
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
AVMs are abnormalities of the intracranial vessels that constitute a connection between the arterial and venous systems and lack an intervening capillary bed. Hemorrhagic presentation of AVM is associated with significant morbidity and mortality; it is an independent predictor of future hemorrhage. AVM rupture is one of the most frequent and important causes of hemorrhagic stroke during pregnancy and puerperium. Whether the risk of AVM rupture increases during pregnancy and puerperium is controversial, but maternal physiological changes in hemodynamics, blood volume, and hormonal effects on the vessel walls could potentially increase the risk of hemorrhage from AVMs during pregnancy and in the postpartum period. For AVM during pregnancy and puerperium, previous studies have demonstrated histologic changes in arteries and arterioles of pregnant women, thought to be mediated by progesterone. The changes included fragmentation of reticular fibers and loss of normal corrugation of elastic fibers, which might play a role in the increased risk for AVM hemorrhage during pregnancy. However, there is insufficient evidence to guide management decisions for ruptured AVMs during pregnancy, and further well-designed, multicenter, perspective clinical trials are needed. We report the case of a young woman, who had an emergency ceasarean surgery for a headeck and consciousness disorder witch evoked eclampsia, while in fact, she had a rupture of arteriovenous malformation following the rupture of a cerebral Arterio-venous malformation in cerebral imaging.
AVMs are abnormalities of the intracranial vessels that constitute a connection between the arterial and venous systems and lack an intervening capillary bed. There are significant morbidity and mortality associated to hemorrhagic presentation of AVM [1]. According to some reports, 0.1% of the general population harbors an AVM [2, 3].
We report the case of a young woman, who had an emergency ceasarean surgery for a headeck and consciousness disorder witch evoked eclampsia, while in fact, she had a rupture of arteriovenous malformation following the rupture of a cerebral Arterio-venous malformation in cerebral imaging.
Observation
Ms. NEZHA C, 19 years old, with no notable pathological history, was referred from a private clinic for the management of spontaneous intracerebral hematoma, which occurred during the third trimester of her first pregnancy. Her symptomatology began with the installation of intense brutal headaches with left deficit and obnibulation state. The initial diagnosis was eclampsia, with fetal caesarean extraction as a therapeutic consequence under general anesthesia. Because of the absence of patient awakening, a cerebral CT scan was performed, and objectified a right fronto parietal hematoma (Figure 1).
Patient transferred to our structure, a cerebral angioscanner was performed that showed an arterioveinus malformation Figure 2, then an endovascular treatment was performed.
The evolution was favorable, marked by a recovery of a normal neurological state but persistence of a left hemiparesie. The patient returned home with anticonvulsant therapy and kinesitherapy sessions 18 days after.
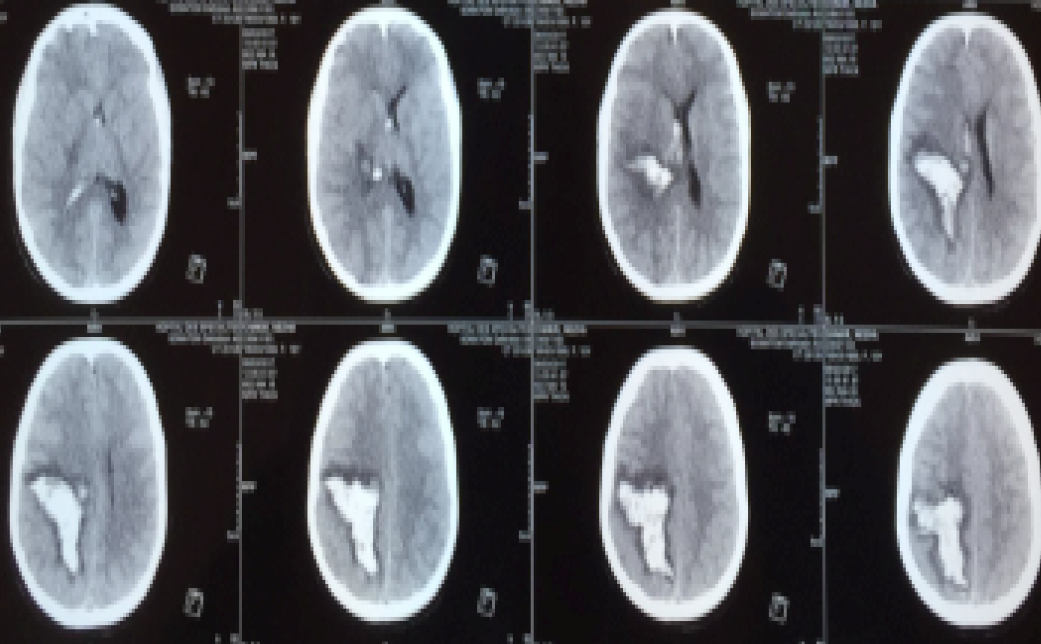
Figure 1: Cerebral CT Scan Showing a Right Parietal Fronto Hematoma
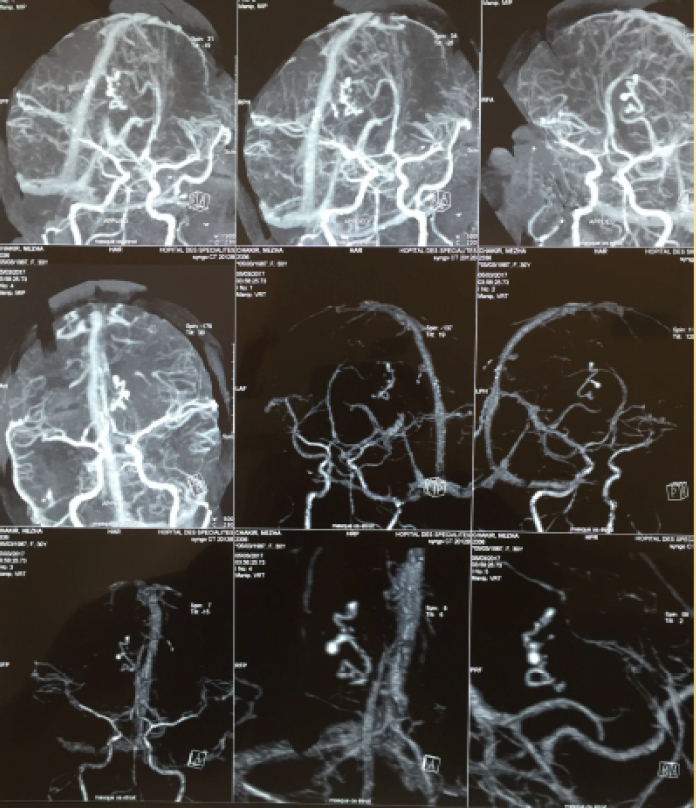
Figure 2: Cerebral Angiography Showing an Arteriovenous Malformation
AVMs are abnormalities of the intracranial vessels that constitute a connection between the arterial and venous systems and lack an intervening capillary bed. Hemorrhagic presentation of AVM is associated with significant morbidity and mortality; it is an independent predictor of future hemorrhage [1].
According to reports, 0.1% of the population harbors an AVM [2, 3]. Both sexes are affected equally. AVMs are the leading cause of nontraumatic intracerebral hemorrhage in people less than 35 years old [4]. Most lesions reach attention in patients in their 40's and 75% of the hemorrhagic presentations occur before the age of 50 years [2].
AVM rupture is one of the most frequent and important causes of hemorrhagic stroke during pregnancy and puerperium. Whether the risk of AVM rupture increases during pregnancy and puerperium is controversial, but maternal physiological changes in hemodynamics, blood volume, and hormonal effects on the vessel walls could potentially increase the risk of hemorrhage from AVMs during pregnancy and in the postpartum period [5]. A meta-analysis by Gross and Du revealed that the rate of hemorrhage was 2.2% for unruptured AVMs and 4.5% for ruptured AVMs [6].
Differing reports on rupture risk of AVM during pregnancy and puerperium may be related to different reasons, such as research methods, sample size, or outcome measures. Most, but not all, studies suggest that there is an increased risk of AVM rupture during pregnancy and puerperium [7].
It is generally recognized that there is a relationship between angioarchitecture and ruptured cerebral AVM. Besides the location of AVM, the characteristics of feeding arteries and number and deepness of draining veins are also considered risk factors for rupture. For AVM during pregnancy and puerperium, previous studies have demonstrated histologic changes in arteries and arterioles of pregnant women, thought to be mediated by progesterone; the changes included fragmentation of reticular fibers and loss of normal corrugation of elastic fibers, which might play a role in the increased risk for AVM hemorrhage during pregnancy [7].
Pregnant women presenting with signs and symptoms suggestive of intracranial hemorrhage require timely diagnosis. Digital subtraction angiography is the gold standard method for diagnosing cerebral AVM [7-8].
The diagnosis of eclampsia should not be delaying us from doing cerebral imaging. In case of rupture of an Arteriovenous malformation during a pregnancy, Piotin et al [9] suggest to give priority to the maternal prognosis, this may eventually lead to termination of pregnancy or fetal extraction depending on the term.
Maternal management for pregnant patients with a ruptured AVM should be mainly based on neurosurgical indications to save maternal life, especially in cases with severe neurological deteriorations.
However, in cases with mild neurological symptoms, treatment strategies should be considered that can save both mother and fetus. Moreover, when the fetus is immature, elective treatment might be selected until the fetus matures. Therefore, the management for ruptured AVMs during pregnancy has not been consistent, because of the consideration not only of the mother, but also of the fetus. Furthermore, the degree of surgical invasion, X-ray exposure, and influence of embolic materials and medical drugs on the fetus must be considered [5].
However, there is insufficient evidence to guide management decisions for ruptured AVMs during pregnancy, and further well-designed, multicenter, perspective clinical trials are needed [7].
Hemorrhagic presentation of AVM is associated with significant morbidity and mortality. The therapeutic management of a brain AVM discovered during pregnancy requires a multidisciplinary approach. It will take into account the neurological status of the parturient, the term of pregnancy and the feasibility of different therapeutic techniques (endovascular treatment or surgery). This case should give us a real warning, about precoce realization of cerebral imaging in front of neurological symptomatology especially for pregnant woman, because eclamsia is not the only risk, and an AVM isn't that rare.
Ajiboye, N. et al. “Cerebral Arteriovenous Malformations: Evaluation and management.” The Scientific World Journal, vol. 2014, 2014.
Brown, R.D. Jr. et al. “Frequency of intracranial hemorrhage as a presenting symptom and subtype analysis: A population-based study of intracranial vascular malformations in Olmsted County, Minnesota.” Journal of Neurosurgery, vol. 85, no. 1, 1996, pp. 29–32, https://doi.org/10.3171/jns.1996.85.1.0029.
Arteriovenous Malformation Study Group. “Arteriovenous malformations of the brain in adults.” The New England Journal of Medicine, vol. 340, no. 23, 1999, pp. 1812–1818.
Ruíz-Sandoval, J.L. et al. “Intracerebral hemorrhage in young people: Analysis of risk factors, location, causes, and prognosis.” Stroke, vol. 30, no. 3, 1999, pp. 537–541, https://doi.org/10.1161/01.STR.30.3.537.
Michiwaki, Y. et al. “Ruptured cerebral arteriovenous malformation during fifth pregnancy: A case report and literature review.” World Neurosurgery, 2019.
Gross, B.A. and R.Du. “Natural history of cerebral arteriovenous malformations: A meta-analysis.” Journal of Neurosurgery, vol. 118, 2013, pp. 437–443.
Zhu, D. et al. “Rupture risk of cerebral arteriovenous malformations during pregnancy and puerperium: A single-center experience and pooled data analysis.” World Neurosurgery, vol. 111, 2018, pp. e308–e315.
Porras, J.L. et al. “Hemorrhage risk of brain arteriovenous malformations during pregnancy and puerperium in a north american cohort.” Stroke, vol. 48, 2017, pp. 1507–1513.
Piotin, M. et al. “Cerebral arteriovenous malformations and pregnancy: Management of a dilemma.” Journal of Neuroradiology, vol. 31, no. 5, 2004, pp. 376–378.
