
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3239
ISSN (Online) : 2709-3220
Background: Nipple-sparing mastectomies (NSMs) are a relatively new method of conservatism in the treatment of breast cancer. Most of the breast skin is left intact during NSM, creating a pocket that can be filled with an implant or an autologous graft for a rapid reconstruction that yields an excellent cosmetic outcome. Combining prosthetic-based breast restoration with autologous flaps, such the latissimus dorsi (LD) flap, may be necessary to achieve symmetry. Case Description : A 45 year old woman who developed a breast deformity following a mastectomy for breast cancer. The Latissimus dorsi (LD) flap was chosen because it is a thin layer flap with good vascularization. The Latissimus dorsi (LD) flap, on the other hand, necessitates a different skin incision than the mastectomy. An inframammary adipofascial flap has been used as an autologous flap in conjunction with prosthetic-based breast reconstruction subsequent to nipple-sparing mastectomy (NSM). In this instance, the Latissimus dorsi muscle flap was employed in the axillary and breast regions. The Latissimus dorsi (LD) flap was deemed suitable as it can provide extensive coverage without any delay in the transfer procedure. Anatomically, this flap and its vascular supply are quite consistent. The arterial supply is provided by the thoraco-dorsal artery which provides a large branch to the serratus anterior muscle and provides a cutaneous branch. Successful management of the infection, postoperative partial weight bearing, and restricted range of motion in the affected breast was anticipated. Conclusion: The latissimus dorsi flap is a safe choice for skin regeneration after a nipple sparing mastectomy. This procedure has the advantage of minimizing donor site morbidity.
Post-mastectomy chest reconstruction has developed into a common aspect of the treatment for breast cancer over the course of the past century. In order to ease the issues that arise after a mastectomy and to correct defects in the chest wall, reconstruction was developed. Breast reconstruction surgery offers various options such as the utilization of endoprostheses (implants), autologous tissue transfer, or a combination of both techniques [1-4].
Over the last three decades, breast reconstruction has been accomplished through various surgical methods, such as the utilization of tissue expanders in conjunction with implants, latissimus dorsi myocutaneous flaps, and transverse rectus abdominis myocutaneous (TRAM) flaps. These techniques require tissues and skin that come from elsewhere in the body. Although all reconstructive procedures are effective, the decision to use one or the other depends on the suitability of the operation and the preferences of the patient [1-4].
The latissimus dorsi muscle is a large and thin muscle that serves as the main muscle in the back of the lower chest. These muscles are located under the chest bone. Its functions are especially important in humerus movements, such as extensors, adductors, and medial rotators. This muscle is responsible for maintaining the inferior angle of the scapula to the chest wall as well as stabilizing and elevating the pelvis when the lower extremity moves forward. Another role of the muscle in question is that of the accessory respiratory muscle [3, 5-6].
The thoracodorsal artery supplies the primary muscle, which is the latissimus dorsi. The dissection reveals that the artery in question is a direct extension of the subcapular artery, originating from the third segment of the axillary artery. The lymphatic egress from this muscle conforms to a standard lymphatic drainage pattern. The procedure involves the drainage of superficial and deep lymphatics into a group of six to seven axillary lymph nodes located on the inferior edge of the posterior axillary wall. This group of lymph nodes is situated in close proximity to the subscapular veins. The innervation of the latissimus dorsi muscle is provided by the thoracodorsal nerve, which originates from the posterior cords of the brachial plexus. The predominant spinal nerve roots involved in this innervation are C6 to C8, with C7 being the most prominent [3, 5-6].
A neurovascular bundle will be moved, and it will consist of the nerves, the thoracodorsal artery, and the veins that are adjacent to it. A strong connection exists between nerves and branching arteries in the body [5-7].
Case Summary
A 45-year-old female patient was admitted to general hospital with a chief complaint of a lump in the left breast that had been present for one year. The patient presents with a hard, throbbing lump on the left breast. There are also notable changes in breast skin color and p'eau de orange, as well as pulled breast skin and retracted nipple abnormalities. No discharge from the nipple is observed. Upon initial observation, the patient presents with a small nodule measuring the size of a seed. Subsequent examination reveals that the aforementioned nodule has progressed in size to that of a ping pong ball.
The surgical procedure involving the examination and documentation of the onset of menstruation in females. At 12 years of age, the patient underwent a medical procedure. At the age of 30, the individual had her first child through surgery and subsequently received after-surgery care. She also breastfed for an extended period of 2 years. Moreover, she was prescribed KB pills, which she took for over 5 years, and has a confirmed history of using hormonal medication. The medical examination did not reveal any indications of alcohol consumption or a family history of the same illness. Radiation exposure was also not detected. The individual's profession is that of a homemaker. Although she tried alternative therapy, it did not yield any significant improvement. As a result, she decided to undergo medical treatment (Figure1).

Figure 1: Pre-Operative Clinical Appearance
The patient's medical history was negative for any systemic disease. The patient's ambulatory history indicates the ability to ambulate without the use of assistive devices. During the primary surgical assessment, it was observed that the airway was clear and the patient was breathing with a thoracoabdominal breathing pattern.
The respiratory rate was noted to be 21 breaths per minute. In terms of circulation, the heart rate was 87 beats per minute and the blood pressure was 126/93 mmHg. The patient's karnofsky score was also evaluated. The patient's performance status was assessed as 100 and their body temperature was recorded as 36.5° C. Upon completion of the secondary survey, no injuries or abnormalities were observed in the regions of the head, face, neck, abdomen, and genitalia.
The patient presents with asymmetry of the breasts, with the left breast demonstrating hypertrophy in comparison to the right breast. Further evaluation is warranted. Upon examination, it was observed that the skin color of both the right and left breasts is uniform. The skin was subjected to a slight tension test, resulting in a positive or negative response. The presence of peau de orange was also noted, along with nipple retraction, which was either positive or negative. No discharge was observed from the nipples. Patient presents with a mass in the axillary region, with uncertain characteristics. Additionally, there is a mass in the infraclavicular and supraclavicular regions, with no apparent abnormalities.
The patient underwent a surgical procedure for Ca Mammae (S) T2N0M0. The patient underwent a nipple sparing mastectomy procedure as part of their treatment. The musculocutaneous latissimus dorsi flap was selected as the surgical procedure for closing the raw surface defect in the mamae (S) region resulting from the mastectomy.
Post-surgical intervention, the patient's condition remained stable without any undesirable complications. Upon completion of the surgical procedure, the patient was advised to refrain from exposing the surgical site to moisture, exerting excessive force during routine activities, and to prioritize rest. The patient was instructed to undergo a dietary regimen consisting of high protein foods to facilitate post-operative recovery. In the event of post-discharge complications, the patient was instructed to promptly contact the emergency ward.
On the seventh day after the operation, the patient underwent a re-evaluation at an outpatient center. Upon examination, the patient diminished any symptoms of fever, nausea, vomiting, or dyspnea. Upon examination of the chest, no indications of infection were observed at the donor and recipient sites of the flap (Figure 1-4).

Figure 2: Intraoperative We Founded Defect Size 10x5 Cm at the Left Superolateral Region After Excision

Figure 3: (A) Desain Insicion for Musculocutaneous Latissimus Dorsi Flap, (B) Exposed of Musculocutaneous Latissimus Dorsi Flap

Figure 4: Post operative after Inserting Flap
Following the patient's discharge from the ward, it was advised that she undergo an evaluation of her tumor status by the oncologic department. In the event of necessity, the patient was recommended to undergo a medical procedure involving physical therapy aimed at the restoration of normal bodily function. The procedure would involve a series of progressive exercises, neuromuscular training, and functional activity training that would be tolerated by the patient (Figure 5).

Figure 5: Clinical Photograph Illustrating Breast Asymmetry
The patient underwent a successful surgical procedure, as evidenced by a positive outcome at the 3 months follow up. No new lesions were observed, and the surgical scar exhibited satisfactory healing (Figure 6).
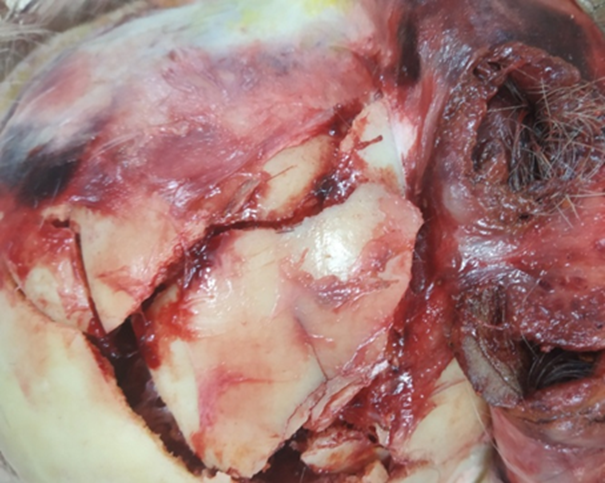
Figure 6: Post Operative Control Evaluation after 3 Months After Surgery
The patient was admitted to the hospital for a surgical procedure to address a mass located in the left breast. The patient underwent a surgical procedure for the removal of Ca mammary (S) with T2N0M0 staging following a physical and radiological assessment. Subsequent to that, medical professionals opted to perform a Nipple Sparing Mastectomy (NSM) operation. A surgical procedure was performed to repair the defect in the left mammary region by utilizing the Latissimus Dorsi Muscle Flap (LDMF) technique. The raw surface was discovered during the surgery [4,8-9].
The procedure of breast reconstruction is performed with the aim of mitigating the issues that arise after mastectomy and rectifying any anomalies in the chest wall. The surgical objective is to perform reconstruction to correct the anatomical abnormality and reestablish the breast's form and symmetry in accordance with the patient's goals. The surgical procedure of breast reconstruction presents a range of alternatives, such as endoprostheses (implants), autogenous tissue transfer, or a fusion of both methods [10-11].
The patient's cosmetic concerns have been addressed through a novel endoscopic procedure, resulting in a donor site scar that measures only 6 cm in length. Adequate closure of the donor site defect is achievable for the majority of myocutaneous flaps through surgical intervention[5,7].
Possible complications related to the correction of the defect may arise during the surgical procedure. In general, patients who undergo this surgical procedure can expect a postoperative survival rate of 95-99 percent. A surgical procedure may result in the manifestation of orocutaneous fistula in approximately 2.5% of cases. Delayed wound healing may be observed in approximately 7-10% of cases, and a hematoma may develop in approximately 2-4% of cases [5-7].
The success rates of the cure procedure are subject to variation and can be impacted by various factors, including but not limited to prior exposure to radiation, tobacco use, and diabetes. Post flap installation, a reduction in size may occur due to muscle atrophy caused by denervation. The secondary flap's volume reduction procedure can be postponed to a subsequent surgical intervention [5-6].
The Latissimus Dorsi Muscle Flap (LDMF) procedure is recommended for autogenous breast cancer reconstruction in patients who are not eligible for TRAM flap surgery due to various factors, including previous abdominoplasty or TRAM surgery, inadequate abdominal skin or fat, and high-risk comorbidities such as diabetes, obesity, or tobacco use. The surgical procedure known as Latissimus Dorsi Muscle Flap (LDMF) can be utilized to provide vascularized tissue to the chest wall suffering from ischemia in patients who have received breast irradiation [5-7].
The procedure known as Latissimus Dorsi Muscle Flap (LDMF) is utilized to provide tissue for the partial correction of a mastectomy or lumpectomy defect. The procedure may be utilized for the purpose of augmenting an inadequate or unreliable integumentary fold on an implant or for enhancing the cosmetic result of a preventive mastectomy. The patient is scheduled for a medical procedure that involves the latissimus muscle. However, due to a previous posterior lateral thoracotomy that resulted in the division of the muscle and its blood supply, as well as atrophy caused by the division of the thoracodorsal nerve during axillary node dissection, the utilization of the latissimus muscle is relatively contraindicated [6-7].
Following the procedure, a thorough observation of the patient's condition was conducted during the initial 48 hours to assess the drainage of the surgical site and the overall well-being of the individual. The postoperative evaluation was conducted at the surgical clinic after a week, revealing successful wound healing without any indications of necrosis or infection in both the donor and latissimus dorsi flap recipient. The patient's condition and complaints are monitored periodically for further adjustments.
The procedure of utilizing the latissimus dorsi myocutaneous flap is a prevalent technique in contemporary reconstructive surgery. The identified muscle can be utilized as a primary muscle flap or as a composite myocutaneous or osteomyocutaneous flap during surgical procedures. Throughout the medical operation of head and neck reconstruction, the utilization of extended pedicles and ample tissue supply provides a beneficial advantage for the reconstruction of the affected region.
The Latissimus Dorsi Muscle Flap (LDMF) procedure has been widely employed in the surgical repair of trunk and chest wall deformities, particularly in patients who have undergone mastectomy. The procedure of latissimus dorsi flap is indicated for the purpose of wound closure subsequent to the excision of tumors, as well as for the correction of insufficient adipose tissue in the mammary region. The adipose tissue deficit post-insertion cannot be substituted by the latissimus dorsi muscle. Implantation procedure.
Chang, D.W. et al. “Autologous breast reconstruction with the extended latissimus dorsi flap.” Plast Reconstr Surg, vol. 110, no. 3, 2002, pp. 751-759.
Zhang, B.N. et al. “Guidelines on the diagnosis and treatment of breast cancer (2011 edition).” Gland Surg, vol. 1, no. 1, 2012, pp. 39-61.
Ashikari, A.Y. et al. “Nipple sparing mastectomy techniques: a literature review and an inframammary technique.” Gland Surg, vol. 7, no. 3, 2018, pp. 273-287.
Gupta, A., and Borgen, P.I. “Total skin sparing (nipple sparing) mastectomy: what is the evidence?” Surg Oncol Clin N Am, vol. 19, no. 3, 2010, pp. 555-566.
Bogduk, N., Johnson, G., and Spalding, D. “The morphology and biomechanics of latissimus dorsi.” Clin Biomech (Bristol, Avon), vol. 13, no. 6, 1998, pp. 377-385.
Teisch, L.F. et al. “Latissimus dorsi flap versus pedicled transverse rectus abdominis myocutaneous breast reconstruction: outcomes.” J Surg Res, vol. 199, no. 1, 2015, pp. 274-279.
Jeno, S.H., and Varacallo, M. “Anatomy, back, latissimus dorsi.” StatPearls [Internet], 2021. Available: https://www.ncbi.nlm.nih.gov/books/NBK448120/
Sood, R. et al. “Latissimus dorsi flap in breast reconstruction: recent innovations in the workhorse flap.” Cancer Control, vol. 25, 2018, pp. 1073274817744638.
Nejadsarvari, N., Ebrahimi, A., Ebrahimi, A., and Hashem-Zade, H. “Medical ethics in plastic surgery: a mini review.” World J Plast Surg, vol. 5, no. 3, 2016, pp. 207-212.
Durkan, B. et al. “Postmastectomy radiation of latissimus dorsi myocutaneous flap reconstruction is well tolerated in women with breast cancer.” Am Surg, vol. 78, no. 10, 2012, pp. 1122-1127.
Hammond, D.C. “Latissimus dorsi flap breast reconstruction.” Plast Reconstr Surg, vol. 124, no. 4, 2009, pp. 1055-1063.
