
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Background: The procedure of endoscopic retrograde cholangiopancreatography (ERCP) is a challenging one with rare postoperative complications. Although biliary plastic stent-related duodenal perforations are uncommon, they can be fatal. Treatment options for perforations of this type are varied and controversial. Case presentation: A male patient, 48 years old, with severe pain in the abdomen was referred to Dr. Moewardi Hospital. For one day after endoscopic retrograd cholangiopancreatography (ERCP) five days ago. To hepatopancreatobiliary surgery department of Moewardi Hospital for malignant biliary obstruction due to advanced pancreatic cancer. Due to obstructed jaundice due to biliary stenosis, the patient underwent dilatation and stent placement of the bile duct. After perforation of duodenal due in to biliary peritonitis and biliary, the patients underwent duodenography, laparotomy, peritoneal lavage, and a biliodigest procedure. Conclusion: Despite the low risk of interference with complications, biliary obstruction such as pancreatitis, bleeding and fatigue may happen. Early detection or a high index of suspection lead to effective intervention. Stent migration can lead to duodenal perforation, which can lead to morbidity and mortality if treatment is delayed.
Background
Endoscopic intervention becomes a standard feature of complicated biliary disease management. The endoscopic retrograde cholangiopancreatography (ERCP) operation is widely tto explore abnormalities of common bile duct, pancreatic ducts, and ampula. ERCP also perform some therapeutic interventions [1]. Endoscopy diagnostic procedures have developed beyond ERCP, which allow the implantation of prostheses and stents to bypass biliary blockage as both palliative and therapeutic operations [2]. Despite the fact that procedure is minimally invasive, these procedures may cause some consequences. This operation is regrarded as the most invasive and difficult endoscopic procedure. This operation has a 1% fatality rate and a 15% complication rate [3]. ERCP could also cause pancreatitis, bleeding, and duodenal damage. Besides, biliary stent migration after ERCP had been documented in previous report (reference?). Dislocation and migration were mentioned in previous research as late complications, which occur in 7% (0–40%) of endoscopic stenting patients [4,5].
Recent development of bile duct stent, also known as proximal migration, was revealed in biliary obstruction. Although the procedure was technically difficult, it could be corrected endoscopically with forceps, snare, or balloon. The stent can be replaced endoscopically in early phases of distal migration. Early endoscopically accessible cases could be treated with endoscopy. The stent can pass naturally in the majority of cases through the intestinal wall's contractions and distensibility. This mechanism might lead to bowel obstruction or perforation as a result of distal migration, which necessitating surgical intervention. These complications were considered have higher risk in approximately 10% of patients with benign biliary strictures. Additionally, intestinal perforation could occur in less than 1% of migrating stents, with less than 1% mortality incidences [6]. Thus, we present a perforation of duodenal case by the relocation of plastic biliary stent, which was reported at Dr. Moewardii Hospital's hepatopancreatic biliary surgery service.
Review of Literature
The procedure of endoscopic retrograde cholangiopancreatography (ERCP) is a procedure that used by a surgeon, gastroenterologist to check condition of pancreatic ducts, ampula, and bille duct [1].
This operation is used by an endoscope specialized, a maneuverable tube that has micro camera that move through to the digestive tract from the mouth, oesophagus, until the patient’s stomach works inside the duodenum.
The tip of the endoscope has a miniaturized video camera which allows a doctor to watch a magnified view inside the gastrointestinali tracts on the monitor. The pancreatic and bile duct images can be received by injectingi a radiolucent agent into the agent reach the pancreatic and bile ducts while x-rays are already in use. To perform a biopsy, a Special instrument is inserted through the endoscope, remove the stones from the organs, expand solids, insert stent (narrow tube to allows pancreatic or bile juice to send through the narrow space.). Before procedure of ERCP, you have to inform the patient to refrain from drinking and eating for et 6 hour. Depending on the characteristics of the patient and the complexity of the operation, ERCP is performed under general or deep sedation on complexity and patient of the procedure acceptable. Patients who undergo ERCP are comfortable with minimal pain during and after the procedure, and many do not remember it.Usually, ERCP is performed on an outpatient basis [1]. The target of therapeutic for procedure ERCP is the biliary tract stones.
Most of general surgeons do not have enough appropriate experience in laparoscopic ductal stone removal. Therefore, patients with gallstone who have had previous cholecystectomy at risk of surgery have benefit from medical ERCP. Ten years after the gallstones were removed, endoscopists began using ERCP with lithotripsy to remove the pancreatic stone from the duct. Control of malignancy in the biliary tree is another target for ERCP, especially in patients who are at risk for surgery or have untreated malignant stones. The ERCP procedure is also good for preoperatively procedure in patients with. borderline resection and receiving neoadjuvant chemotherapy and/or irradiation. to try to make. them resectable. The third therapeutic indication is bile leakage after hepatectomy, liver transplant, or laparoscopic cholecystectomy. Patients with abnormality like pancreatic. ascites, pancreatic duct. leaks, pseudocysts, pancreatic plural effusions, and walled-off. pancreatic necrosis. may also. undergo therapeutic. ERCP [7].
Based on difficulty, a previous study showed an evolved grading scale for ERCP change. Accepted by ASGE as part of the quality assessment document [8]. The ECRP difficulty rating is described in Table 1.
Table 1: Grading difficuty for ERCP by scale
| Grade | Biliary Procedures | Pancreatic Procedures |
| I |
|
|
| II |
|
|
| III |
|
|
NBD, Nasobiliary Drain; BII, Bilrothh II; CBD, Commonn Bile Ddut; SOM, Sphincter of Oddi Manometry.
Important aspects of patient care should be emphasized, including post-ERCP procedures, outcome information, treatment implications, and follow-up planning. This includes effective patient communication and referral to doctor. The importance of detailed procedural reporting using accepted nomenclature should be explored. The use of abbreviations should be kept to a minimum [8].
The risk of adverse events in the ERCP procedure is higher than in lower endoscopy, upper endoscopy, and pancreatitis; adverse events such as cholangitis and post-sphincterotomy hemorrhage are unique to your operation. Serious side effects such as acute cholangitis and pancreatitis may not be clinically apparent for few hours after surgery [9]. Previous studies have demonstrated patient risk factors for postoperative of ERCP pancreatitis that were determined by multivariate analysis. (Table 2).
Table 2: Patient Risk Factors for Postoperative of ERCPI Pancreatitis
| Patient-related risk factors | Odds ratio (95% confidence interval) |
| Prior post-ERCP pancreatitis | 8.7 (3.2-23.86) |
| Female sex | 3.5 (1.1-10.6) |
| Previous recurrent pancreatitis | 2.46 (1.93-3.12) |
| Suspected sphincter of Oddi dysfunction | 1.91 (1.37-2.65) |
Younger patient age (<40 years old) 30 vs 70 years old | 1.8 (1.27-2.59) 2.14 (1.41 3.25) |
| Absence of chronic pancreatitis | 1.87 (1.003.48) |
| Normal serum bilirubin | 1.89 (1.222.93) |
Apart from pancreatitis, sepsis and cholangitis are also known side effects associated with the ERCP procedure, occurring in 0.5% to 3% of cases. Cholecystitis after ERCP should also be admitted early and great diagnosed as acute cholangitis. The Patients may present with abdominal pain, fever, a positive Murphy's sign, and leukocytosis. It can result in duodenal infection after ECRP. Perforation can also occur and be classified as duodenal wall, periampullary, instrument-related, or stent-related perforation. Cardiopulmonary side effects may also occur post-ERCP procedure, including hypotension, hypoxia, aspiration, and cardiac arrhythmias [10].
Case Presentation
A male patient, 48 years old was admitted to hospital after five days high fever and abdominal pain. He also complained of a history of jaundice associated with losing his wight and dark urine. The patient had no concomitant diseases. On physical examination, the patient is febrile, has tachycardia, and is otherwise normal, with a systolic and diastolic blood pressure of 110/70 mmHg and a heart rate of 110 bpm, respectively. The patient had icteric sclerae and generalized jaundice. Thorax and abdominal examinations revealed no abnormalities. The patient was referred to the hepatopancreatic biliary unit of Dr. Moevardi Hospital and was diagnosed with complications due to an advanced stage of pancreatic cancer.
The patient underwent ERCP with placement of an 8.5 Fr 9 cm flat plastic stent (Boston Scientific, FleximaTM,). After intervention, the patient was admitted to the ward. She complained of fever and upper abdominal pain the next day. Abdominal computed tomography (CT) was performed and showed a fragmented bladder obstruction, the distal end of which breached the lower wall of the third part of the gallbladder and extended into the abdominal cavity and duodenum. The ERCP procedure was repeated. According to endoscopic scans, the proximal tip of the previously implanted plastic stent is in the distal tip and the bile duct has penetrated the wall of duodenal opposite your papilla. The plastic stent was pulled out of the duodenum wall using rat dental forceps. The patient was discharged on postoperative day 10 after receiving gastric emptying, antibiotics, and somatostatin.
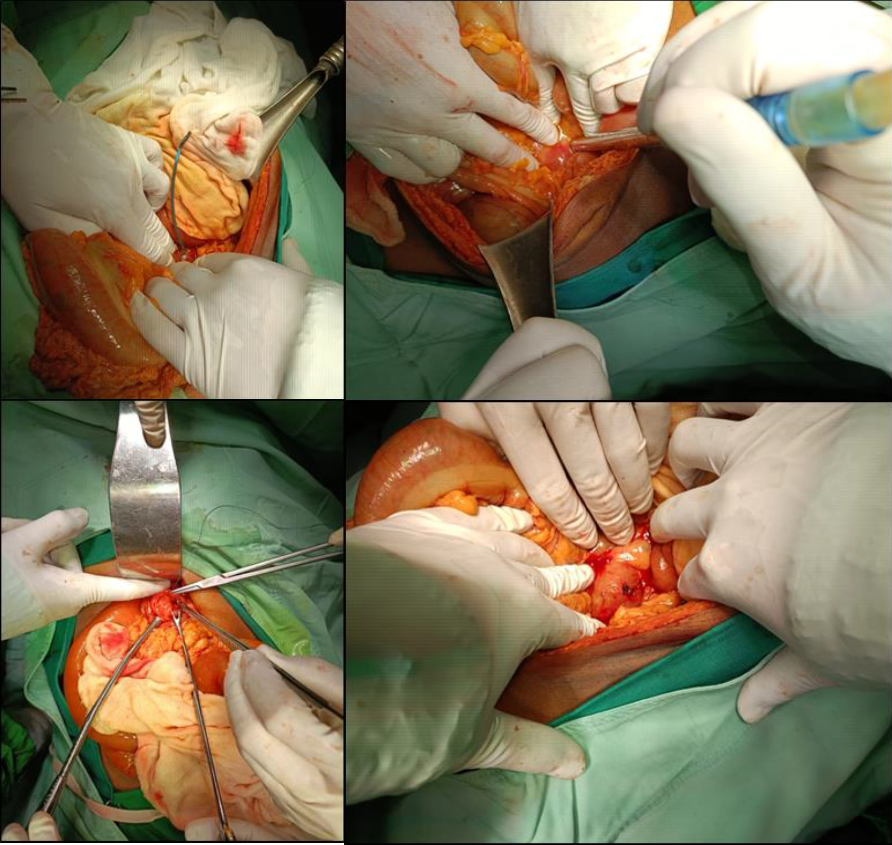
Figure 1: Casee Presentation a Male Patient Admitted in Hospital after Five Days High Fever and Abdominal Pain
The operation for obstructive jaundice caused by benign or malignant strictures is endoscopic retrograde cholangiopancreatography with biliary stenting. It is generally thought to cause less morbidity than surgery, and it can also be used to cure postoperative biliary leakage, avoiding the need for reoperation. Stent migration can occur in up to 10% of patients who have biliary stenting, with less than 1% of cases resulting in death [6,11]. Intraperitoneal or retroperitoneal perforations may result from a distally migrated stent [3]. Symptoms usually appear early in the course of the disease. In our case, the patient presented with upper stomach pain and fever. Patients with benign biliary pathologies are more likely to migrate, probably because strictures weaken as ductal inflammation and mucosal edema resolve. Tumor growth in malignant strictures may potentially aid in stent anchoring and migration prevention. Proximal biliary stent migration has been linked to malignant strictures, bigger diameter stents, and short stents [12]. Stent-related parameters like the stent's kind, length, and caliber can all help to reduce the chance of migration. Early on after biliary stenting, distaltic migration and accompanying duodenal injuries are more likely to occur. Stent diameter and length may also have an impact [13].
Upper gastrointestinal endoscopy and ERCP can be used to extract the majority of migrating stents. If the stent migrates to the intestines, 43% of the time it will pass on its own. Biliary stents can occasionally impact and perforate fixed intestinal segments like the duodenum or the right side of the colon, as well as other places that have been fixed due to adhesions from a prior procedure. Biloma or biliary peritonitis can result from an intestinal perforation. Surgery is the therapy of choice when this is suspected [4,6].
A similar case was reported in a case report by Perez et al. where duodenal perforations occurred secondary to stent migration after ERCP for hepatobiliary tuberculosis in a young patient. Unfortunately, in this case, due to the delay in early recognition, the problem has progressed to pancreatitis [4].
In conclusion, despite the minimal risk of biliary obstruction interventional procedures, problems like pancreatitis, bleeding, and perforation can develop. Early detection and a high level of suspicion result in effective early intervention. Stent migration can result in duodenal perforation, which can be fatal if treatment is delayed.
Baiu, I. and B. Visser. “Endoscopic retrograde cholangiopancreatography.” JAMA, vol. 320, no. 19, 2018, pp. 2050, doi:10.1001/jama.2018.14481.
Dumonceau, J.M. et al. “Endoscopic biliary stenting: Indications, choice of stents, and results: European society of gastrointestinal endoscopy (ESGE) clinical guideline—updated october 2017.” Endoscopy, vol. 50, no. 9, 2018, pp. 910–930.
Wang, X. et al. “Duodenal perforations secondary to a migrated biliary plastic stent successfully treated by endoscope: Case report and review of the literature.” BMC Gastroenterology, vol. 20, no. 1, 2020, pp. 1–7.
Perez, A.R. et al. “Duodenal perforation secondary to stent migration after ercp for hepatobiliary tuberculosis: Case report of a lethal complication in a young patient.” International Journal of Surgery Case Reports, vol. 88, 2021, article 106510, doi:10.1016/j.ijscr.2021.106510.
Issa, H. “Migration of a biliary stent causing duodenal perforation and biliary peritonitis.” World Journal of Gastrointestinal Endoscopy, vol. 5, no. 10, 2013, pp. 523.
Bagul, A. et al. “A review of problems following insertion of biliary stents illustrated by an unusual complication.” The Annals of the Royal College of Surgeons of England, vol. 92, no. 4, 2010, pp. e27–e31.
Kozarek, R.A. “The past, present, and future of endoscopic retrograde cholangiopancreatography.” Gastroenterology & Hepatology, vol. 13, no. 10, 2017, pp. 620–622.
Jorgensen, J. et al. “Endoscopic retrograde cholangiopancreatography (ERCP): Core curriculum.” Gastrointestinal Endoscopy, vol. 83, no. 2, 2016, pp. 279–289, doi:10.1016/j.gie.2015.11.006.
Lichtenstein, D.R. et al. “Sedation and anesthesia in GI endoscopy.” Gastrointestinal Endoscopy, vol. 68, no. 5, 2008, pp. 815–826.
Chandrasekhara, V. et al. “Adverse events associated with ERCP.” Gastrointestinal Endoscopy, vol. 85, no. 1, 2017, pp. 32–47, doi:10.1016/j.gie.2016.06.051.
Agha, R.A. et al. “The SCARE 2020 guideline: Updating consensus surgical case report (SCARE) guidelines.” International Journal of Surgery, vol. 84, 2020, pp. 226–230.
Yuan, X.L. et al. “Risk factors for distal migration of biliary plastic stents and related duodenal injury.” Surgical Endoscopy, vol. 34, no. 4, 2020, pp. 1722–1728, doi:10.1007/s00464-019-06957-x.
Arhan, M. et al. “Migration of biliary plastic stents: experience of a tertiary center.” Surgical Endoscopy, vol. 23, no. 4, 2009, pp. 769–775.
