
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Background: Bacterial co-infections in COVID-19 patients can lead to increased morbidity and mortality, necessitating prompt recognition and appropriate management. Aim: The study aimed to characterize bacterial infections in COVID-19 patients, providing valuable insights into co-infections and their clinical implications. Materials and Methods: The study conducted in Kirkuk city from March 10, 2022, to September 1, 2022, aimed to investigate bacterial infections in COVID-19 patients admitted to Al-Shifaa Epidemiological Hospital. The study included 104 individuals of different age groups and sexes who tested positive for COVID-19 and required hospitalization. The severity of COVID-19 was determined by specialized physicians based on internal medicine practices and CT scan results. Data were collected through interviews using a structured questionnaire to gather demographic characteristics and clinical presentations of the patients. COVID-19 diagnosis was confirmed using WHO criteria and RT-PCR of nasopharyngeal specimens following approved protocols. Respiratory samples (nasopharyngeal swabs) were collected under medical supervision for further analysis. The cultural diagnosis involved studying the color, shape, size, edge, and height of the growing colonies to identify the bacteria. Different culture media were used for this purpose, such as the solid MacConkey medium to differentiate fermented lactose colonies from non-fermented ones. Another medium, the solid chrome medium, was used to diagnose bacterial growth based on specific colors associated with each bacteria. Results: The study investigated the relationship between COVID-19 severity and various factors, including age, sex, body mass index (BMI), comorbidities, and bacterial infections. The findings indicated that severe COVID-19 cases were more prevalent among elderly patients (>57 years) and those with obesity, diabetes, respiratory problems, chronic kidney disease, cerebrovascular diseases, and autoimmune diseases. However, pregnancy did not show a significant association with severe COVID-19. Regarding clinical features, severe COVID-19 cases were more likely to present with dyspnea, headache, anosmia, and ageusia. Among the bacterial infections, Enterococcus faecalis was the most frequently isolated bacteria in COVID-19 patients, followed by Klebsiella pneumoniae and Staphylococcus aureus. Among the bacterial isolates, Enterococcus faecalis shows the highest occurrence in severe COVID-19 cases, constituting 64.52% of positive cases in this category. 64.71 percent of mild COVID-19 patients had Klebsiella pneumoniae. In mild, moderate, and severe COVID-19 instances, Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Staphylococcus epidermidis, and Proteus mirabilis are found in varying amounts. Cephalothin and Imipenem showed great sensitivity against all isolates without resistance. Clindamycin and Carbenicillin were completely insensitive to all isolates. Conclusion: In severe COVID-19 instances, bacterial co-infections must be identified. Severe cases had Enterococcus faecalis, highlighting the necessity for specific antibiotics. Drug stewardship reduces antibiotic resistance and improves patient outcomes. More study is needed to understand COVID-19 patients' viral-bacterial interactions.
The existence of a bacterial co-infection is a common effect of viral illnesses. This co-infection is linked to an increase in morbidity and mortality, as well as a larger drain on the resources that are available in healthcare. It is likely that significant bacterial infections will be undetected when everyone's attention is focused on COVID-19. Because of this, it is of the utmost importance to determine whether or not individuals who have COVID-19 also have another illness at the same time. It enables us to put into practice the appropriate management and control of antibiotic consumption, as well as the effective delivery of antimicrobial stewardship [1-2]. A number of different data have been uncovered about the prevalence of bacterial co-infection with COVID-19. The majority of these studies use the assumption that the incidence of bacterial co-infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is lower than the incidence of bacterial co-infection with influenza and other viral diseases [3]. On the other hand, some opinions based on the previous experience with the outbreak of severe acute respiratory syndrome (SARS) in 2003 and the outbreak of Middle East Respiratory Syndrome in 2012 suggest an underestimation of bacterial co-infections in COVID-19 as a result of the non-discriminatory use of antibiotics or the limitation of the overwhelmed clinical examinations in healthcare systems during the pandemic. These opinions are supported by previous experience with the outbreaks of SARS and MERS. Bacteria have the capacity to boost viral competence by augmenting virion stability, stimulating viral infection of eukaryotic cells, and increasing the rates of co-infection. All of these effects lead to an increase in viral competence. In a similar manner, the attachment of viruses to bacteria can have an impact on the biology of bacteria, including the capacity of bacteria to bind to eukaryotic cells [4]. When patients with COVID-19 require intensive care, including help from invasive mechanical ventilators, it is of the utmost importance to rule out the presence of any bacterial co-infections. For instance, bacterial co-infections were discovered in more than a third of the children who required invasive ventilation for bronchiolitis treatment. There was a correlation between these infections and longer hospitalizations in pediatric intensive care units as well as increased usage of mechanical ventilation [5]. In addition, patients who are admitted to the intensive care unit (ICU) with a prolonged illness or intubation have a higher incidence of the identification of multidrug-resistant gram-negative bacteria, which most likely reflects hospital-acquired infection. Patients who are admitted to the ICU with a protracted illness or intubation have a higher incidence of the identification of multidrug-resistant gram-negative bacteria. In light of this, it is vital, while evaluating these patients, to take into account (check and treat on an empirical basis) the likelihood of bacterial co-infection. Taking this into account means treating on an empirical basis [6]. Regrettably, there is no general agreement about the treatment of those who have COVID-19 sickness. Not only does the course of therapy change depending on the location, but it also differs depending on the nation. Because of this, medical specialists strongly advise against the routine use of prophylactic antibiotics in patients who have COVID-19. This is especially true for patients who are not intubated or who are in the early stages of the disease. They recommend, as an alternative, keeping a vigilant lookout for any symptoms of a secondary infection, in particular in severely sick patients who have been brought to the intensive care unit for more than 48 hours [7]. The purpose of this study was to describe bacterial infections in COVID-19 patients in the hopes of gaining useful insights regarding co-infections and the therapeutic implications of those infections.
A cross-sectional study was done in the Kirkuk/Iraq from March 10 to September 1, 2022. 104 people who had already been infected with the Covid-19 virus and were hospitalized at the Al-Shifaa Epidemiological Hospital in Kirkuk city took part in the study.
These people were of both sexes and different ages (less than 18 years old). Patients with a severity level of 19 on the Covid scale, which is based on hospital-based internal medicine specialists and CT scan results.
An interview was done with these patients using a questionnaire form made by the researcher. This form included questions about their age, weight, height, etc., as well as their demographic information (Appendix I).
WHO criteria and/or RT-PCR of nasopharyngeal specimens, as well as instructions for companies that make lab materials, were used to diagnose Covid-19 infection using the PCR device in the Public Health Laboratory in the city of Kirkuk, where the infection was confirmed by following the Ministry of Health's protocols. Also, the companies that make laboratory materials were given clear instructions.
Clinical Presentation
Based on the rules that the China Center for Disease Control and Prevention used in this study to classify the clinical spectrum of COVID-19, a person with COVID-19 infection could have no symptoms or have severe acute respiratory distress [8] (Figure 1).
The trained doctor oversaw the collection of 104 nasopharyngeal swabs from patients' noses and throats. Under the watch of a doctor, these samples were taken.
Suspicious subcultures from blood cultures were grown directly on chocolate agar, 5 percent sheep blood agar, MacConkey agar, and supplemented anaerobic blood agar. All of the isolates were put in an aerobic environment at 35 degrees Celsius for 24 hours.
Suspicious colonies were then picked for a final microscopic examination, testing of the culture, and biochemical testing.
Isolated colonies were put on clean slides and dried by air. The Gram stain was then used to color the smears. Under a light microscope with an oil immersion objective lens at 100X power, the Gram stain reaction and the arrangement of bacterial cells were looked at. With the help of a 10X lens, the shape and size of colonies that were kept separate were carefully studied.
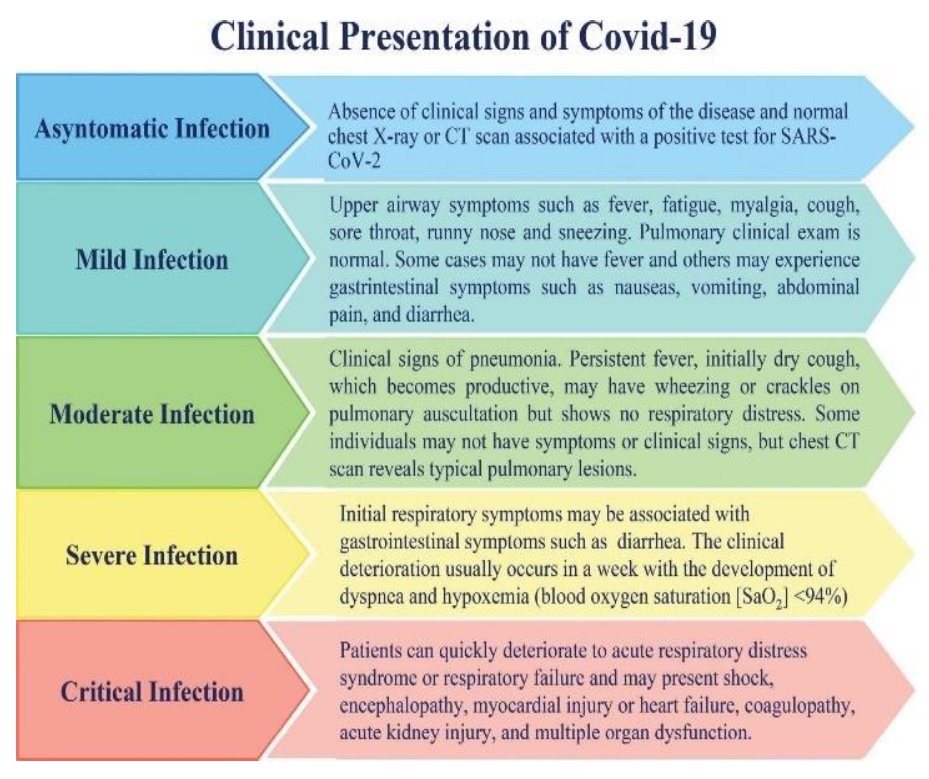
Figure 1: Specimen Collection for Swab Culture.
Cultural Diagnosis
The bacteria that were growing on the media were figured out by looking at the color, shape, size, edge, and height of the growing colonies. To get single pure cultures, the colonies were grown over and over again, and the growing characteristics of the colonies were studied on the following culture media:
It was put to the test by having bacteria make the hemolysin enzyme in a solid blood base medium, and the shape and color of the colonies that formed were recorded.
Solid MacConkey medium: This medium was used to look at the shape of the colonies and separate the ones that had fermented lactose from the others. This was done because colonies of lactose that have been fermented show up as red or pink on the surface of the medium while colonies of organisms that haven't been fermented show up as clear.
Because it has a solid base and blood azide, this medium is thought to favor the growth of enterococcal bacteria. In this medium, which has sodium azide in it, the colonies seem to have a grayish color to them.
This medium was used to test how well enterococci could ferment mannitol sugar. As the experiment went on, the medium's color changed from pink to yellow.
Solid chrome medium: The color of the colony growing on this medium can be used to tell what kind of bacteria is growing on it, since each kind of bacteria has its own color.
Statistical Analysis
Computerized statistically analysis was performed using Statistical Package for the Social Sciences (SPSS) ver. 23.1 statistic program. Comparison was carried out using chi-square (X2), T-Test, analysis of variances (ANOVA) and for calculation of probability (p) value.
Interpretation of p. value:
>0.05 (non-significant)
≤0.01 (highly significant)
General Characteristics of Covid-19 Patients
The study found that most people with severe covid-19 infections were over the age of 57, while most people with mild infections were young. There was a strong link between severity and age. The study didn't find any differences between men and women when it came to COVID-19 infection, even though men were more likely to get sick from the virus than women. The study found that most people with a severe COVID-19 infection have a high BMI, while most people with a mild infection have a normal or low BMI. There is a strong link between the two. The study found that most people with severe covid-19 infections were over the age of 57, while most people with mild infections were young. There was a strong link between severity and age. The study didn't find any differences between men and women when it came to COVID-19 infection, even though men were more likely to get sick from the virus than women. The study found that most people with a severe COVID-19 infection have a high BMI, while most people with a mild infection have a normal or low BMI. There is a strong link between the two. between obesity and severity of COVID-19 infection. More details were listed in Table 1.
Table 1: General Characteristics of Covid-19 Patients
Epidemiological Parameters | Mild N (%) | Moderate N (%) | Severe N (%) | Total N (%) | p. value |
Age Groups (years) | |||||
18-27 | 16 (88.89) | 2 (11.11) | 0 (0) | 18 (100) | <0.001 |
28-37 | 6 (66.67) | 3(33.33) | 0(0) | 9(100) | |
38-47 | 11 (64.71) | 4(23.53) | 2(11.76) | 17(100) | |
48-57 | 6(40) | 5(33.33) | 4(26.67) | 15(100) | |
58-67 | 0(0) | 5(29.41) | 12(70.59) | 17(100) | |
>67 | 1(3.57) | 13(46.43) | 14(50) | 28(100) | |
Total | 40 (38.46) | 32 (30.77) | 32 (30.77) | 104 (100) | |
Sex | |||||
female | 17(38.64) | 13(29.55) | 14(31.82) | 44(100) | 0.96 |
male | 23(38.33) | 19(31.67) | 18(30) | 60(100) | |
Obese | |||||
Underweight | 4 (66.67) | 1(16.67) | 1(16.67) | 6(100) | 0.045 |
Normal | 24(48.98) | 11(22.45) | 14(28.57) | 49(100) | |
Overweight | 10(32.26) | 11(35.48) | 10(32.26) | 31(100) | |
Obese | 2(11.11) | 9(50) | 7(38.89) | 18(100) | |
The study found that more than half of diabetic patients with COVID-19 infection had a severe infection. There was a strong link between type 2 diabetes and severe COVID-19 infection. In this study, there was also no link between being pregnant and having a severe COVID-19 infection. The study found a strong link between respiratory problems and severe COVID-19 infections, since most people with severe COVID-19 infections also had respiratory problems. The study also found a strong link between chronic kidney disease and severe COVID-19 infections, since most people with these diseases also had severe COVID-19 infections (Table 2).
Table 2: Comorbidities Among Covid-19 Patients
Comorbidities | Mild (n) | Moderate (n) | Severe (n) | Total (n) | p. value |
Diabetes | 3 (12) | 8 (32) | 14 (56) | 25 (100) | <0.001 |
Pregnant | 1 (33.33) | 2 (66.67) | 0 (0) | 3 (100) | 0.32 |
Respiratory Problem | 0 (0) | 2 (16.67) | 10 (83.33) | 12 (100) | <0.001 |
Chronic Kidney Diseases | 0 (0) | 2 (13.33) | 13 (86.67) | 15 (100) | <0.001 |
Cerebrovascular diseases | 0 (0) | 1 (16.67) | 5 (83.33) | 6 (100) | 0.013 |
Autoimmune diseases | 0 (0) | 1 (100) | 0 (0) | 1 (100) | 0.32 |
Cancer | 0 (0) | 2 (66.67) | 1 (33.33) | 3 (100) | 0.28 |
Thyroid Diseases | 0 (0) | 1 (50) | 1 (50) | 2 (100) | 0.52 |
Mental illness | 0 (0) | 1 (50) | 1 (50) | 2 (100) | 0.54 |
Rheumatoid arthritis | 0 (0) | 0 (0) | 1 (100) | 1 (100) | 0.32 |
Liver diseases | 0 (0) | 0 (0) | 1 (100) | 1 (100) | 0.32 |
The study showed a significant relation of observed clinical features with Covid-19 infection especially who suffered from headache, Dyspnea, Anosmia and Ageusia Table 3.
Table 3: Clinical features of Covid-19 patients
Signs and Symptoms | Mild (n) | Moderate (n) | Severe (n) | Total (n) | p. value |
Cough | 27 (34.62) | 26 (33.33) | 25 (32.05) | 78 (100) | 0.36 |
Headache | 36 (52.17) | 19 (27.54) | 14 (20.29) | 69 (100) | <0.001 |
Body ache | 24 (39.34) | 15 (24.59) | 22 (36.07) | 61 (100) | 0.21 |
Fever | 20 (35.71) | 18 (32.14) | 18 (32.14) | 56 (100) | 0.82 |
Sneezing | 13 (61.90) | 5 (23.81) | 3 (14.29) | 21 (100) | 0.03 |
Abdominal pain | 1 (100) | 0 (0) | 0 (0) | 1 (100) | 0.44 |
Diarrhea | 6 (37.5) | 4 (25) | 6 (37.5) | 16 (100) | 0.78 |
Vomiting | 1 (11.11) | 4 (44.44) | 4 (44.44) | 9 (100) | 0.21 |
Dyspnea | 0 (0) | 29 (47.54) | 32 (52.46) | 61 (100) | <0.001 |
The study demonstrated 75 percent of covid-19 patients were with positive culture (Figure 4.1) and E. faecalis represented the most isolated bacteria from by nasopharyngeal culture of covid-19 patients’ 39.74 percent, Klebsiella pneumoniae 21.79 percent, Staphylococcus aureus 14.10 percent, E. coli 10.26 percent, Pseudomonas aeruginosa and Staphylococcus epidermidis 5.13 percent and Proteus mirabilis 3.85 percent (Table 4).
Table 4: Isolated bacteria by culture
Bacterial Isolates | No. | Paecentage |
Enterococcus faecalis | 31 | 39.74 |
Klebsiella pneumoniae | 17 | 21.79 |
Staphylococcus aureus | 11 | 14.10 |
Escherichia coli | 8 | 10.26 |
Pseudomonas aeruginosa | 4 | 5.13 |
Staphylococcus epidermidis | 4 | 5.13 |
Proteus mirabilis | 3 | 3.85 |
Total | 78 | 100 |
Enterococcus faecalis is the most common bacterial isolate found in severe COVID-19 cases, making up 64.52 percent of positive cases in this group. Klebsiella pneumoniae comes next, with 64.71 percent of moderate COVID-19 patients testing positive for it. There are also different amounts of Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Staphylococcus epidermidis, and Proteus mirabilis in mild, moderate, and severe COVID-19 cases (Table 5).
Table 5: Relation Bacterial Infection with Covid-19 Severity
Bacterial Isolates | No. of +ve | Mild Covid-19 | Moderate Covid-19 | Severe Covid-19 |
Enterococcus faecalis | 31 | 3 (9.68) | 8 (25.81) | 20 (64.52) |
Klebsiella pneumoniae | 17 | 0 (0) | 6 (35.29) | 11 (64.71) |
Staphylococcus aureus | 11 | 0 (0) | 2 (18.18) | 9 (81.82) |
Escherichia coli | 8 | 1 (12.5) | 2 (25) | 5 (62.5) |
Pseudomonas aeruginosa | 4 | 0 (0) | 2 (50) | 2 (50) |
Staphylococcus epidermidis | 4 | 1 (25) | 1 (25) | 2 (50) |
Proteus mirabilis | 3 | 1 (33.33) | 1 (33.33) | 1 (33.33) |
Total | 78 | 6 (7.69) | 22 (28.21) | 50 (64.10) |
The data shown on how sensitive and resistant bacterial isolates are to antibiotics is important for understanding how well they treat infections. Cephalothin and Imipenem exhibit excellent sensitivity, indicating their potency against all tested isolates with no resistance observed. Ampicillin is very effective, but only a small number of isolates are resistant to it. But some antibiotics, like Clindamycin and Carbenicillin, have no sensitivity, which means they don't work on any of the tested isolates. This means that all of the tested isolates are 100% resistant (Table 6).
Table 6: Distribution of Antibiotics Sensitivity toward E. Faecalis Isolated Women with Vaginitis.
Antibiotics | Sensitive No. | Sensitive % | Resistance No. | Resistance % |
|---|---|---|---|---|
Cephalothin | 31 | 100 | 0 | 0 |
Imipenem | 31 | 100 | 0 | 0 |
Ampicillin | 29 | 93.55 | 2 | 6.45 |
Levofloxacin | 20 | 64.52 | 11 | 35.48 |
Ceftriaxone | 16 | 51.61 | 15 | 48.39 |
Chloramphenicol | 12 | 38.71 | 19 | 61.29 |
Cefotaxime | 8 | 25.81 | 23 | 74.19 |
CO-Trimoxazole | 8 | 25.81 | 23 | 74.19 |
Vancomycin | 6 | 19.35 | 25 | 80.65 |
Rifampicin | 5 | 16.13 | 26 | 83.87 |
Gentamycin | 5 | 16.13 | 26 | 83.87 |
Ciprofloxacin | 4 | 12.90 | 27 | 87.10 |
Amikacin | 3 | 9.68 | 28 | 90.32 |
Streptomycin | 1 | 3.23 | 30 | 96.77 |
Carbenicillin | 0 | 0 | 31 | 100 |
Clindamycin | 0 | 0 | 31 | 100 |
There is a link between the severity of the COVID-19 disease and the number of comorbidities that are present. Most of COVID-19's less-than-ideal results have been linked to the presence of cardiovascular diseases [9]. On the other hand, this could be a direct result of the heart problem, or it could be caused by other health problems that are present along with the heart problem [9]. Patients with type 2 diabetes were more likely to have a more severe case of COVID-19 [10]. It was shown that people with less control over their blood sugar had an overall higher risk of dying than those with better glucose control [9]. Chronic obstructive pulmonary disease, or COPD, has been linked to a slower progression of illness, as well as to other diseases that happen at the same time. Patients who already had COPD and were given a COVID-19 diagnosis had a four times higher chance of dying, according to the results of a meta-analysis that looked at the results of different studies done in China. For this study, the patients' smoking histories and how bad their COVID-19 symptoms were were also looked into. There was only one study that showed that smoking was linked to a severe case of COVID-19. When this research was taken out of the picture, there was no longer a strong link between smoking and severe COVID-19 illness [11]. Patients with acute respiratory distress syndrome and respiratory failure caused by the new coronavirus may have prothrombotic coagulopathy. The fact that scattered microthrombi were found in the pulmonary vasculature of people who had died from COVID-19 showed that the cause of respiratory failure was occlusion. After treatment with anticoagulant alteplase given through an IV, three people with COVID-19-related acute respiratory distress syndrome (ARDS) and respiratory failure got better by 38% to 100%. All three of the patients showed this kind of improvement. Even though the results were good, they only lasted for a short time in two of the three cases, and the patients got worse after therapy was over. More research needs to be done on anti-thrombolytic therapy to find out if the benefits seen are actually caused by the treatment and not just by chance [12]. In this study, we were able to show that an infection with SARS-CoV-2 is linked to changes in the nasopharyngeal microbiota at different stages of the disease. This gives the microbiota a microbiological signature as the infection progresses. This was done by looking at the bacteria that live in the nose and throat. First, we found that the number of anaerobes in COVID-19 patients went down, and this was true no matter how the infection showed up on the outside. These results are similar to what Edouard et al. [13] found when they looked at people with respiratory illnesses caused by viruses other than SARS-CoV-2. Based on these results, the loss of anaerobes might be a result of viral infections in the lungs. [Needs citation] Klebsiella pneumoniae was much more common in COVID-19 patients than in COVID-negative people, but firmicutes were much more common in COVID-negative people than in COVID-19 patients. These differences are the same as those found by De Maio et al. [14], who did not find statistically significant differences despite their analysis. This could be because their sample size was small, which could explain why they didn't find statistically significant differences. When we looked at COVID-19 positive patients and COVID-19 negative participants, we found that COVID-19 positive patients had more of 8 taxa in their nasopharyngeal microbiota. C. propinquum/pseudodiphtericum, S. aureus, K. pneumoniae, and E. faecalis were some of these taxa. In a recent study, it was found that these pathogens were more common in people who had respiratory infections caused by different viruses [15,16]. This means that COVID-19 may not be the only place where they are overrepresented. But a recent study done on a group of COVID-19 patients showed that Corynebacterium and Staphylococcus are the most common types of bacteria in the upper respiratory tract microbiome of COVID-19 patients. [17] have found that people with Covid-19 are more likely to get Covid-19. Ghasemi et al. [18] showed that all of the E. faecalis isolates could be killed by ampicillin. This finding fits with what we already knew. Muratani and Matsumoto did a study on urinary enterococci in Japan. Their results showed that 84.8 percent of E. faecalis strains were resistant to the antibiotic gentamicin. According to the results of several previous studies [19,20], most E. faecalis isolates were sensitive to -lactams. Garcia-Solache and Rice [21] say that enterococci are thought to be sensitive to the antibiotic vancomycin but naturally resistant to clindamycin, quinupristin-dalfopristin, cephalosporins, and aminoglycosides. In line with what we found, it was shown that the current strains of enterococci are very resistant to the antibiotic gentamycin. Because enterococcal infections are getting better at picking up mobile genetic elements, they are getting harder and harder to treat. This is a direct result of the fact that bacteria are becoming more resistant to antibiotics, even ones like vancomycin that are thought to be the last line of defense. In recent years, there has been an increase in the number of enterococci that are resistant to vancomycin. This makes immunocompromised patients more likely to get severe, long-lasting enterococcal infections [22].
The study highlights the importance of recognizing bacterial co-infections in COVID-19 patients, particularly in severe cases. Enterococcus faecalis was found to be prevalent in severe cases, emphasizing the need for targeted antibiotic therapy. Proper antibiotic stewardship is essential to combat antibiotic resistance and improve patient outcomes. Further research is warranted to better understand the interplay between viral and bacterial infections in COVID-19 patients.
Papagiannitsis, C.C. et al. “Molecular characterization of carbapenemase-producing pseudomonas aeruginosa of czech origin and evidence for clonal spread of extensively resistant sequence type 357 expressing imp-7 metallo-β-lactamase.” Antimicrobial Agents and Chemotherapy, vol. 61, no. 12, 2017, article e01811-17.
Laverde Gomez, J.A. et al. “Intra- and interspecies genomic transfer of the enterococcus faecalis pathogenicity Island.” PLoS One, vol. 6, no. 4, 2011, article e16720.
Manson, J.M. et al. “Mechanism of chromosomal transfer of enterococcus faecalis pathogenicity island, capsule, antimicrobial resistance, and other traits.” Proceedings of the National Academy of Sciences of the United States of America, vol. 107, no. 27, 2010, pp. 12269–12274.
Dos Santos Oliveira, J. et al. “Structure and physiology of giant DNA viruses.” Current Opinion in Virology, vol. 49, 2021, pp. 58–67.
Molechan, C. et al. “Molecular epidemiology of antibiotic-resistant enterococcus spp. from the farm-to-fork continuum in intensive poultry production in KwaZulu-Natal, South Africa.” Science of the Total Environment, vol. 692, 2019, pp. 868–878.
Langford, B.J. et al. “Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis.” Clinical Microbiology and Infection, vol. 26, no. 12, 2020, pp. 1622–1629.
Yam, E.L.Y. “COVID-19 will further exacerbate global antimicrobial resistance.” Journal of Travel Medicine, vol. 27, no. 6, 2020.
Eythorsson, E. et al. “Clinical spectrum of coronavirus disease 2019 in Iceland: Population-based cohort study.” BMJ, vol. 371, 2020.
Guan, W.J. et al. “Cardiovascular comorbidity and its impact on patients with COVID-19.” European Respiratory Journal, 2020.
Zhu, L. et al. “Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes.” Cell Metabolism, vol. 31, 2020, pp. 1068–1077.
Wang, D. et al. “clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China.” JAMA, vol. 323, no. 11, 2020, pp. 1061–1069.
Zhao, Q. et al. “The impact of COPD and smoking history on the severity of COVID-19: A systematic review and meta-analysis.” Journal of Medical Virology, vol. 92, no. 10, 2020, pp. 1915–1921.
Edouard, S. et al. “The nasopharyngeal microbiota in patients with viral respiratory tract infections is enriched in bacterial pathogens.” European Journal of Clinical Microbiology & Infectious Diseases, vol. 37, 2018, pp. 1725–1733.
De Maio, F. et al. “Nasopharyngeal microbiota profiling of SARS-CoV-2 infected patients.” Biology Procedures Online, vol. 22, 2020, article 18.
DeMuri, G.P. et al. “Dynamics of bacterial colonization with streptococcus pneumoniae, haemophilus influenzae, and moraxella catarrhalis during symptomatic and asymptomatic viral upper respiratory tract infection.” Clinical Infectious Diseases, vol. 66, 2018, pp. 1045–1053.
Al-Azzawy, M.A. et al. “Study of the relationship between vitamin d level and the increase in the severity of COVID-19 infection in Kirkuk city.” Medico-Legal Update, vol. 21, no. 2, 2021, pp. 1383–1387.
Lloréns-Rico, V. et al. “Clinical practices underlie COVID-19 patient respiratory microbiome composition and its interactions with the host.” Nature Communications, vol. 12, 2021, article 6243.
Ghasemi, E. et al. “Vaginal colonization and susceptibility to antibiotics of enterococci during late pregnancy in Kerman city, Iran.” Archives of Clinical Infectious Diseases, 2016.
Fernández-Fuentes, M.A. et al. “Genetic determinants of antimicrobial resistance in gram-positive bacteria from organic foods.” International Journal of Food Microbiology, vol. 172, 2014, pp. 49–56.
Chajęcka Wierzchowska, W. et al. “Enterococci from ready-to-eat food: horizontal gene transfer of antibiotic resistance genes and genotypic characterization by PCR melting profile.” Journal of the Science of Food and Agriculture, vol. 99, 2019, pp. 1172–1179.
Garcia-Vidal, C. et al. “Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study.” Clinical Microbiology and Infection, vol. 27, no. 1, 2021, pp. 83–88.
Hamzah, A.M. and H.K. Kadim. “Isolation and identification of enterococcus faecalis from cow milk samples and vaginal swab from human.” Journal of Entomology and Zoology Studies, vol. 6, 2018, pp. 218–222.
