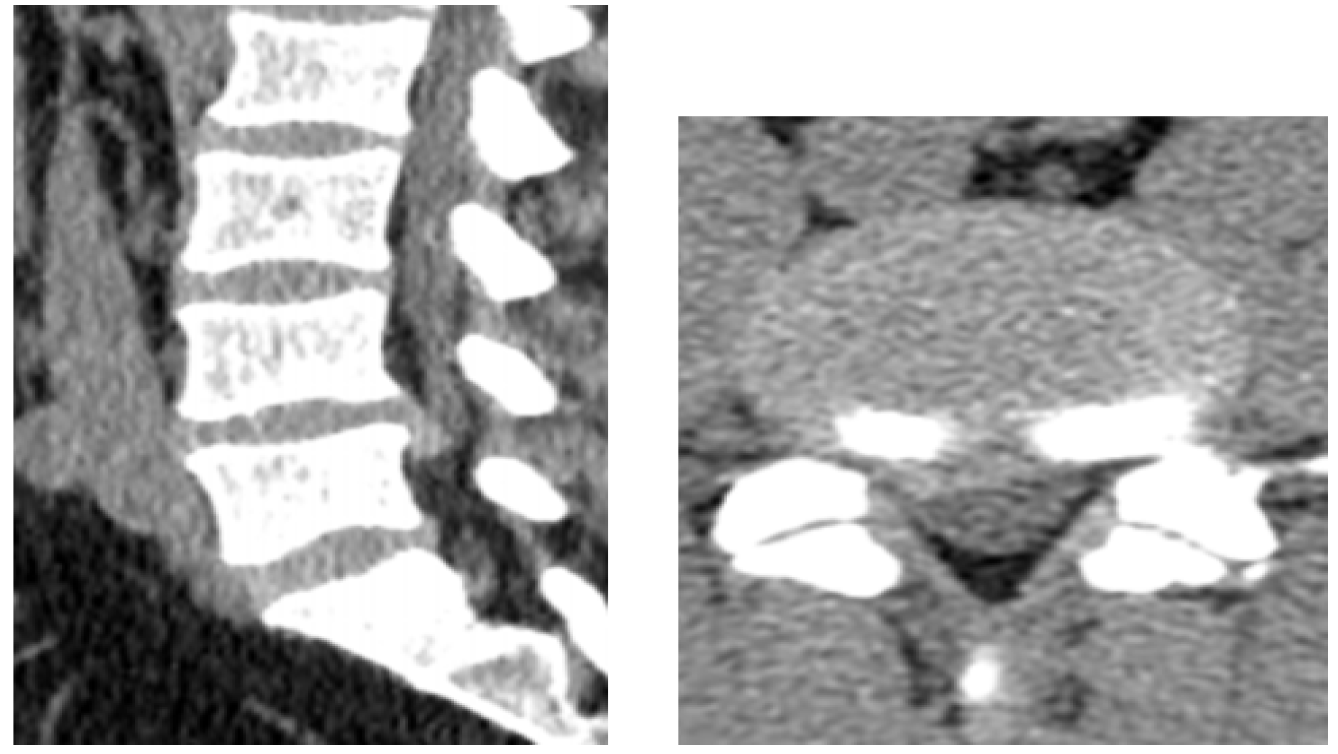
Figure 2: Sagittal (Left) and Axial (Right)CT Scan Showing a Giant Right Posterolateral Lumbar Disc Herniation at L4L5 Level Migrated Down
GLDH is a distinct entity compared with smaller herniations. Patients can develop cauda equina syndrome. Surgery has good results in our conditions.
Author’s Contributions
All authors contributed to this work: Agbéko Komlan Doléagbénou: collect information, data analyzing and writing of the manuscript, all the other authors corrected the manuscript and approve its final version.
Akhaddar, A. et al. “Surgical Management of Giant Lumbar Disc Herniation: Analysis of 154 Patients over a Decade.” Neurochirurgie, vol. 60, no. 5, 2014, pp. 244–248. https://doi.org/10.1016/j.neuchi.2014.02.012.
Benson, R. et al. “Conservatively Treated Massive Prolapsed Discs: A 7-Year Follow-Up.” Annals of the Royal College of Surgeons of England, vol. 92, no. 2, 2010, pp. 147–153. https://doi.org/10.1308/003588410X12518836438840.
Qureshi, A. and P. Sell. “Cauda Equina Syndrome Treated by Surgical Decompression: The Influence of Timing on Surgical Outcome.” European Spine Journal, vol. 16, no. 12, 2007, pp. 2143–2151. https://doi.org/10.1007/s00586-007-0491-y.
Molina-Martínez, R.P. et al. “Minimally Invasive Management for a Giant Lumbar Intervertebral Disc Herniation: A Case Report and Literature Review.” International Journal of Surgery Case Reports, vol. 81, 2021, article 105843. https://doi.org/10.1016/j.ijscr.2021.105843.
Cribb, G.L. et al. “Observations on the Natural History of Massive Lumbar Disc Herniation.” The Journal of Bone and Joint Surgery. British Volume, vol. 89-B, no. 6, 2007, pp. 782–784. https://doi.org/10.1302/0301-620X.89B6.18712.
Ma, Z.J. et al. “MRI Outcomes of Nonsurgical Treatment of Giant Lumbar Disc Herniation: A Prospective Clinical Study.” In Review, 2020. https://doi.org/10.21203/rs.3.rs-100153/v1.
Tulloch, I. and M. Papadopoulos. “Giant Central Lumbar Disc Herniations: A Case for the Transdural Approach.” Annals of the Royal College of Surgeons of England, vol. 100, no. 3, 2018, pp. e53–e56. https://doi.org/10.1308/rcsann.2017.0218.
Hurme, M. and H. Alaranta. “Factors Predicting the Result of Surgery for Lumbar Intervertebral Disc Herniation.” Spine, vol. 12, no. 9, 1987, pp. 933–938.
Macnab, I. “Pain and Disability in Degenerative Disc Disease.” Neurosurgery, vol. 20, suppl. 1, 1973, pp. 193–196. https://doi.org/10.1093/neurosurgery/20.CN_suppl_1.193.
Gao, X. et al. “Efficacy Analysis of Percutaneous Endoscopic Lumbar Discectomy Combined with PEEK Rods for Giant Lumbar Disc Herniation.” Pain Research & Management, vol. 2020, 2020, article 3401605. https://doi.org/10.1155/2020/3401605.
Lee, J.C. et al. “An Analysis of the Prognostic Factors Affecting the Clinical Outcomes of Conventional Lumbar Open Discectomy: Clinical and Radiological Prognostic Factors.” Asian Spine Journal, vol. 4, no. 1, 2010, pp. 23–31. https://doi.org/10.4184/asj.2010.4.1.23.
Davis, A. “Massive L5/S1 Disc Protrusion: Subtle CT Signs.” Australasian Radiology, vol. 45, no. 3, 2001, pp. 394–395. https://doi.org/10.1046/j.1440-1673.2001.0945c.x.
Halldin, K. et al. “Three-Dimensional Radiological Classification of Lumbar Disc Herniation in Relation to Surgical Outcome.” International Orthopaedics, vol. 33, no. 3, 2009, pp. 725–730. https://doi.org/10.1007/s00264-008-0519-x.
Blamoutier, A. “Surgical Discectomy for Lumbar Disc Herniation: Surgical Techniques.” Orthopaedics & Traumatology, Surgery & Research, vol. 99, suppl. 1, 2013, pp. S187–S196. https://doi.org/10.1016/j.otsr.2012.11.005.
Bai, X. et al. “Percutaneous Endoscopic Lumbar Discectomy Compared with Other Surgeries for Lumbar Disc Herniation.” Medicine, vol. 100, no. 9, 2021. https://doi.org/10.1097/MD.0000000000024747.
Clark, A.J. et al. “Tubular microdiscectomy: Techniques, complication avoidance and review of the literature.” Neurosurgical Focus, vol. 43, no. 2, 2017, pp. E7. https://doi.org/10.3171/2017.5.FOCUS17202
Aljawadi, A. et al. “Sciatica presentations and predictors of poor outcomes following surgical decompression of herniated lumbar discs: A review article.” Cureus, vol. 12, no. 11, n.d. https://doi.org/10.7759/cureus.11605
Graver, V. et al. “Seven-year clinical follow-up after lumbar disc surgery: Results and predictors of outcome.” British Journal of Neurosurgery, vol. 13, no. 2, 1999, pp. 178–184. https://doi.org/10.1080/02688699943952
Häkkinen, A. et al. “Changes in the total oswestry index and its ten items in females and males pre- and post-surgery for lumbar disc herniation: A 1-year follow-up.” European Spine Journal, vol. 16, no. 3, 2007, pp. 347–352. https://doi.org/10.1007/s00586-006-0187-8
Lequin, M.B. et al. “Surgery versus prolonged conservative treatment for sciatica: 5-Year results of a randomised controlled trial.” BMJ Open, vol. 3, no. 5, 2013, pp. e002534. https://doi.org/10.1136/bmjopen-2012-002534
Cobo Soriano, J. et al. “Predictors of outcome after decompressive lumbar surgery and instrumented posterolateral fusion.” European Spine Journal, vol. 19, no. 11, 2010, pp. 1841–1848. https://doi.org/10.1007/s00586-010-1284-2
Ng, L.C.L. and P. Sell. “Predictive value of the duration of sciatica for lumbar discectomy: A prospective cohort study.” The Journal of Bone and Joint Surgery. British Volume, vol. 86, no. 4, 2004, pp. 546–549.
