
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
Introduction: The most prevalent type of abdominal trauma in children is blunt abdominal trauma (BAT). Traffic accidents and falls are the most prevalent causes of trauma. In this case, a CT scan is the gold standard for detecting BAT. However, there are several limits to this examination, particularly in terms of availability, cost, and radiation exposure. In BAT, FAST assists in the detection of intraabdominal free fluid. Case Description: Three pediatric patients with stable hemodynamics underwent BAT in this case series. All three patients were below 17 years old and had stomach discomfort due to a traffic accident. All three patients tested positive for FAST. Then, a contrast CT scan of the abdomen revealed a splenic rupture in the three patients and a splenic rupture and liver rupture in one of them. All the patients were hemodynamically stable before being treated with symptomatic medicines in a conservative (non-surgical) manner. All of the patients had satisfactory outcomes and could return home without undergoing surgery. Conclusion: Both FAST and CT scans do not affect therapeutic care, that were conservative management in these patients with stable hemodynamics. As a result, FAST may be a less expensive examination alternative, reducing radiation exposure and lowering the risk of cancer in children in the future.
Trauma is the leading cause of death in children, in which every year, roughly 20 million children are harmed. More specifically, after head and chest trauma, abdominal trauma is the third highest cause of mortality in children. In this regard, blunt abdominal trauma accounts for 90% of abdominal trauma in children. Then, traffic accidents and falls are the most prevalent trauma mechanisms. In addition, the most prevalent reason for children being sent to the emergency room is acute abdominal injury, and it is a leading cause of death in children under the age of one year [1-2].
Management of blunt abdominal trauma cases in children with hemodynamically stable is conservative management. Therefore, the Focused Assessment with Sonography for Trauma (FAST) examination results are not necessary to change management. In addition, free fluid is not always present in cases of solid organ rupture, so a CT scan must be performed. Moreover, now is the era of “gentle imaging”, which reduces the examination using radiation exposure in children to reduce the risk associated with malignancy in the future. Thus, this case series discusses the role of FAST in assessing blunt abdominal trauma in hemodynamically stable children [4-6].
Case Series
In this case series, three pediatric patients had blunt abdominal trauma who were hemodynamically stable. The three patients were evaluated for age, injury mechanism, FAST examination, CT scan examination, Hb examination, and therapy management. The three patients were under 17 years old and registered through the emergency department at the General Hospital of Dr. Moewardi Surakarta in December 2019. Following a traffic accident, all of these patients complained of abdominal pain. All three patients tested positive for FAST. Then, a contrast CT scan of the abdomen revealed a splenic rupture in the three patients and a splenic rupture and liver rupture in one of them. All of the patients were hemodynamically stable before being treated with symptomatic medicines in a conservative (non-surgical) manner. Furthermore, all of the patients had positive outcomes and could return home without undergoing surgery.
Case 1
Child A, female, aged 12 years old. Twelve hours before admission to the hospital, when the patient was riding a motorcycle wearing a standard helmet, the patient had an accident colliding with another motorcycle from the opposite direction. The patient fell with her stomach hitting the road. After the incident, the patient was conscious, and the patient then complained of pain in the left side of the abdomen, headache (+), nausea (-), and vomiting (-). The rescuer took the patient to Ungaran General Hospital. The patient was infused, injected with painkillers, and treated for wounds. The family took the patient to Dr. Moewardi General Hospital Surakarta. The patient arrived at the emergency room six hours after the incident, and the pain was felt in the left abdomen. From the primary survey examination, the airway was still free with normal breathing, RR 20 x/m, no circulatory disturbances, BP 110/70 mmHg, HR 98 x/min with GCS E4V5M6, isochor pupil (3mm/3mm), pupillary light reflex (+/+), lateralization (-/-), and a temperature of 36.8 degrees Celsius. In the secondary survey, injuries were found in the left hypochondria region, no open wounds, no abdominal distension, bowel movements (+), and pain when palpated in the left upper quadrant of the abdomen. In stable hemodynamic conditions, the FAST examination was performed, and FAST (+) was obtained in Morrison's pouch and splenorenal (Figure 1).
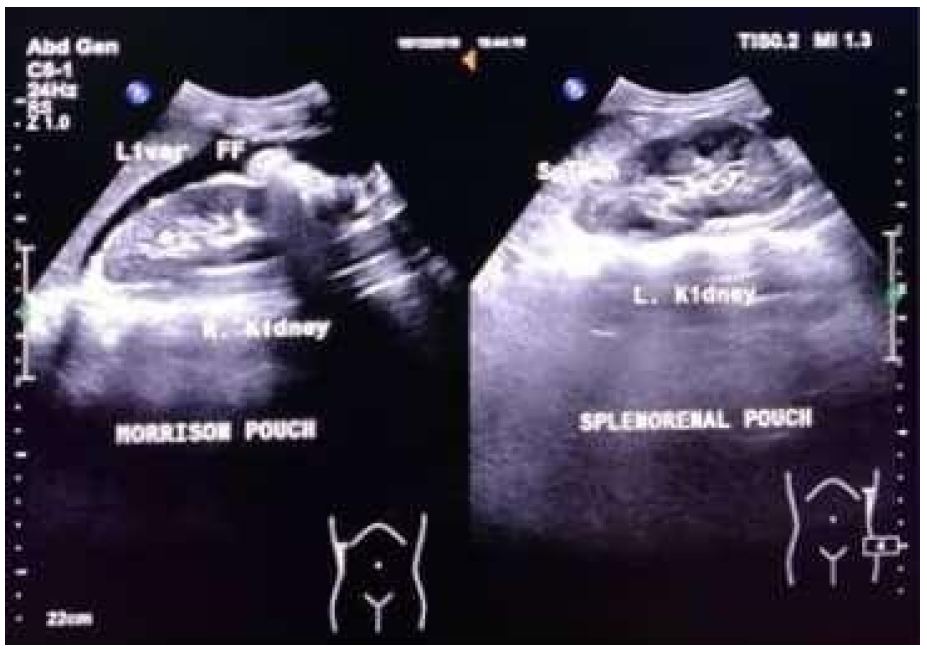
Figure 1: FAST Examination (+) on the Morrison Pouch and Splenorenal Pouch
Then, the patient was sent to radiology for abdominal CT examination. The results showed grade IV Spleen Injury (AAST rating scale) and free fluid in the abdominal cavity (Hematoperitoneum) (Figure 2).
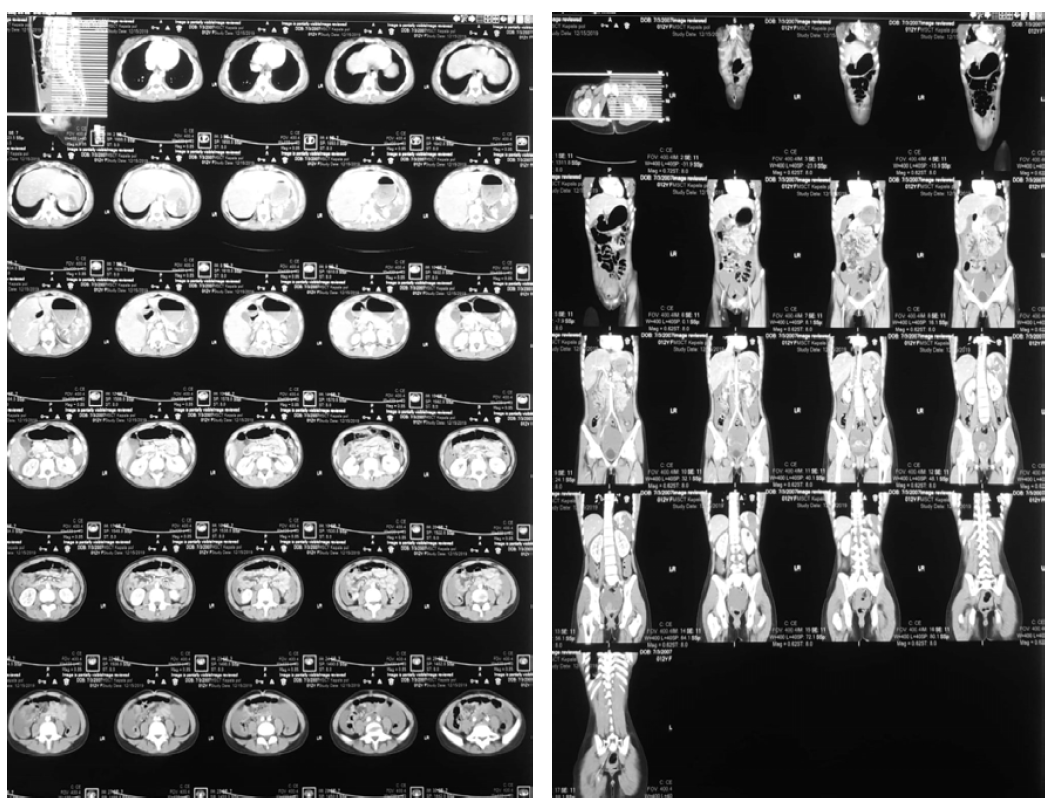
Figure 2: Spleen Rupture Grade 4 (AAST Grading Scale), Free Fluid in the Abdominal Cavity (hematoperitoneum)
After that, the patient's blood was taken to be checked for hemoglobin (Hb) levels, and serial Hb examinations were performed; Hb decreased to less than 10 periodically (Tables 1 and 2).
Table 1: Decrease in Hemoglobin After the Incident
15/12/2019 | 13.00 | 15.00 | 17.00 |
Hemoglobin (mg/dl) | 8.8 | 8.4 | 7.6 |
Table 2: Hemoglobin Levels on Days II-IV After the Incident
No | Date | Hemoglobin (mg/dl) |
1 | 15/12/2019 | 7.6 |
2 | 16/12/2019 | 9.0 |
3 | 17/12/2019 | 10.4 |
4 | 18/12/2019 | 10.6 |
In this case, the patient showed FAST (+) in the Morison Pouch and minimal (+) in the Splenorenal Pouch. The FAST ultrasound results were then followed by a contrast CT scan of the abdomen, and spleen rupture grade IV and free intra-abdominal fluid were obtained. In this case, the result (+) in the Morison Pouch was not accompanied by liver rupture.
Therapeutic management in this patient started from the emergency room. The patient received NaCl 0.9% infusion of 1500 cc/24 hours and symptomatic injection therapy, with an injection of Metamizole 1 gr/8 hours as a pain reliever and an injection of Ranitidine 50 mg/12 hours as an injection anti-nausea. The patient also received a transfusion of 2 kolf PRC when the patient's Hb dropped to 7.6. Then, it was continued with Asering 20ml/kg loading in 20 minutes and then treatment with D5 ½ NS 78 cc/hour. Injections of antibiotics were with Ampicillin sulbactam 50 mg kg/6 hours or 1 gram IV bolus/6 hours and injection of Paracetamol 15 mg/kg/6 hours or 500 mg/6 hours. The patient had a total of four days of total rest. After three days, the hemoglobin began to rise and returned to normal values on the fourth day. The patient's general condition improved, and the patient was finally able to go home on the fifth day.
Case 2
Child B, male, aged 17 years old. Ten hours before admission to the hospital, while the patient was riding a motorcycle wearing a standard helmet, the patient had an accident colliding with a car from the opposite direction. The patient fell with his stomach hitting the handlebars and the road. After the incident, the patient was conscious, and the patient then complained of pain in the right and left abdominal areas, headache (-), nausea (-), and vomiting (-). The rescuer took the patient to Widodo General Hospital, Ngawi. The patient was infused, injected with painkillers, and treated for wounds. The patient was then taken to Dr. Moewardi General Hospital, Surakarta, by the family. The patient arrived at the emergency room eight hours after the incident, and pain in the abdomen was felt in the right and left abdomen. From the primary survey examination, the airway was still free with normal breathing, RR 22 x/m, no circulation disturbance found, BP 100/60 mmHg, HR 104 x/min with GCS E4V5M6, isochor pupil (3mm/3mm), pupillary light reflex (+/+), lateralization (-/-), and a temperature of 36.4 degrees Celsius. In the secondary survey, injuries were found in the right hypochondria and left lumbar regions, no open wounds, no abdominal distension, bowel movements (+), and pain when palpated in the left upper quadrant of the abdomen. Then, hemodynamically stable, a FAST examination was performed. FAST (+) was obtained in Morrison pouch, splenorenal, and perivesical (Figure 3).
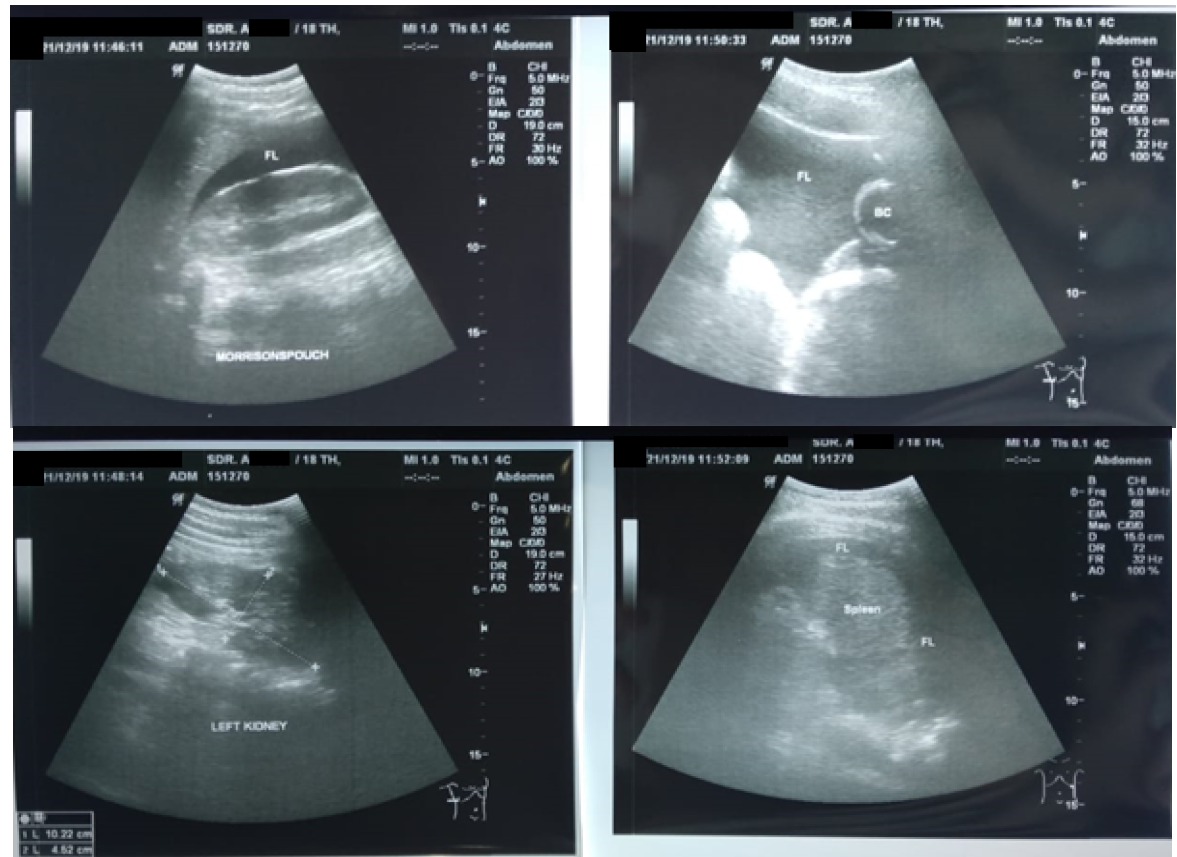
Figure 3: FAST Examination (+) on the Morrison Pouch, Splenorenal, and Perivesical
Then, the patient was sent to radiology for abdominal CT examination, with results showing spleen injury grade V (AAST rating scale) and free fluid in the abdominal cavity (Hematoperitoneum) (Figure 4).

Figure 4. Spleen Rupture Grade 5 (AAST Grading Scale), Free Fluid in the Abdominal Cavity (Hematoperitoneum)
The patient's blood was then taken to be checked for Hb levels, and serial Hb examinations were performed; Hb decreased to less than 10 periodically (Tables 3 and 4).
Table 3: Decrease in Hemoglobin on Day 1 After the Incident
19/12/2019 | 10.00 | 12.00 | 14.00 |
Hemoglobin (mg/dl) | 9.0 | 8.4 | 8.4 |
Table 4: Hemoglobin Levels on Days II-IV After the Incident
| No | Date | Hemoglobin (mg/dl) |
| 1 | 19/12/2019 | 8.4 |
| 2 | 20/12/2019 | 9.2 |
| 3 | 21/12/2019 | 10.1 |
| 4 | 22/12/2019 | 10.4 |
In this case, the patient showed FAST (+) results in Morison Pouch, splenorenal, and perivesical. The FAST ultrasound results were then followed by a contrast CT scan of the abdomen and revealed a spleen rupture grade V and free intra-abdominal fluid. In this case, the results (+) in the Morison pouch and perivesical were not accompanied by rupture of the liver and rupture of the bladder.
Therapeutic management in this patient started from the emergency room, with the patient receiving 0.9% NaCl infusion of 1500 cc/24 hours. The patient also received symptomatic injection therapy, with an injection of Metamizole 1 g/8 hours as a pain reliever and Ranitidine 50 mg/12 hours as an anti-nausea. In addition, the patient received a transfusion of 2 kolf PRC when the patient's Hb dropped to 8.4. Then, it was followed up with Asering 20ml/kg in 20 minutes and then treatment with D5 ½ NS 84 cc/hour. The antibiotic injections were Ampicillin sulbactam 50 mg/kg/6 hours or 1 gram IV bolus/6 hours and Paracetamol injection 15 mg/kg/6 hours or 500 mg/6 hours. Furthermore, the patient had a total of four days of rest. After three days, the hemoglobin began to rise and returned to normal values on the fourth day. The patient's general condition improved, and the patient was finally able to go home on the fifth day.
Case 3
Child C, female, aged 16 years old. Eight hours before admission to the hospital, while the patient was riding a motorcycle wearing a standard helmet, the patient had an accidental fall while avoiding a pothole in the road. The patient fell with her stomach hitting the motorcycle handlebar. After the incident, the patient was conscious, and the patient then complained of pain in the right and left abdominal areas, headache (-), nausea (-), and vomiting (-). The rescuer took the patient to Karanganyar General Hospital. The patient was infused, injected with painkillers, and treated for wounds. The family took the patient to Dr. Moewardi General Hospital Surakarta. The patient arrived at the emergency room two hours after the incident, and abdominal pain was felt in the right and left abdomen. From the primary survey examination, the airway was still free with normal breathing, RR 18 x/m, no circulatory disturbances, BP 90/60 mmHg, HR 84 x/min with GCS E4V5M6, isochor pupil (3mm/3mm), pupillary light reflex (+ /+), lateralization (-/-), and a temperature of 36.5 degrees Celsius. In the secondary survey, the injury was found in the right hypochondria region, with no open wounds, no abdominal distension, bowel movements (+), and pain on palpation in the right upper quadrant of the abdomen. Then, a FAST examination was performed with stable hemodynamics, and FAST (+) was obtained in the Morrison pouch and splenorenal pouch (Figure 5).
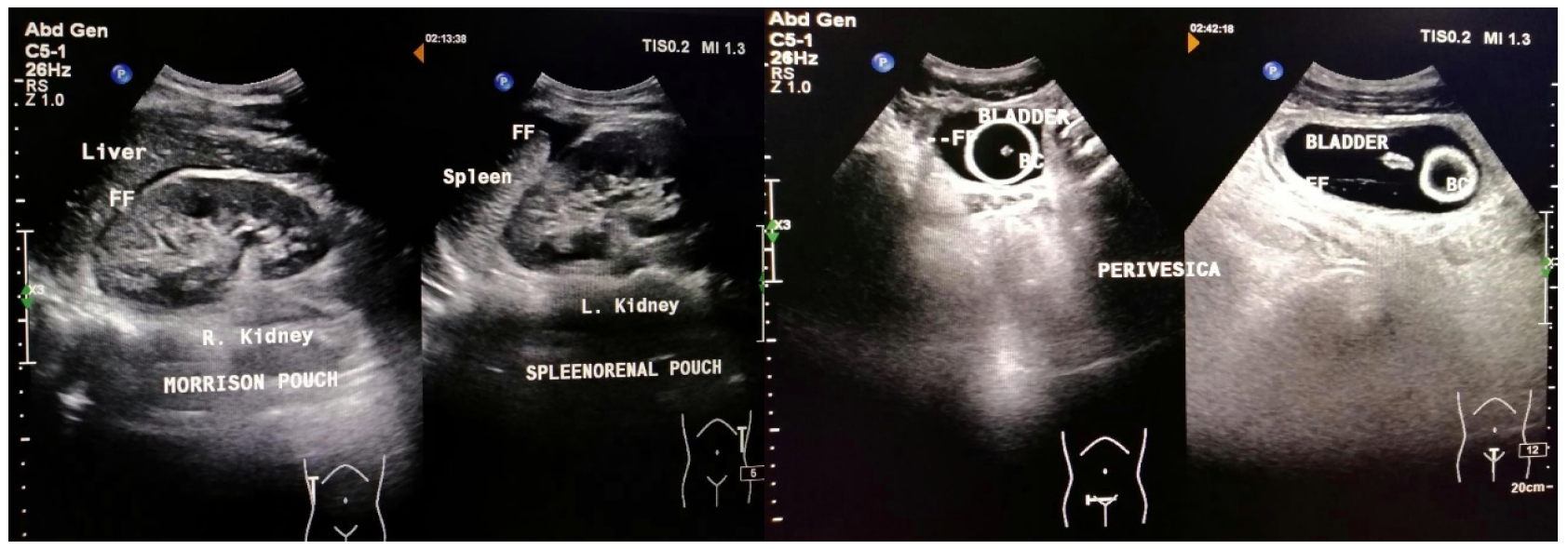
Figure 5: FAST Examination (+) on the Morrison Pouch and Splenorenal Pouch
Later, the patient was sent to radiology for abdominal CT examination, and the results showed liver rupture grade IV and splenic rupture grade II (AAST rating scale), with free fluid in the abdominal cavity (Hematoperitoneum) (Figure 6).
Figure 6: Liver Rupture Grade IV and Splenic Rupture Grade II (AAST Rating Scale), Free Fluid in the Abdominal Cavity
The patient's blood was then taken to be checked for hemoglobin (Hb) levels, and serial Hb examinations were performed; Hb decreased to less than 10 periodically (Tables 5 and 6).
Table 5: Decrease in Hemoglobin at Day 1 After the Incident
16/12/2019 | 14.00 | 16.00 | 18.00 |
Hemoglobin (mg/dl) | 8.8 | 8.4 | 8.0 |
Table 6: Hemoglobin Levels on Days II-IV After the Incident
No | Date | Hemoglobin (mg/dl) |
1 | 16/12/2019 | 8.0 |
2 | 17/12/2019 | 9.2 |
3 | 18/12/2019 | 10.4 |
4 | 19/12/2019 | 10.4 |
In this case, the patient showed FAST (+) results in the Morison pouch and Splenorenal pouch. The FAST ultrasound results were then followed by a contrast CT scan of the abdomen and obtained liver rupture grade IV, splenic rupture grade II, and free intra-abdominal fluid. In this case, the (+) result in Morison pouch was accompanied by liver rupture grade IV, while the (+) result in Splenorenal was accompanied by splenic rupture grade II.
Therapeutic management in this patient began in the emergency room. The patient received an infusion of 0.9% NaCl from 1500 cc/24 hours and symptomatic injection therapy, with an injection of Metamizole 1 gr/8 hour as a pain reliever and Ranitidine 50 mg/12 hours as an anti-nausea. The patient also received a transfusion of 2 kolf PRC when the patient's Hb dropped to 8.0. Then, it was followed up with Asering 20ml/kg in 20 minutes and then treatment with D5 ½ NS 80 cc/hour. Antibiotic injections were Ampicillin sulbactam 50 mg/kg/6 hours or 1 gram IV bolus/6 hours and Paracetamol injection 15 mg/kg/6 hours or 500 mg/6 hours. In total, the patient had a total rest for four days. After three days, the hemoglobin began to rise and returned to normal values on the fourth day. The patient's general condition improved, and the patient was finally able to go home on the fifth day.
Of the three cases, all the above blunt abdominal trauma incidents were caused by traffic accidents. It is consistent with several studies stating that the most common trauma mechanism in blunt abdominal trauma is traffic accidents. Incidents of blunt abdominal trauma with high velocity often cause damage to multiple organs, such as solid organs, liver, spleen, or kidney, compared to hollow organs. Some literature even stated that the organ most commonly affected is the spleen, about 40-55% of cases. It is because the spleen is the most fragile organ. The number of cases in the liver is 35-45%, and the small intestine is 5-10%. Meanwhile, the incidence of blunt abdominal trauma to the kidney is about 80-90%, usually accompanied by severe trauma with injury to other organs [7,8].
Moreover, the therapeutic management of the three cases was in the form of conservative or non-surgical management. Conservative management or without surgery is the standard management of abdominal solid organ rupture in children with hemodynamically stable according to APSA guidelines. The 96% of ruptures that occur are managed without surgery. In these cases, all had a splenic rupture, and the first option is conservative management. Here, close patient observation and aggressive fluid resuscitation dictate conservative therapy. On the other hand, if there is continuing bleeding and the demand for resuscitation blood transfusions surpassing 40 mL/kg, splenectomy is required [9].
In addition, a contrast CT scan is the best method for evaluating solid organ rupture so that the location and extent of the rupture can be known. Accordingly, there is a grading scale for liver, spleen, and kidney injuries, ranging from subcapsular hematoma to overall organ impairment. The grading scale for splenic and liver ruptures is in accordance with the American Association for Surgery of Trauma, as shown in Table 7. Moreover, classification of injury severity remains an essential aspect of non-operative management. However, in ruptured spleen and liver in children with hemodynamically stable, conservative management is the first choice. In these three cases, splenic ruptures grade II, grade IV, and grade V were found, while in one of the cases, it was accompanied by liver rupture grade IV [11-13].
In some studies, for all cases of intra-abdominal organ rupture, FAST's sensitivity (28%) was low, but its specificity was high (91%). Similar findings have also been seen in many studies in children. When evaluating patients with intra-abdominal organ rupture requiring urgent intervention, the FAST examination’s sensitivity is increased (44%), with high specificity (89%). In this case, i.e., hemodynamically stable, both FAST and CT scan did not change therapy management, namely still with conservative management [11-13].
FAST can be used for early detection of blunt abdominal trauma in children and at the same time to determine whether a CT scan of the abdomen is necessary. In this regard, the degree of rupture in hemodynamically stable conditions does not change the therapeutic management, i.e., still conservative management. Hence, FAST may be a less expensive examination alternative, reducing radiation exposure and lowering the risk of cancer in children in the future.
Karam, O. “National survey on abdominal trauma practices of pediatric surgeons.” European Journal of Pediatric Surgery, vol. 20, no. 5, 2010, pp. 334–338.
Gaines, B. A. and H. R. Ford. “Abdominal and pelvic trauma in children.” Critical Care Medicine, vol. 30, no. 11, suppl., 2002, pp. S416–S423.
Van Schuppen, J. et al. “Diagnostic accuracy of a step-up imaging strategy in pediatric patients with blunt abdominal trauma.” European Journal of Radiology, vol. 83, no. 1, 2014, pp. 206–211.
Menaker, J. et al. “Use of the focused assessment with sonography for trauma (FAST) examination and its impact on abdominal computed tomography use in hemodynamically stable children with blunt torso trauma.” Journal of Trauma and Acute Care Surgery, vol. 77, no. 3, September 2014, pp. 427–432.
Tummers, W. et al. “Role of focused assessment with sonography for trauma as a screening tool for blunt abdominal trauma in young children after high energy trauma.” South African Journal of Surgery, vol. 54, no. 2, 2016.
Miglioretti, D. L. et al. “The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk.” JAMA Pediatrics, vol. 167, no. 8, 2013, pp. 700–707.
Sjamsuhidajat and W. de Jong. Buku Ajar Ilmu Bedah. 3rd ed., EGC, 2011.
Mattox, K. L. et al. Trauma. 7th ed., McGraw-Hill, 2013.
Notrica, D. M. “Pediatric Blunt Abdominal Trauma: Current Management.” Current Opinion in Critical Care, vol. 21, 2015, pp. 531–537.
Carter, J. W. et al. “Do we really rely on FAST for decision-making in the management of blunt abdominal trauma?” Injury, vol. 46, no. 5, May 2015, pp. 817–821.
Scaife, E. R. et al. “The role of focused abdominal sonography for trauma (FAST) in pediatric trauma evaluation.” Journal of Pediatric Surgery, vol. 48, no. 6, June 2013, pp. 1377–1383.
Brunicardi, F. C. et al. Schwartz’s Principles of Surgery. 8th ed., McGraw-Hill Education, 2004, pp. 141–142.
McVay, M. R. et al. “Throwing out the ‘grade’ book: Management of isolated spleen and liver injury based on hemodynamic status.” Journal of Pediatric Surgery, vol. 43, no. 6, June 2008, pp. 1072–1076.
