
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
Lower extremity complications in diabetes patients are extremely common worldwide and the most common one to occur is ulcer in the foot though other complications also occur frequently like abscess, gangrene, cellulitis, etc. With the increasing incidence of diabetes worldwide, there is an increased incidence of these complications in different parts of the world. Most of these complications are preventable. The author had recently introduced 2 terminologies namely the diabetic foot delay and diabetic foot push, which are aimed at decreasing the complications in diabetic foot. This article provides a brief discussion on diabetic foot push.
Diabetes mellitus is a metabolic disease with multi-organ involvement whose incidence is increasing worldwide [1-3]. It is predicted that people with diabetes mellitus will increase from 463 million in 2019 to around 700 million by year 2045 [1].
Of all the complications in diabetes, the most common complications are lower limb problems of which foot ulcers tops the list [4]. The annual incidence of diabetic foot ulcers is around 2.2% [3]. The issue with diabetic foot ulcer is that it can lead to limb loss [5]. It is observed that infection can occur in up to 58% of patients having a new foot ulcer [3]. This can lead to increase in hospitalization, amputation and death [6]. Interestingly, most of the foot complications are preventable. It is observed that good knowledge and practices on diabetic foot can reduce the risk of diabetic foot complications and amputation [7]. As a part of preventive strategy, the author had introduced 2 new terms’ namely, “Diabetic foot Delay” and “Diabetic Foot Push” [8].
Diabetic Foot Push
The term “Diabetic foot Push” was recently introduced by Amit Jain from India [8]. Diabetic foot push is prolonging the time interval from high-risk foot to development of any complications in foot like abscess, gangrene, ulceration, etc. (Figure 1).
Diabetes patients are considered to have a high-risk foot if they have peripheral neuropathy, peripheral arterial disease, previous ulceration, foot deformities or an amputation [4, 5].
The diabetic foot push can be primary or secondary. Primary diabetic foot push should be instituted in those patients who have peripheral neuropathy or underlying ischemia but never developed foot complications like ulcer, abscess, etc.
Secondary diabetic foot push should be instituted in those patients who have already suffered a complication in the past for which they were treated like previous ulcers or amputation.
A primary diabetic foot push is always better than a secondary diabetic foot push because once a complication like ulcer has occurred or an amputation has taken place, the chances of recurrences are high. Overall outcomes are better in primary diabetic foot push strategies.
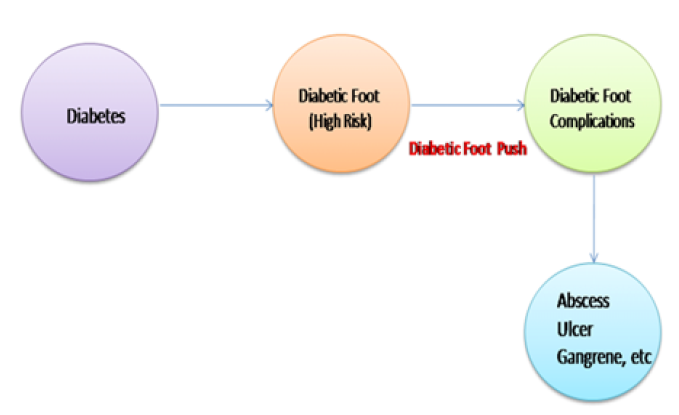
Figure 1: Showing the Diabetic Foot Push
Preventative Strategies
If patient is considered to have high risk feet, then there should be an intense effort, both from patient and the healthcare provider, to ensure that the diabetic foot complication does not happen or it should be postponed as much as possible [8]. Some of the recommended strategies for diabetic foot push are listed in Table 1.
Regular screening and ensuring proper footwear are 2 most important strategies a health care provider like diabetic foot specialist should focus to ensure a good diabetic foot push. A study has shown that more than 66% of patients had poor footwear that may predispose to ulceration [4]. There are also numerous studies that show screening being omitted by health care professionals [9].
Amit Jain’s screening tool, also known as Amit Jain’s triple assessment/Amit Jain’s linear foot test [9] and Amit Jain’s footwear ladder approach [10] are 2 good methods that can employed to achieve diabetic foot push. Amit Jain’s type 1 therapeutic foot wears [11, 12] should be the minimum type of footwear to be used for high-risk foot patient with other types to be used based on foot status.
Table 1: Showing the Suggested Strategies for Diabetic Foot Push
Primary Diabetic Foot Push | Secondary Diabetic Foot Push |
Frequency of screening / evaluation should be once in 3 to 6 months | Frequency of screening/evaluation should be quarterly
|
Type of footwear- usually Type 1 therapeutic footwear suffices | Type 1, 2 or 3 therapeutic footwear based on foot status |
At least weekly inspection of feet by patient or attender’s | Daily inspection to once in 2 to 3 days
|
Can continue walking for 30 to 45 minutes in protective footwear
| Restricted ambulation to avoid repetitive stress on scar or stump. Alternative exercise like swimming, yoga, etc. suggested that does not involve much pressure on foot. |
Patient education | Patient education |
Strict diabetes control | Strict diabetes control |
Diabetes and diabetic foot are growing menace worldwide and are known to cause increased morbidity and mortality. Diabetic foot can result in amputation that can lead to misery. Most of the complications especially foot ulcers are recurrent in nature. The best treatment is to prevent them. Diabetic foot push is the new term introduced by author that aims at prolonging the interval of development of complications. One can use various preventive strategies like screening, education, use of therapeutic footwear, etc for achieving a good push.
Turkmen, A. et al. “Research of knowledge and attitudes of patients with diabetic foot ulcer regarding foot care.” International Journal of Diabetes and Clinical Research, vol. 8, 2021, pp. 144.
Jinadasa, C.V.M. and M. Jeewantha. “A study to determine the knowledge and practice of foot care in patients with chronic diabetic ulcers.” International Journal of Collaborative Research on Internal Medicine and Public Health, vol. 3, 2011, pp. 115–122.
Del Core, M.A. et al. “The evaluation and treatment of diabetic foot ulcers and diabetic foot infections.” Foot and Ankle Orthopedics, 2018, pp. 1–11.
Aziz, K.M.A. “Association between high-risk foot, Retinopathy and HbA1c in Saudi Diabetic Population.” Pakistan Journal of Physiology, vol. 6, no. 2, 2010, pp. 22–28.
Lavery, L.A. et al. “Practical criteria for screening patients at high risk for diabetic foot ulceration.” Archives of Internal Medicine, vol. 158, 1998, pp. 157–162.
Lazzarini, P.A. et al. “The Queensland high risk foot form (QHREF): Is it a reliable and valid clinical research tool for foot disease?” Journal of Foot and Ankle Research, vol. 7, 2014, pp. 7.
Pourkazemi, A. et al. “Diabetic foot care: Knowledge and practice.” BMC Endocrine Disorders, vol. 20, 2020, pp. 40.
Jain, A.K.C. “Diabetic foot delay and diabetic foot push.” IAR Journal of Medical Sciences, vol. 2, no. 2, 2021, pp. 102–103.
Jain, A.K.C, and H.C. Apoorva. “Predictive validity of amit jain’s screening tool in estimating the risk of complications in diabetic foot: A retrospective cohort study.” Wound International, vol. 11, no. 4, 2020, pp. 31–37.
Jain, A.K.C. and H.C. Apoorva. “Footwear problems in developing countries: A practical approach.” The Diabetic Foot Journal, vol. 24, no. 1, 2021, pp. 20–25.
Jain, A.K.C. “Triangle of therapeutic footwear.” SAR Journal of Medicine, vol. 1, no. 2, 2020, pp. 31–33.
Jain, A.K.C. and H.C. Apoorva. “Auditing the usage of therapeutic footwear in diabetic foot patients through amit jain’s extended ‘SCC’ classification for therapeutic footwear.” Medicine Science, vol. 9, 2020, pp. 437–442.
