
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3239
ISSN (Online) : 2709-3220
Background: Mucoepidermoid carcinoma (MEC) is the most common malignant salivary gland tumor, representing approximately 30–35% of all salivary gland malignancies. Primary intraosseous MEC of the jaws is an exceptionally rare entity, with fewer than 200 cases reported in the literature since its first description in 1939. Its clinical presentation is often nonspecific, contributing to delayed diagnosis and potential mismanagement. Objective: To highlight the diagnostic challenges and clinical significance of atypical presentations of intraosseous mandibular MEC, particularly those associated with neurological manifestations. Materials and Methods: We report a case of primary intraosseous MEC of the mandible with unusual clinical features, emphasizing the diagnostic process, radiological and histopathological findings and therapeutic management. Results: Intraosseous MEC typically presents as a slow-growing, painless swelling in the posterior mandible, often mimicking benign odontogenic lesions. Neurological symptoms are uncommon and usually limited to inferior alveolar nerve involvement, presenting as hypoesthesia or paresthesia. In this case, the presence of facial nerve palsy as an initial symptom represented a rare and alarming feature, suggesting advanced disease or neural invasion. Imaging and histopathological examination confirmed the diagnosis, guiding appropriate surgical management. Conclusion: Intraosseous MEC of the mandible remains a diagnostic challenge due to its rarity and nonspecific clinical presentation. The occurrence of facial nerve palsy as an initial manifestation is exceedingly rare and should raise suspicion for aggressive disease. Early recognition and comprehensive evaluation are essential to ensure accurate diagnosis and optimal management.
Mucoepidermoid Carcinoma (MEC) represents the most common malignant salivary gland neoplasm, accounting for approximately 30-35% of all salivary gland malignancies. While MEC typically arises from major and minor salivary glands, primary intraosseous mucoepidermoid carcinoma of the jaws remains an exceptionally rare entity, with fewer than 200 cases documented in the English literature since Lepp's initial description in 1939 [1].
Intraosseous MEC of the mandible predominantly affects the posterior regions, particularly the molar and premolar areas and typically presents as a slowly expanding, painless mass. The clinical presentation is often nonspecific, with patients commonly experiencing localized swelling, tooth mobility, or ill-fitting dentures. The insidious nature of these symptoms frequently leads to delayed diagnosis, as the lesion may be initially mistaken for common odontogenic pathology such as cysts or benign tumors.
Neurological manifestations, particularly cranial nerve involvement, are uncommon presenting features of mandibular intraosseous MEC. When neurological symptoms do occur, they typically involve the inferior alveolar nerve, presenting as hypoesthesia or paresthesia of the lower lip and chin. Facial nerve palsy as an initial presenting symptom is extraordinarily rare in cases of intraosseous mandibular MEC and suggests either advanced local disease with extensive soft tissue involvement or potential neural invasion patterns that warrant immediate attention.
The rarity of this presentation poses significant diagnostic challenges, as facial palsy in the context of a mandibular lesion requires careful consideration of various differential diagnoses, including perineural spread of malignancy, direct tumor extension, inflammatory processes, or coincidental pathology. The proximity of the facial nerve to the mandible, particularly in the region of the stylomastoid foramen and its course through the parotid gland, necessitates thorough evaluation of potential pathways for tumor involvement.
Early recognition and appropriate management of intraosseous MEC are crucial for optimal patient outcomes, as the prognosis is significantly influenced by tumor grade, extent of disease and adequacy of initial surgical treatment. The presence of neurological symptoms may indicate more aggressive tumor behavior or advanced disease, potentially affecting treatment planning and long-term prognosis.
We present a unique case of a 56-year-old male with primary intraosseous mucoepidermoid carcinoma of the left mandible whose initial presentation was dominated by ipsilateral facial nerve palsy, highlighting the diagnostic complexity and clinical significance of this rare presentation.
This case emphasizes the importance of considering malignant salivary gland tumors in the differential diagnosis of facial nerve palsy, even when the primary lesion appears to be located within the jawbone and demonstrates the need for comprehensive evaluation and multidisciplinary management in such complex cases.
A 56-year-old man presented to the emergency department with an acute onset of left-sided facial paralysis. He was initially treated as a case of Bell’s palsy with corticosteroids for two weeks, but no clinical improvement was observed.
On physical examination, he had a House–Brackmann grade VI left facial palsy. The patient also reported left-sided trigeminal neuralgia. Otoscopic examination was unremarkable. Palpation of the left parotid region elicited pain but no obvious mass was detected.
Given the atypical presentation with combined facial paralysis and trigeminal neuralgia, a Computed Tomography (CT) scan of the temporal bone was performed which revealed a double mass involving the ramus of the mandible and extending through the stylomastoid foramen to the temporal bone, with perineural spread into the facial canal and mastoid bone, as well as evidence of bone lysis (Figure 1).
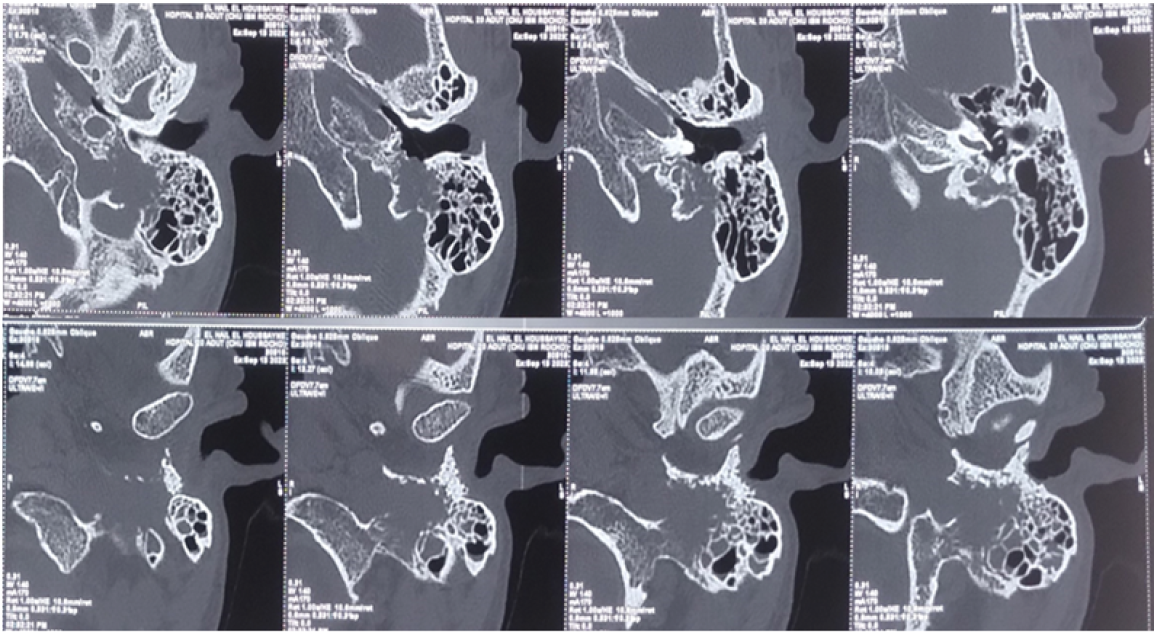
Figure 1: Axial and Longitudinal CT Scan of the Left Temporal Bone Showing the Mastoid Bone Lysis and the Extension of an Irregular Mass
Magnetic Resonance Imaging (MRI) confirmed that the primary lesion was located in the mandibular ramus, with perineural extension to the stylomastoid process and associated infiltrated lymph nodes. No evidence of an extension to the parotid gland was found (Figure 2).
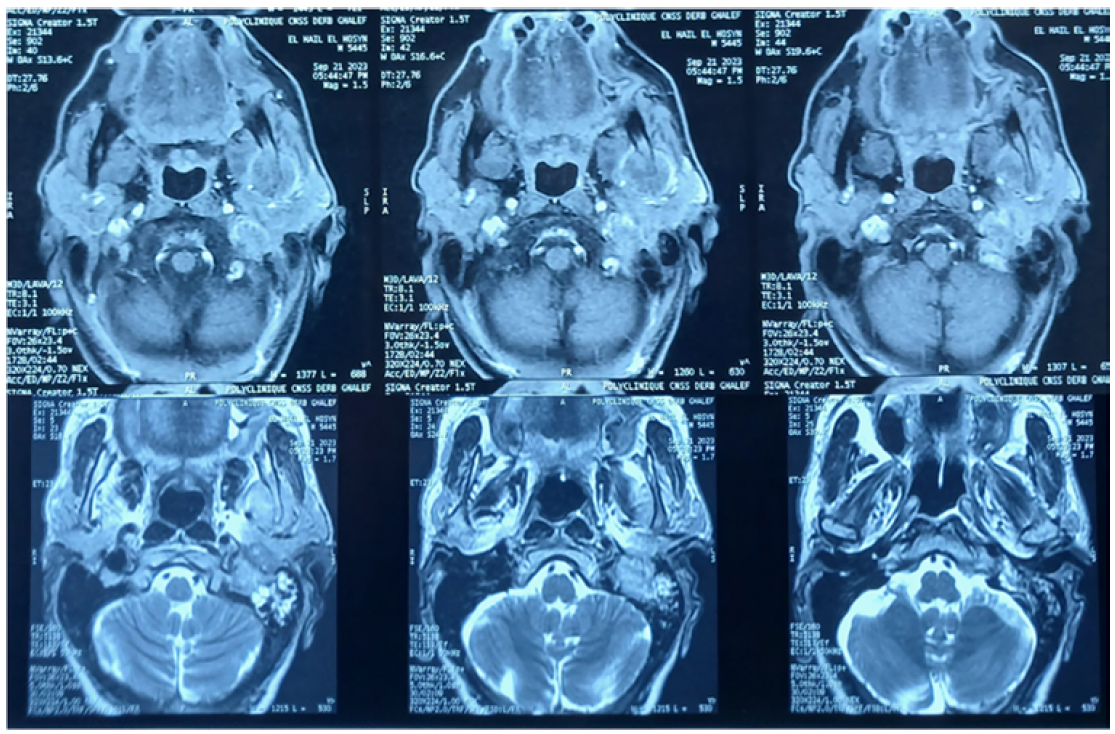
Figure 2: Cerebral MRI Showing the Extensive Mass in the Left Mandibular Ramus (Black Arrow) with an Extension to the Left Temporal Bone (Asterix)
A diagnostic biopsy was performed under general anesthesia in the left mandibular region, which revealed a carcinomatous proliferation of mucoepidermoid cells. The tumor architecture was varied, with the presence of epidermoid, mucinous and intermediate zones. The mitotic count was estimated at 6 mitoses/2 mm². Numerous images of vascular emboli and perineural invasion were found. The results confirmed an intermediate-grade mucoepidermoid carcinoma (Brandwein classification). Due to the extent of the tumor and the general status of the patient, palliative chemotherapy was recommended in a multidisciplinary tumor board.
The patient declined treatment. Unfortunately, he passed away six months after the diagnosis.
Mucoepidermoid Carcinoma (MEC) represents the most common malignant salivary gland tumor, accounting for approximately 30-35% of all salivary gland malignancies. However, intraosseous mucoepidermoid carcinoma of the mandible remains an exceptionally rare entity, with fewer than 200 cases reported in the English literature since its first description by Lepp in 1939 [1].
The present case demonstrates several characteristic features of mandibular MEC. The patient's age and gender align with established demographic patterns, as intraosseous MEC typically affects patients in their fourth to sixth decades of life, with a slight female predominance (female-to-male ratio of 1.5:1) [2,3]. The posterior mandible, particularly the molar and premolar regions, represents the most common site of involvement, as observed in our patient. The initial presentation as a slowly growing, painless swelling is consistent with previous reports, though the duration of symptoms can vary significantly.
Several malignant entities should be considered in the differential diagnosis of mandibular lesions presenting with facial nerve palsy, as this symptom suggests aggressive behavior and possible perineural invasion [4,5].
Primary intraosseous squamous cell carcinoma is a key consideration, particularly in cases arising from odontogenic epithelium or pre-existing cysts and is known for its potential for local invasion and neural involvement. Metastatic tumors to the mandible-most commonly originating from primary sites such as the breast, lung, kidney, or prostate-may also present with pain, swelling, and, in advanced stages, cranial nerve deficits including facial palsy [6].
Other salivary gland malignancies, especially adenoid cystic carcinoma, are well recognized for their marked neurotropism and propensity for perineural spread, which can lead to facial nerve dysfunction even in early stages [5-7].
Additionally, high-grade malignancies such as osteosarcoma or Ewing sarcoma of the jaw, although rare, may exhibit aggressive local extension with possible neural compromise [7].
The treatment of intraosseous MEC requires complete surgical excision with adequate margins. The extent of resection depends on tumor size, location, grade and involvement of surrounding structures. Conservative approaches, such as enucleation or curettage, are associated with high recurrence rates and are generally not recommended.
Mandibular resection with immediate or delayed reconstruction represents the standard treatment for larger lesions or those approaching vital structures. The decision between marginal and segmental resection should consider oncological principles while preserving maximum function and aesthetics [1,8,9].
The role of adjuvant radiotherapy in intraosseous MEC remains controversial. While some authors advocate radiotherapy for high-grade tumors or cases with positive margins, others question its efficacy due to the relatively radio-resistant nature of salivary gland malignancies. Adjuvant chemotherapy is typically reserved for metastatic or unrespectable disease [10,11].
The prognosis of intraosseous MEC is generally favorable, particularly for low-grade tumors completely excised with negative margins. Five-year survival rates exceed 90% for low-grade lesions but decrease significantly for high-grade tumors (60-70%). Local recurrence rates range from 5-15% and are primarily related to inadequate initial treatment [11-13]
Long-term follow-up is essential, as recurrences can occur many years after initial treatment. The potential for distant metastasis, though uncommon in low-grade tumors, necessitates comprehensive surveillance including regular imaging and clinical examination [13,14].
This case highlights the diagnostic and therapeutic challenges associated with intraosseous mucoepidermoid carcinoma of the mandible. Early recognition, appropriate imaging and prompt histopathological evaluation are crucial for optimal patient outcomes. Complete surgical excision with adequate margins remains the cornerstone of treatment, with the extent of resection tailored to individual patient factors and tumor characteristics. Given the rarity of this entity, multicenter collaborative studies would be valuable to better define optimal management strategies and long-term outcomes.
Lepp, H. “Zur kenntnis des papillar wachsenden schleimigen cystadenokarzinoms der mundhohle.” Zieglers Beiträge zur Pathologischen Anatomie, vol. 102, 1939, pp. 164–166.
Wang, Y.L. et al. “Clinicopathological features and prognostic factors of intraosseous mucoepidermoid carcinoma: A retrospective study.” Head and Neck, vol. 43, no. 5, 2021, pp. 1405–1413.
Xu, T. et al. “Central mucoepidermoid carcinoma of the jaws: clinical, radiographic and histopathologic analysis of 15 cases.” Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, vol. 129, no. 4, 2020, pp. e190–e198.
Bodner, L. et al. “Primary intraosseous squamous cell carcinoma arising in an odontogenic cyst: A clinicopathologic analysis of 116 reported cases.” Journal of Oral Pathology & Medicine, vol. 40, no. 10, 2011, pp. 733–738.
Hirshberg, A. et al. “metastatic tumors to the jawbones: analysis of 390 cases.” Journal of Oral Pathology & Medicine, vol. 43, no. 10, 2014, pp. 743–747.
Coca-Pelaz, A. et al. “Adenoid cystic carcinoma of the head and neck—An update.” Oral Oncology, vol. 51, no. 7, 2015, pp. 652–661.
Rapidis, A.D. et al. “Primary malignant tumors of the mandible: A clinicopathologic study of 12 cases.” Journal of Oral and Maxillofacial Surgery, vol. 61, no. 1, 2003, pp. 19–27.
Bell, D. and E.Y. Hanna. “Salivary gland cancers: biology and molecular targets for therapy.” Nature Reviews Clinical Oncology, vol. 19, no. 3, 2022, pp. 181–197.
Mifsud, M.J. et al. “Adjuvant radiotherapy for salivary gland malignancies: Outcomes and indications.” Oral Oncology, vol. 114, 2021, pp. 105164.
Laurie, S.A. and L. Licitra. “Systemic therapy in the palliative management of advanced salivary gland cancers.” Journal of Clinical Oncology, vol. 39, no. 17, 2021, pp. 1909–1920.
Seethala, R.R. and G. Stenman. “Update from the 5th edition of the who classification of head and neck tumors: salivary gland tumors.” Head and Neck Pathology, vol. 16, no. 1, 2022, pp. 40–53.
Bishop, J.A. et al. “WHO classification of salivary gland tumors: Recent advances.” Virchows Archiv, vol. 478, no. 1, 2021, pp. 21–30.
Alfaar, A.S. et al. “Long-term outcomes and prognostic factors in mucoepidermoid carcinoma: A contemporary analysis.” Head and Neck, vol. 45, no. 2, 2023, pp. 321–330.
Peraza, A. et al. “Mucoepidermoid carcinoma: An update and review of the literature.” Journal of Stomatology, Oral and Maxillofacial Surgery, vol. 121, no. 6, December 2020, pp. 713–720. https://doi.org/10.1016/j.jormas.2020.06.003
