
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
One of the problems facing public health is the control of Crimean-Congo hemorrhagic fever. It is a zoonotic virus that can infect the two humans and animals and occasionally result in mortality. Because of the endemic's recurrence in some regions, which called for more factual and documented information about it, this review aimed to gather the most important details regarding this virus. The infectious virus is made up of a segmented negative sense ribonucleic acid genome particle in globular shape encased in an infected viral glycoprotein-containing lipid structure. Diseases are frequently spread via ticks through blood or tissue from humans or animals. When there are mammals present, regardless of size, such as cattle and rabbits, the causative virus can spread quickly. Unlike in animals, where it is asymptomatic, in people it results in a high fever and hemorrhagic condition. Precautionary steps to manage tick vectors in endemic countries are recommended, as is fostering collaboration among clinical veterinary, medical, and ecology specialists.
Cimean-Congo hemorrhagic fever poses a significant risk to public health as a result of its negative consequences on social and economic well-being as well as human health [1].
(CCHF) is brought on by infection with the Bunyavirus family member Narivirus, which is transmitted by Ixodes ticks. Despite being named after its initial outbreaks in the Congo (1969) and Crimea (1944), it is no longer exclusive to these nations. As per the World Health Organization (WHO), CCHF is currently endemic to countries in most of Africa, the Balkans, the Middle East, and much of Asia [2]. It is one of the zoonotic illnesses that infect people. A simple definition of zoonosis is an infectious disease brought on by pathogens that are spread from one animal species to humans [3-5].
Recently, it has become a challenge for public health, particularly in the wake of COVID-19, the most recent epidemic, which caused injury to millions of people worldwide in addition to financial losses. Therefore, there are still concerns about the advent of other outbreaks that could get out of hand, particularly ones that become viral [6-8]. CCHF is asymptomatic in between 60 and 80% of patients, while the remaining between 20 and 40% typically exhibit gastrointestinal symptoms after an initial fever, headache, and malaise; serious situations may include hemorrhage, shock, and multi-organ system failure [9]. Severity is linked to unchecked increased cytokine levels and viral replication in host tissues; as a result, immune-mediated diseases that can result in vascular dysfunction in addition, more frequently, extreme situations, demise, as well as viral pathologies [10]. The geographical distribution of There is a correlation between CCHF and the hard tick vector, which is mostly the plant Hyalomma marginatum, which is widespread in Europe, Asia, and Africa [11]. There have been recent outbreaks documented and an increase in conditions in Iraq's neighbors to the north and east, Turkey and Iran, which are prevalent in CCHF [12]. 20–30% prevalence rates for CCHF in sheep, camels, and animals were discovered in Iraq, Iran, and Turkey in a 2016 sero-epidemiologic survey. Comparatively, all three countries had a higher frequency of CCHF in goats (50%) than in any other animal [13].
The Nairovirus CCHFV belongs to the Bunyaviridae family, it includes the genera as well Orthobunyavirus, Hantavirus, Tospovirus, and Phlebovirus, [19]. Except for Tospovirus, which affects plants (20), these genera are all recognized for including illnesses that affect humans. Nairoviruses are viruses carried by ticks that are distinguishable from other bunyaviruses through their long genomic L segments [19, 21]. The virus that causes Crimean-Congo hemorrhagic fever is encased in RNA with an 80-100nm diameter [21].
The virus has a three-segment antisense RNA genome that is labeled S, M, and L segments (for small, medium, and large) in accordance with their relative lengths [14]. The RNA polymerase [14], Gn, and Gc constitute two membrane glycoproteins (also known as gap 1 and gap 2 in other Bunyaviridae), a nonstructural protein (NSm), and the nucleocapsid protein are the viral proteins [15]. The Gn glycoprotein consists of an ectodomain with 176 residues, a transmembrane region with 24 residues, and a long cytoplasmic tail with 100 residues in the mature virion [16]. A lipid structure encases the DNA and includes the G1 and G2 viral glycoproteins [17].
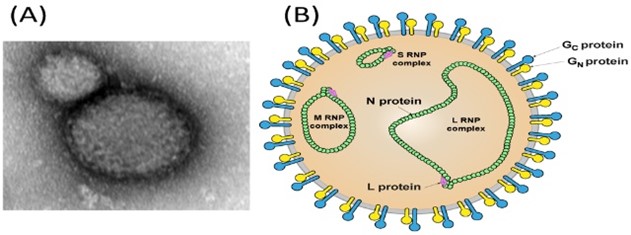
Figure 1. The CCHF virus's structure [18].
Crimean-Congo hemorrhagic fever infections are mostly asymptomatic and enzootic in a variety of species [22]. The CCHFV can spread to humans through contact with infected individuals, animal tissues, or blood., as well as bites from ticks [23]. Hospital nosocomial outbreaks are associated with resource- constraints situations [24]. In 2008, as an illustration, a nosocomial epidemic was recorded in Al- Fulah, Kordufan, Sudan, when a sixty-year-old male butcher was taken to the hospital. Because personal protective equipment (PPE) was not used, the virus was transferred to nurses who had assisted with the index patient and the execution of severe infection control procedures [24]. Ticks of the Hyalomma, the genus, are the most common origin of diseases in humans, possibly because mature and immature ticks require host blood at every developmental stage [19]. Hyalomma ticks act as CCHFV reservoirs and additional vectors [25]. The female nymphs and larvae of the Hyalomma tick graze on small mammals, whereas the adults consume ungulates and spread the CCHFV virus through transovarian and transstadial transmission in the wild, birds, or reptiles [26]. Determining the role of reptiles as adept hosts for reservoirs and the transmission of the CCHFV is essential. Animals acquire CCHFV when they are bitten by an infected tick. As a result, when healthy ticks feed on the blood of the diseased host, the virus transmits to them. Ticks may also contract diseases while co-feeding on the same host by ticks that are infected or not, as well as viral components contained in tick saliva that promote viral transmission [21]. All mammals, however, are similarly vulnerable to become infected with the CCHFV [27]. Birds are thought to be inadequate hosts used in the replication and spread of CCHFV since they frequently exhibit resistance to becoming viremic [28]. Humans are often regarded as secondary, dormant hosts for CCHFV. Bites from ticks, getting in touch with the blood and tissues of animals that are virus-positive, and contact with tissues and bodily human infection fluid or blood are the most common ways for people to become infected [19]. The risk of spreading CCHFV can be decreased by changing land use and limiting the movement and commerce of affected livestock. During previous outbreaks in the Arab world, contact with tainted blood from dead bodies through an infected animal's wound or mucous membrane was discovered to be the most widely used CCHFV transmission technique.
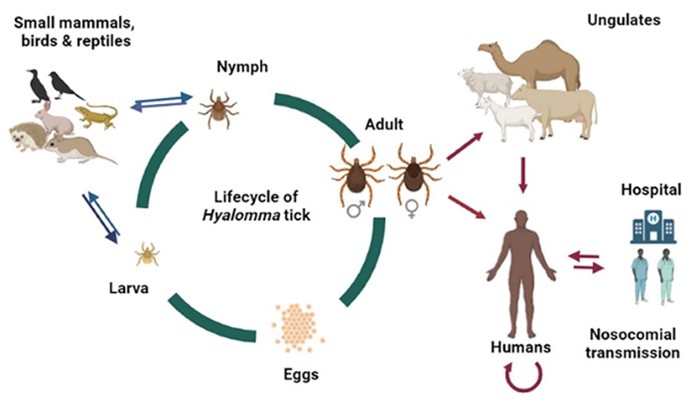
Figure 2. Hyalomma tick life cycle and probable CCHFV transmission vector in the Arab world. BioRender was used to generate the original figure [21].
In humans, this sickness is distinguished by an abrupt high temperature, chills, and dizziness, as well as gastrointestinal abnormalities like diarrhea and vomiting. The period prior to the hemorrhage stage normally lasts three days. The illness requires a week to incubate. The patient experiences blood loss from the skin, ranging from bruises to petechiae, as well as blood loss from the respiratory, digestive, and urinary systems, which shortens the hemorrhagic phase [29]. Infection in animals generally, particularly the lack of clinical indications, is a defining characteristic of both wild and domesticated mammals. Viremia, on the other hand, can last up to fourteen days in mammals. Animals have a significant influence in the infection's life cycle, and the virus that causes it multiplies before being sent to humans through ticks [30].
The early steps in the diagnosis of CCHF should involve the accurate collection of patient data, a physical examination, a review of recent travel history, and the use of specialist laboratories to analyze tissue and blood samples. (RT-PCR), IgG and IgM antibody detection by ELISA, and separation of viruses are currently the foundation of laboratory techniques for CCHF diagnostics [31]. Ribavirin is the most often used antiviral medication in CCHF. However, data on the efficacy of this medication in humans has come from observational studies [32]. An evaluation of the effectiveness of favipiravir in a mouse model as an inhibitor of viral polymerase with a broad spectrum indicated that it was superior to ribavirin [33]. In severe cases of CCHF, ribavirin treatment in conjunction with plasmapheresis to reduce the burden from proinflammatory cytokines has been reported to be beneficial [34].
The use of active tick surveillance is necessary to mitigate the spread of the disease via the tick vector. The incidence, location, and the prevalence of CCHFVV infection among tick carriers in a specific geographic area must be tracked for this purpose [35]. Applying acaricides to farms where livestock are raised is the primary method of prevention for this infection. It is well recognized that the absence of symptoms of this illness makes it difficult to control its animal host. A fourteen-day premortem for the duration of quarantine is recommended in regions where it is endemic when using acaricides prior to animal slaughter. Controlling the movement of animals across borders, particularly to endemic nations, and taking precautions to prevent infection in humans, particularly in at-risk groups, are also necessary [36]. Consideration should be given to the application of personal defense equipment (PPE) in medical environments. While caring for CCHF patients, healthcare personnel run the danger of suffering needlestick injuries. Therefore, it is recommended to utilize needle-safe devices. It is similarly crucial to safeguard additional patients and their family members against the nosocomial transmission of CCHFV. To reduce contact with patients who have CCHF, hospitals should have enough isolation rooms [37]. Unfortunately, there isn't a known vaccine that is also secure. People who interact with animals and those who live in tick-infested areas of the countryside should wear long, light-colored protective garments [38]. But if a tick becomes attached, it has to be swiftly removed using thin-tipped tweezers, and the bite sites are supposed to be washed, and the palms should be as clean as feasible. When handling the corpses and bodily fluids of dead animals, caution must be exercised [39].
CCHF is a zoonotic illness that endangers the health of the general public. As a result of climate change, travel, and the trade of animals, the disease's geographic range is rapidly expanding. The distribution of Hyalomma ticks is also expanding as a result of changes in the host range distribution pattern, which increases the risk of contracting CCHFV. In endemic nations, local governments should put in place efficient tick vector control measures. Collaboration between medical professionals, environmental scientists, and clinical veterinarians should also be supported.
Lahariya, C., Goel, M. K., Kumar, A., Puri, M., & Sodhi, A. “Emergence of viral hemorrhagic fevers: Is recent outbreak of crimean congo hemorrhagic fever in India an indication?”. Journal of Postgraduate Medicine (2012): 39 https://www.researchgate.net/publication/221885941
Watts, D. M., Ksiazek, T. G., Linthicum, K. J., & Hoogstraal, H. “Crimean-Congo hemorrhagic fever”. The Arboviruses (2019): 177-222
Ghareeb, O. A., & Ali, Q. A. “Waterborne Zoonotic Bacterial Pathogens”. Texas Journal of Medical Science (2023): 63-69 https://doi.org/10.62480/tjms.2023.vol21.pp63-69
Ghareeb, O. A., & Sultan, A. I.” Nipah-An Emerging Viral Zoonotic Disease: A Review”. Annals of the Romanian Society for Cell Biology (2021): 456-465 http://annalsofrscb.ro
Ghareeb, O. A. “ Ebola-A fatal Emerging Zoonotic Disease: A Review”. Annals of the Romanian Society for Cell Biology (2021): 8748-8754 http://annalsofrscb.ro
Kzar, A. J., Faiq, T. N., & Ghareeb, O. A. “Recent infection with black fungus associated with COVID-19: a review”. Pakistan Journal of Medical and Health Sciences (2021): 1771-1773 https://doi.org/10.53350/pjmhs211551771
Al-Haidari, K. A., Faiq, T. N., & Ghareeb, O. A. “Preventive value of black seed in people at risk of infection with COVID–19”. Pakistan J Med Health Sci (2021): 384-387 https://pjmhsonline.com
Ciloglu, A., Ibis, O., Yildirim, A., Aktas, M., Duzlu, O., Onder, Z., & Inci, A. “Complete mitochondrial genome characterization and phylogenetic analyses of the main vector of Crimean-Congo haemorrhagic fever virus: Hyalomma marginatum Koch, 1844”.Ticks and Tick-Borne Diseases (2021): 101736 https://www.sciencedirect.com
Alhilfi, R. A., Khaleel, H. A., Raheem, B. M., Mahdi, S. G., Tabche, C., & Rawaf, S.”Large outbreak of Crimean-Congo haemorrhagic fever in Iraq, 2022”. IJID regions (2023): 76-79 https://www.ncbi.nlm.nih.gov
Rodriguez, S. E., Hawman, D. W., Sorvillo, T. E., O'Neal, T. J., Bird, B. H., Rodriguez, L. L.& Spengler, J. R.” Immunobiology of Crimean-Congo hemorrhagic fever”. Antiviral research (2022): 105244 https://pubmed.ncbi.nlm.nih.gov
Messina, J. P., Pigott, D. M., Golding, N., Duda, K. A., Brownstein, J. S., Weiss, D. J. & Hay, S. I. “The global distribution of Crimean-Congo hemorrhagic fever”. Transactions of the Royal Society of Tropical Medicine and Hygiene (2015) 503-513 https://doi.org/10.1093/trstmh/trv050
Sah, R., Mohanty, A., Mehta, V., Chakraborty, S., Chakraborty, C., & Dhama, K. “Crimean-Congo haemorrhagic fever (CCHF) outbreak in Iraq: Currently emerging situation and mitigation strategies–Correspondence”. International Journal of Surgery (2022): 106916 https:// DOI: 10.1016/j.ijsu.2022.106916
Spengler, J. R., Bergeron, É., & Rollin, P. E.” Seroepidemiological studies of Crimean-Congo hemorrhagic fever virus in domestic and wild animals”. PLoS neglected tropical diseases (2016): e0004210 https://doi.org/10.1371/journal.pntd.0004210
Schmaljohn, C. S., and Hooper, J. W. “in Bunyaviridae: the Viruses and Their Replication, 4th Ed. Fields Virology (Knipe, D. M., and Howley,P. M. eds.), Lippincott, Williams & Wilkins, Philadelphia”(2001): https://www.sciencedirect.com › topics › neuroscience
Sanchez, A. J., Vincent, M. J., Erickson, B. R., & Nichol, S. T. “Crimean-congo hemorrhagic fever virus glycoprotein precursor is cleaved by Furin-like and SKI-1 proteases to generate a novel 38-kilodalton glycoprotein”. Journal of virology (2006): 514-525 https://doi.org/10.1128/jvi.80.1.514-525.2006
Altamura, L. A., Bertolotti-Ciarlet, A., Teigler, J., Paragas, J., Schmaljohn, C. S., & Doms, R. W. “Identification of a novel C-terminal cleavage of Crimean-Congo hemorrhagic fever virus PreGN that leads to generation of an NSM protein”. Journal of virology (2007): 6632-6642 https://doi.org/10.1128/jvi.02730-06
Sánchez-Seco, M. P., Sierra, M. J., Estrada-Peña, A., Valcárcel, F., Molina, R., de Arellano, E. R., & Negredo, A. “Widespread detection of multiple strains of Crimean-Congo hemorrhagic fever virus in ticks, Spain”. Emerging Infectious Diseases (2022) 394 http://doi.10.3201/eid2802.211308
Wang, W., Liu, X., Wang, X., Dong, H., Ma, C., Wang, J., ... & Guo, Y. “Structural and functional diversity of nairovirus-encoded nucleoproteins”. Journal of virology (2015): 11740-11749 https://doi.org/10.1128/jvi.01680-15
Bente, D. A., Forrester, N. L., Watts, D. M., McAuley, A. J., Whitehouse, C. A., & Bray, M. “Crimean-Congo hemorrhagic fever: history, epidemiology, pathogenesis, clinical syndrome and genetic diversity”. Antiviral research (2013): 159-189 https://pubmed.ncbi.nlm.nih.gov
Olaya, C., Adhikari, B., Raikhy, G., Cheng, J., & Pappu, H. R. “Identification and localization of Tospovirus genus-wide conserved residues in 3D models of the nucleocapsid and the silencing suppressor proteins”. Virology journal (2019) 1-15 7 https://doi.org/10.1186/s12985-018-1106-4
Perveen, N., & Khan, G. “Crimean–Congo hemorrhagic fever in the Arab world: a systematic review”. Frontiers in Veterinary Science (2022): 938601 https://doi.org/10.3389/fvets.2022.938601
Spengler, J. R., Bergeron, É., & Rollin, P. E. “Seroepidemiological studies of Crimean-Congo hemorrhagic fever virus in domestic and wild animals”. PLoS neglected tropical diseases (2016): e0004210 https://doi.org/10.1371/journal.pntd.0004210
Papa, A., Tsergouli, K., Tsioka, K., & Mirazimi, A. “Crimean-Congo hemorrhagic fever: tick-host-virus interactions”. Frontiers in cellular and infection microbiology (2017): 213 https://doi.org/10.3389/fcimb.2017.00213
Aradaib, I. E., Erickson, B. R., Mustafa, M. E., Khristova, M. L., Saeed, N. S., Elageb, R. M., & Nichol, S. T. “Nosocomial outbreak of Crimean-Congo hemorrhagic fever, Sudan”. Emerging infectious diseases (2010): 837 http://doi. 10.3201/eid1605.091815
Sorvillo, T. E., Rodriguez, S. E., Hudson, P., Carey, M., Rodriguez, L. L., Spiropoulou, C. F., ... & Bente, D. A. “Towards a sustainable one health approach to crimean–congo hemorrhagic fever prevention: Focus areas and gaps in knowledge”. Tropical Medicine and Infectious Disease (2020): 113 https://doi.org/10.3390/tropicalmed5030113
Gargili, A., Estrada-Peña, A., Spengler, J. R., Lukashev, A., Nuttall, P. A., & Bente, D. A. “The role of ticks in the maintenance and transmission of Crimean-Congo hemorrhagic fever virus: A review of published field and laboratory studies”. Antiviral research (2017): 93-119 http://doi. 10.1016/j.antiviral.2017.05.010
Shepherd, A. J., Leman, P. A., & Swanepoel, R. “Viremia and antibody response of small African and laboratory animals to Crimean-Congo hemorrhagic fever virus infection”. The American journal of tropical medicine and hygiene (1989): 541-547 https://doi.org/10.4269/ajtmh.1989.40.541
Shepherd, A. J., Swanepoel, R., Leman, P. A., & Shepherd, S. P. “Field and laboratory investigation of Crimean-Congo haemorrhagic fever virus (Nairovirus, family Bunyaviridae) infection in birds”. Transactions of the Royal Society of Tropical Medicine and Hygiene (1987): 1004-1007 http://doi.10.1016/0035-9203(87)90379-8.
Hawman DW.”Feldmann H. Crimean–Congo haemorrhagic fever virus”. Nature Reviews Microbiology (2023): 463-477
https://doi.org/10.3390/diagnostics13162708
Spengler, J. R., Estrada-Peña, A., Garrison, A. R., Schmaljohn, C., Spiropoulou, C. F., Bergeron, É., & Bente, D. A. “A chronological review of experimental infection studies of the role of wild animals and livestock in the maintenance and transmission of Crimean-Congo hemorrhagic fever virus”. Antiviral research (2016): 31-47 http://doi. 10.1016/j.antiviral.2016.09.013
Serretiello, E., Astorri, R., Chianese, A., Stelitano, D., Zannella, C., Folliero, V., ... & Galdiero, M. “The emerging tick-borne Crimean-Congo haemorrhagic fever virus: A narrative review”. Travel Medicine and Infectious Disease (2020): 10187 http://doi. 10.1016/j.tmaid.2020.101871
F. de la Calle-Prieto, A. Martín-Quir´os, E. Trigo, M. Mora-Rillo, M. Arsuaga,M. Díaz-Men´endez, J.R. Arribas.” Therapeutic management of Crimean-Congo-haemorrhagic fever”. Enfermedades infecciosas y microbiologia clinica (English ed.) (2018): 517–522 http://doi: 10.1016/j.eimce.2017.04.016
Hawman, D. W., Haddock, E., Meade-White, K., Williamson, B., Hanley, P. W., Rosenke, K., & Feldmann, H.”Favipiravir (T-705) but not ribavirin is effective against two distinct strains of Crimean-Congo hemorrhagic fever virus in mice”. Antiviral research (2018): 18-26 http://doi. 10.1016/j.antiviral.2018.06.013
Fillâtre, P., Revest, M., & Tattevin, P. “Crimean-Congo hemorrhagic fever: An update”. Medecine et maladies infectieuses (2019): 574-585 https://www.sciencedirect.com
Sharma, S. N., Singh, R., Balakrishnan, N., Kumawat, R., & Singh, S. K. “Vectors of Crimean-Congo hemorrhagic fever (CCHF): prevention and its control. Journal of Communicable Diseases (2020): 22-26 https://orcid.org/0000-0001-8569-1661
Al-Rubaye, D., Al-Rubaye, T. S., Shaker, M., & Naif, H. M. “Recent outbreaks of crimean–congo hemorrhagic fever (CCHF) In Iraq”. Sci Arch, (2022): 109-112 http://doi.org/10.47587/SA.2022.3205
Fletcher, T. E., Gulzhan, A., Ahmeti, S., Al-Abri, S. S., Asik, Z., Atilla, A., & Leblebicioglu, H. “Infection prevention and control practice for Crimean-Congo hemorrhagic fever—A multi-center cross-sectional survey in Eurasia”. PloS one (2017):e0182315 https://doi.org/10.1371/journal.pone.0182315
Mohammed, T. A., Mostafa, A. H., Ahmad, J. Q., Yahya, N. B., & Tayib, G. A. “The Trojan horse feature of SARS-CoV-2 behind the re-emergence of the Crimean-Congo hemorrhagic fever in Iraq”. Human Vaccines & Immunotherapeutics (2022): 2128610 https://doi.org/10.1080/21645515.2022.2128610
