
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
Background: The present study was done to compare the Quality of life in patients of chronic pelvic pain after pulsed radiofrequency ablation versus thermal radiofrequency ablation of Ganglion Impar. Material and Methods: The present study was prospective, randomized, single blinded study and was based on series of 30 patients presenting with chronic pelvic pain, having already failed conservative medical management, presenting in Pain clinic if IGMC Shimla. The patients were divided into 2 groups of 15 patients. Patients in Group A(n = 15) were given thermal radiofrequency ablation whereas patients in Group B were given pulsed radiofrequency ablation. Results: Mean 24 Hours Post Procedural American Chronic Pain Association Quality of Life Scale Score (ACP) of the patients in Group A was 6.20±0.414 whereas mean 24 Hours Post Procedural ACP Score in patients of group B was 7.07±0.704. (p = 0.000). The mean 1 week Post Procedural ACP Score of the patients in Group A was 6.00±0.000 whereas mean 1 week Post Procedural ACP Score in patients of group B was 6.73±0.704. (p = 0.000). Mean 2 week Post Procedural ACP Score of the patients in Group A was 5.53±0.516 whereas mean 2 week Post Procedural ACP Score in patients of group B was 6.47±0.743. (p = 0.000). Mean 3 week Post Procedural ACP Score of the patients in Group A was 5.20±0.414 whereas mean 3 week Post Procedural ACP Score in patients of group B was 6.27±0.458. (p = 0.000) Conclusion: Present study showed that mean Post Procedural ACP Score (24 Hours, 1,2 and 3 week) was significantly lower in group A as compared to group B. we can conclude that thermal radiofrequency ablation of ganglion impar for chronic pelvic pain produces Quality of Life and Functional Capacity in the patients as compared to patients who were treated with pulsed radio frequency ablation.
Chronic pelvic pain (CPP) is a poorly localized pain due to damage of tissue or nerve from inflammation which worsens with odd sitting posture such as leaning back while being seated, prolonged sitting as well as standing, and abrupt rising from sitting position. The management of CPP involves a multimodal approach with key goal directed towards maximal achievable functional restoration and significant reduction in severity and intensity of pain [1,2]. Although it is imperative but trial of medical and behavioural therapy is to be given but it is seen that the interventional block technique such as Ganglion Impar block has shown superior patient’s satisfaction and improves patient’s quality of life [3,4]. Radiofrequency ablation is a minimally invasive method for destroying nerve fibres that convey pain signals to the brain. Ganglion Impar radiofrequency ablation (RFA) is a well-established, drug-free treatment that has been clinically demonstrated to give safe, effective, and long-lasting pain relief. Radiofrequency current has two significant advantages over low frequency AC or DC pulses in that it does not directly activate nerves or heart muscle, allowing it to be employed without general anaesthetic in many cases. Under the stimulating needle, both TRF (thermal radiofrequency ablation) and PRF (pulsed radiofrequency ablation) treatments cause distance-dependent tissue damage. Even in normothermia settings, the acute effects of PRF are more reversible and less neurodestructive than those of TRF, hence PRF is preferable to TRF. PRF produces a transient inhibition of evoked synaptic activity and classic thermal RF (TRF) produces a lasting inhibition [5,6].
The purpose of this study is to present that patients with chronic pelvic pain that did not improve with medications but could be controlled after giving Ganglion Impar block using radiofrequency ablation. While viewing medical literature the studies of ganglion impar block were done using steroids, local anaesthestic, neurolytics and radiofrequency ablation , but we could find very few studies which compared the Quality of life of Thermal versus Pulsed radiofrequency ablation in Ganglion Impar block for treatment of chronic pelvic pain in female patients hence we decided to pursue this study of comparison of Quality of life in pulsed versus thermal radiofrequency ablation among patients of chronic pelvic pain.
Aims and Objectives
To compare the Quality of life in patients of chronic pelvic pain after pulsed radiofrequency ablation versus thermal radiofrequency ablation of Ganglion Impar.
After obtaining approval from the Institutional ethics committee, CTRI registration number CRTI/2020/10/028306 and written informed consent of the patients, the proposed study was carried out in adult female patients of age groups 18-60 years, visiting the pain clinic for chronic pelvic pain, who had already taken medications for 2 weeks but inadequate benefit was reported by medications and physiotherapy trial.
Source of Data
This study was conducted on patients with chronic pelvic pain at IGMC and associated hospital KNSH for M and Ch Shimla with the approval of research and Ethics Committee.
Study Design
This study was randomized, single blinded prospective and controlled study.
Inclusion Criteria
Patient giving consent to participate in the study
Female patients with chronic pelvic pain after ruling out any obstetrics and gyanecological cause through specialist opinion and USG or negative diagnostic laproscopy
Patients above the age of 18 years and below 60 years
Patients who have had atleast two weeks trial of medications without significant effect
Patient with normal anatomy for ganglion impar block
Exclusion Criteria
Patient refusal
Patients with uncontrolled systemic diseases
Patients with infection or injury at the injection site
Patients with coccygectomy
Allergy to iodine contrast medium
Hypersensitivity
Patient with bleeding disorders and the patients on anticoagulants
A total of 30 patients from pain clinic who were suffering from chronic pelvic pain were included after obtaining written consent.
Sample Size Calculation
The sample size was calculated to be of 15 subjects for each group; this was calculated on the basis of a similar study in chronic pelvic pain patients where the minimum number of patients required were found to be 31, with a power of at least 80% and α of 0.05. Anticipating loss of subjects during the study, we enrolled 30 patients in our study, 15 in each group.
The patients were divided into 2 groups of 15 patients each using computer generated random numbers.
Group A (Group –Thermal RFA) patients were treated with thermal radiofrequency ablation.
Group B (Group – Pulsed RFA) patients were treated with pulsed radiofrequency ablation.
The study was randomized, single blinded prospective and controlled study with follow up done weekly for three weeks either by routine checkup in the pain clinic or through a phone call. They underwent radiofrequency ablation of Ganglion Impar by trans-sacro-coccygeal technique using C-arm guidance.
Patients were made familiar with American Chronic Pain Association Quality of Life Scale. The ganglion impar block was administered in all these patients under all aseptic precautions using C-arm guidance to mark and identify bony landmarks.
Methodology
All patients underwent a routine preanaesthetic checkup. During this, thorough history, general examination, routine investigations of the patients i.e. FBS/RBS, bleeding time (BT), clotting time (CT) of the patient was carried out. Quality of life was assessed using American Chronic Pain Association Quality of Life scale.
After confirmation of inclusion criteria of the patient by the anesthesiologist the procedure was undertaken. Written informed consent was taken from the patient prior to the procedure explaining the various risks and benefits of the procedure. A 20-gauge venous access was secured and basic monitors such as noninvasive blood pressure, and saturation (SpO2) probe will be connected.
The procedure was carried out with the patient in prone position with pillow under the abdomen to allow flexion of the lumbosacral spine and the lower extrimities rotated internally.
The procedure was performed using C-arm to identify and mark the essential bony landmarks. Under strict aseptic precautions the saccrococcygeal and gluteal regions were cleaned with savlon and painted with povidone iodine 10%. The area was drapped with sterile towels, and the access region was left open. A skin wheal was raised with 1% lidocaine using 25-gauge needle after the identification of the disc in lateral projection. A true lateral image was obtained by superimposing the two greater sciatic notches.
22G, 5 cm long with 5mm active tip radiofrequency needle was then introduced from the marked site to pierce the saccrococcygeal joint and position was confirmed after injecting non-ionic dye and needle placement was confirmed by induction of reverse comma sign/ “crescent” sign in lateral fluroscopic views. A diagnostic block was performed using 1% lidocaine 10ml.
After 5 min, patient was ressessed and if the patient considers pain relief of atleast 2-point reduction in VAS scores, the patients were considered candidates for radiofrequency ablation of Ganglion Impar.
Before radiofrequency ablation was performed, tissue impedence check and motor and sensory tests were done. These comprised tissue impedence <600 Ohm, sensory response <50 Hz and motor response < 2 Hz at stimulation intensity between 0.4 – 0.8 volts. Patients with no significant decrease in VAS score were excluded from this study.
Thereafter radiofrequency ablation was done depending upon the group:
Group A: Thermal radiofrequency ablation, was done using radiofrequency thermocouple electrode (Cosman Medical Co Inc.) connected to Cosman radiofrequency generator using following parameters: tissue impedance <600 Ohm, sensory response <50 Hz, and a motor response <2 Hz at a stimulation intensity between 0.4–0.8 volts (V) with 3 cycles each 90 seconds apart and temperature ranging from 60 -80°C
Group B: Pulsed radiofrequency ablation, was done using radiofrequency thermocouple electrode using the following parameters: voltage output 45 V, 2 Hz frequency, 20 ms pulses in a one-second cycle, 120 second duration per cycle, impedance range between 150 and 500 Ohms with 3 cycles and a 42°C plateau temperature Inj bupivacaine 5ml and inj dexamethasone 2 mg was injected the end of procedure to overcome ablation induced pain and neuritis. Follow up was done after the procedure using American Chronic Pain Association Quality of Life Scale
Patients were kept in the recovery room for 2 hours and then sent home with the attendents on the day of the procedure with routine single dose antibiotic prophylaxis, NSAIDS in the form of Tablet Diclofenac 100mg SR for 3 days. Patients were advised to abstain from heavy workload after the procedure. Patient who complained of increase in VAS in between the follow up period were given tablet Pregablin 75 mg H.S. at night as rescue drug. Complains / side effects like parasthesias and numbness were noted.
Follow-up after 24 hours,1 week, 2 weeks and 3 weeks was done either in OPD or telephonically and Quality of Life score were noted.
Failure cases: Patients who did not achieve a successful block, that is patients in whom there is no decrease in VAS by 2 points after 24 hours of block were dropped from further study; but the number was noted as failure cases and other form of treatment was given.
American Chronic Pain Association Quality of Life Scale
0 (Non-Functioning)- Stay in bed all day. Feel hopeless and helpless about life
1 Stay in bed atleast half the day. Have no contact with outside world
2 Get out of bed but don't get dressed. Stay in home all day
3- Get dressed in the morning. Minimal activities at home. Contact with friends via phone, email
4 Do simple chores around the house. Minimal activities outside of home two days a week
5 Struggle but fulfil daily home responsibilities. No outside activity. Not able to work/ volunteer
6 Work/Volunteer limited hours. Take part in limited social activities on weekends
7 Work/ Volunteer for a few hours daily. Can be active atleast 5 hours a day. Can make plans to do simple activities on weekends
8 Work/ Volunteer for atleast 6 hours daily. Have energy to make plans for one evening social activity during the week. Active on weekends
9 Work/ Volunteer/ be active 8 hours daily. Take part in family life. Outside social activities limited
10 (Normal Quality of Life)- Go to work/ volunteer each day. Normal daily activities each day. Have a social life outside of work
Data Analysis
All the data collected from the patient’s records was transferred into MS Excel sheet for further processing and analysis. Data was further analyzed using standard statistical software. In order to compare results between two study groups, appropriate parametric or non-parametric test of statistical significance was used. Probability value (p-value) less than 0.05 was considered statistically significant.
The present study was conducted in prospective, single blind, randomized controlled manner in the Pain Clinic in the Department of Anesthesiology at Indira Gandhi Medical College and Hospital. It comprised of total 30 female patients between age group 30- 60 years. Patients were randomly divided into two groups. Patients in Group A (n = 15) were given thermal radiofrequency ablation whereas patients in Group B were given pulsed radiofrequency ablation. No patients experienced any interventional failure (inability to obtain proper fluoroscopic view of dye). So, in each group 15 patients were studied.
Demographic Analysis
According to age distribution, in group A, 3(20%) were≤ 40 years, 6(40%) were between 41-50 years and 6(40%) were between 51-60 years of age while in group B, 8(53.3%) were≤ 40 years, 4(26.7%) were between 41-50 years and 3(20%) were between 51-60 years of age. The p value was calculated to be 0.159 which was found to statistically non-significant. (Figure 1)
Mean age (in years) in group A and B was found to be 47.60±6.833 and 42.67±7.807 years respectively. The p value was calculated to be 0.76 which was found to be statistically non-significant.
American Chronic Pain Association Quality of Life Scale (ACPAQOL)
Pre -procedural ACPAQOL Score: The mean Pre-procedural ACPAQOL score of the patients in Group A was 6.87±0.743 whereas mean Pre-procedure ACPAQOL score in patients of group B was 7.17±0.741. The p value was 0.063 which was statistically non-significant (Table 1).
24 Hours Post Procedural ACPAQOL Score
The mean 24 Hours Post Procedural ACPAQOL Score of the patients in Group A was 6.20±0.414 whereas mean 24
Hours Post Procedural ACPAQOL Score in patients of group B was 7.07±0.704. The p value was 0.000 which was statistically significant. This showed that mean 24 Hours Post Procedural ACPAQOL Score was significantly lower in group A as compared to group B (Table 2).
1 week Post Procedural ACPAQOL Score
The mean 1 week Post Procedural ACPAQOL Score of the patients in Group A was 6.00±0.000 whereas mean 1 week Post Procedural ACPAQOL Score in patients of group B was 6.73±0.704. The p value was 0.000 which was statistically significant. This showed that mean 1 week Post Procedural ACPAQOL Score was significantly lower in group A as compared to group B (Table 3).
2 Week Post Procedural ACPAQOL Score
The mean 2 week Post Procedural ACPAQOL Score of the patients in Group A was 5.53±0.516 whereas mean 2 week Post Procedural ACPAQOL Score in patients of group B was 6.47±0.743. The p value was 0.000 which was statistically significant. This showed that mean 2 weeks Post Procedural ACPAQOL Score was significantly lower in group A as compared to group B (Table 4).
3 Week Post Procedural ACPAQOL Score
The mean 3 week Post Procedural ACPAQOL Score of the patients in Group A was 5.20±0.414 whereas mean 3 week Post Procedural ACPAQOL Score in patients of group B was 6.27±0.458. The P value was 0.000 which was statistically significant. This showed that mean 3 weeks Post Procedural ACPAQOL Score was significantly lower in group A as compared to group B (Table 5).
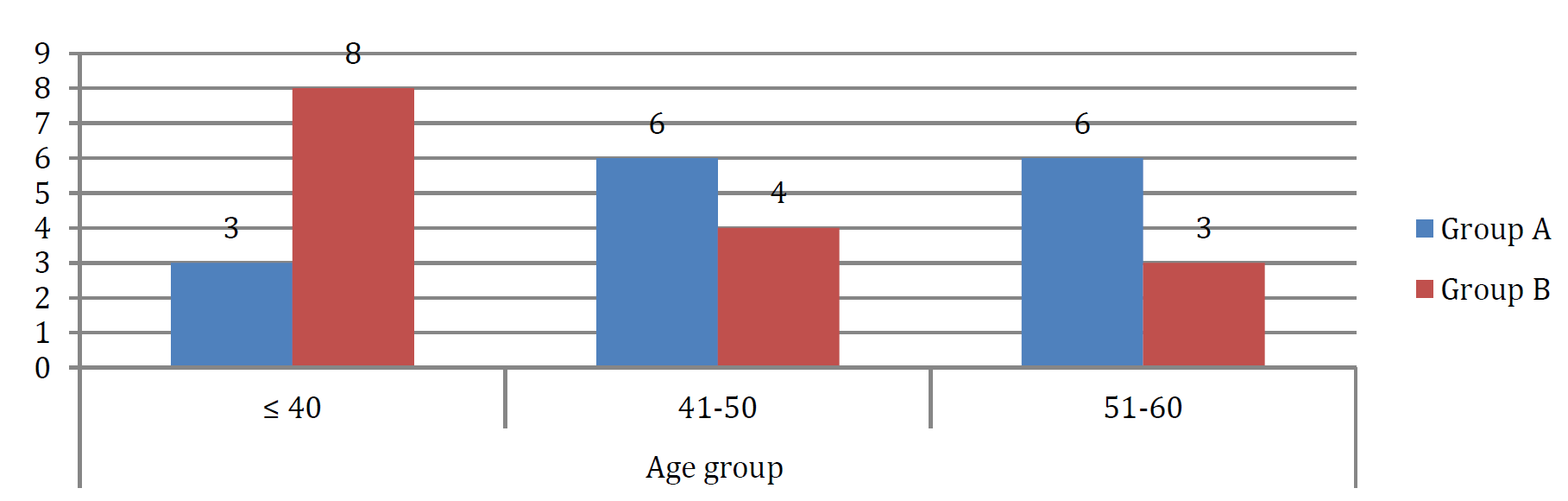
Figure 1: Age Wise Distribution of the Patients
Table1: Comparison of Pre Procedural ACPAQOL Score
| Parameter | Group A | Group B | ||
Mean | SD | Mean | SD | |
Pre-procedural ACPAQOL Score | 6.87 | 0.743 | 7.17 | 0.741 |
T-Statistics | -2.211 | |||
p-value | 0.063 | |||
Table 2: Comparison of 24 Hours Post Procedural ACPAQOL Score
| Parameter | Group A | Group B | ||
| Mean | SD | Mean | SD | |
| 24 Hours Post Procedural ACPAQOL Score | 6.20 | 0.414 | 7.07 | 0.704 |
| T-Statistics | -4.111 | |||
| p-value | 0.000 | |||
Table 3: Comparison of 1 Week Post Procedural ACPAQOL Score
| Parameter | Group A | Group B | ||
| Mean | SD | Mean | SD | |
| 1 week Post Procedural ACPAQOL Score | 6.00 | 0.000 | 6.73 | 0.704 |
| T-Statistics | -4.036 | |||
| p-value | 0.000 | |||
Table 4: Comparison of 2 week Post Procedural ACPAQOL Score
| Parameter | Group A | Group B | ||
| Mean | SD | Mean | SD | |
| 2 weeks Post Procedural ACPAQOL Score | 5.53 | 0.516 | 6.47 | 0.743 |
| T-Statistics | -3.994 | |||
| p-value | 0.000 | |||
Table 5: Comparison of 3 week Post Procedural ACPAQOL Score
| Parameter | Group A | Group B | ||
| Mean | SD | Mean | SD | |
| 3 weeks Post Procedural ACPAQOL Score | 5.20 | 0.414 | 6.27 | 0.458 |
| T-Statistics | -6.693 | |||
| p-value | 0.000 | |||
Chronic pelvic pain is a common problem with higher incidence in female and has high degree of functional and emotional impairment. This sympathetically mediated pelvic pain pain is poorly localized type of pain with a burning quality and a sense of urgency in the perineal region. The initiating factor in neuropathic pain is mainly damage to the tissue caused by either inflammation or nerve damage. Radiofrequency ablation of Ganglion Impar has demonstrated long term effectiveness in reducing the number of analgesics consumed by the patient on daily basis.
We conducted a prospective single blinded randomized control study with a calculated sample size of 30 with history of pelvic pain where we compared thermal radiofrequency ablation versus pulsed radiofrequency ablation. No literature is available with similar study design using the above-mentioned techniques. We observed satistically significant difference in the pain assessment parameters during immediate and follow up period. Thermal radiofrequency ablation was found to be better as compared to pulsed radiofrequency ablation in management of immediate and chronic pelvic pain. The patients were followed for a period of 3 weeks.
Chronic pevic pain is associated with significant physical and emotional impairment especially in females. In our study we incorporated assessment and comparison of this aspect using American Chronic Pain Association Quality of Life Scale. Pre procedural Mean consequtive values of ACPAQLS for thermal and pulsed RFA were 6.87 and 7.17 which were comparable clinically non-significant p value- 0.06. The values after 3 weeks follow up were 5.2 and 6.2 respectively for both groups and difference was found to be clinically significant p value < 0.05. Various other studies have also included this parameter in their study. Demicray et al. [7] evaluated quality of life scale using EQ-5D questionnaire which dercribed 5 domains i.e. mobility, self-care, usual activities, pain/ discomfort and anxiety/depression. Mean pre procedural EQ-5D score was 4.4, 7.5 in 1st month, 6.6 in 6th month follow up period.
Gonnade et al. [8] in their study used Oswestry Disability Index (ODI) to measure the degree of disability and estimate the quality of life with low back pain and observed the baseline value of 48.97 and values of 18.65, 21.84, 26.16 respectively at 4, 12 and 24 weeks. The difference was found to be satistically significant with p value <0.001. They further assessed that preventive measures and exercises should be advised to avoid any recurrence in pain. Blockade of the ganglion impar is an effectual pain-relieving procedure for management of chronic pelvic pain. Usmani et al. [9] conducted a similar study and found that ganglion impar block by conventional radiofrequency ablation provided a significantly better quality of pain with no major side effects as compared with pulsed radiofrequency ablation.
Limitation
Our study was limited by the limited amount of research that has been conducted in this field. Very few studies have been conducted which described Ganglion Impar using radiofrequency ablation for chronic pelvic pain. We found no study which compared thermal radiofrequency versus pulsed radiofrequency ablation of Ganglion Impar in patients with chronic pelvic pain. The sample size was low in our study due to the Covid pandemic which affected many patients. Above all our study was dependent on referral of patients from other departments who did not respond to conservative management. Lack of general awareness of pain clinic and procedures and undertreatment of the symptoms also contribute to poor patient compliance.
Based on the findings, we can infer that thermal radiofrequency ablation of ganglion impar for persistent pelvic pain resulted in better quality of life and functional capacity in patients than pulsed radiofrequency ablation. Patients with chronic pelvic discomfort may benefit from ganglion impar thermal radio frequency ablation. However, more research with a larger sample size and a longer and more thorough follow-up is required.
Wallace, M.S. et al. “Malignant pain.” Textbook of Regional Anesthesia, edited by P.P. Raj, Churchill Livingstone Publishers, 2002, pp. 585.
Maigne, J.Y. et al. “Comparison of three manual coccydynia treatments: A pilot study.” Spine, vol. 26, no. 20, October 2001, pp. E479–E483.
Fitzgerald, M.P. et al. “Randomized multicenter feasibility trial of myofascial physical therapy for the treatment of urological chronic pelvic pain syndromes.” Journal of Urology, vol. 189, no. 1 Suppl., January 2013, pp. S75–S85.
Gunduz, O.H. et al. “Pain Relief due to transsacrococcygeal ganglion impar block in chronic coccygodynia: A pilot study.” Pain Medicine, vol. 16, 2015, pp. 1278–1281.
Usta, B. et al. “Fluoroscopically guided ganglion impar block by pulsed radiofrequency for relieving coccydynia.” Pain Practice, vol. 39, 2010, pp. E1–E2.
Bonica, J.J. “The management of pain of cancer.” Journal of the Michigan State Medical Society, vol. 52, no. 3, March 1953, pp. 284–290.
Demircay, E. et al. “Radiofrequency thermocoagulation of ganglion impar in the management of coccydynia: preliminary results.” Turkish Neurosurgery, vol. 20, 2010, pp. 328–333.
Gonnade, N. et al. “Ganglion impar block in patients with chronic coccydynia.” Indian Journal of Radiology and Imaging, vol. 27, no. 3, July–September 2017, pp. 324–328.
Usmani, H. et al. “Conventional radiofrequency thermocoagulation vs pulsed radiofrequency neuromodulation of ganglion impar in chronic perineal pain of nononcological origin.” Pain Medicine, vol. 19, no. 12, December 2018, pp. 2348–2356.
