
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Objective: To study serum T3, T4 and TSH levels in patients admitted in ICU and its correlation with the outcome. Methodology: This prospective observational study was conducted in an ICU of tertiary care center in western India. Results: Mean T3 level was 0.534 ng/mL in expired patient while it was 0.724 ng/ml in survived patients (p = 0.005). The patients having low T3 levels, days of ventilator requirement and inotropes support was more (p = 0.001 and p = 0.004). In patients with T4 level less than normal i.e., <5.1 µg/dl, odds ratio was 3.148. Mean days of inotropes in patients with T4 <5.1 µg/dL was higher than patients with normal T4 (p = 0.02). Conclusion: Low T3 level was significantly associated with high mortality, longer days of ventilator and inotropic support. Low T4 levels significantly correlated with the high mortality and longer duration of inotropic support.
The thyroid gland is the endocrine gland responsible for producing thyroid hormone, a regulator of growth, development and basal metabolic rate and calcitonin, a regulator of calcium homeostasis. Any dysfunction in the thyroid gland or its regulation can lead to abnormalities in the levels of its hormones that can lead to hypo or hyperthyroidism. Abnormal level of thyroid hormone in the setting of a Non-Thyroidal Illness (NTI) without preexisting hypothalamic-pituitary and/or thyroid gland dysfunction is called sick euthyroid syndrome [1-3]. A decreased level of serum total triiodothyronine (T3) is the most common thyroid function abnormality in patients with acute illness [4] and can be detected within 2 hours after the onset of severe physical stress [5]. As the severity of illness progresses, there is gradual development of a more complex syndrome associated with low levels of T3 and thyroxine (T4) [6,7]. Levels of thyrotropin (TSH) remain unchanged or slightly reduced. The conversion of the pro-hormone (Thyroxine, T4) to the active form is reduced due to decreased 5’-deiodinase activity peripherally and production of reverse T3 (rT3), the inactive metabolite, is increased. These thyroid hormone changes may be mediated in part by cytokines or other inflammatory mediators, acting at the level of the hypothalamus and pituitary, the thyroid gland and the hepatic deiodinase system, as well as on binding of thyroxine to Thyroid Binding Globulin (TBG). It remains unresolved whether the hormone responses in the sick euthyroid syndrome represent part of an adaptive response, which lowers tissue energy requirements in the face of systemic illness, or a maladaptive response, which induces damaging tissue hypothyroidism. The more profound the changes in hormone pattern, the poorer the prognosis [8,9].
Aims and Objectives
To study serum T3, T4 and TSH levels in patients admitted in ICU and its correlation with the outcome which was evaluated by duration of ICU stay, days of ventilator support, duration of inotropic support and overall mortality.
This prospective observational study was conducted in a tertiary care center and following criteria were used for enrollment of the patients.
Inclusion Criteria
Age more than 18 years
Newly admitted patients in medical ICU
Exclusion Criteria
Patients having past or family history of any thyroid illness
Patients taking any prior medication interacting with thyroid function. For example, Amiodarone, glucocorticoids, retinoid, somatostatin analogues
Past history of any malignancy or radiation therapy or chemotherapy
Pregnant patients
The sampling technique used was purposive sampling of patients admitted in medical ICU. A structured clinical proforma was used for data collection in which all pertinent details of the patients were recorded. Serum T3, T4 and TSH were sent in all the patients on admission. Apart from these, other routine and special investigations like cultures, USG, CT scans etc. were done according to the need of the patients. Data was entered in MS EXCEL Spread sheet and analyzed with the help of Open-epi version 3.01 updated 2013/04/06 & SPSS software version 20. The statistical analysis was done by appropriate statistical method.
Most of the patients (24%) were between the age of 28-37 years and mean age of the study population was 42.6±10.09 years. Total 32 (64%) patients were males and 18 (36%) were females. In the present study, 26 (52%) patients of the total study population eventually expired and rest 24 (48%) survived. Total 38 (76%) of 50 patients were detected with low levels of thyroxin i.e. T3 less than 0.8 ng/ml and mean T3 level was 0.633 ng/mL (Table 1).
Table 1: Mean Levels of Thyroid Hormones and its Correlation with Mortality
| Mean level (ng/ml) | Expired patients (n = 24) | Survived Patients (n = 26) | p-value |
| T3 | 0.534±0.281 | 0.724±0.171 | 0.005 |
| T4 | 4.680±2.132 | 5.476±1.827 | 0.161 |
| TSH | 2.113±2.695 | 3.573±2.705 | 0.062 |
Mean T3, T4 and TSH levels were evaluated in expired and survived patients. Mean T3 level was 0.534 ng/mL in expired patient while it was 0.724 ng/mL in survived patients. This difference was clinically significant (p-value = 0.005). Mean T4 and TSH levels in expired patients were less than the survived patients but it was statistically not significant (p-value = 0.161 and p-value = 0.062) (Table 2).
Table 2: Normal and Low Values of Thyroid Hormone and its Correlation with Mortality
| Variables | Expired patients (n = 24) | Survived patients (n = 26) | Odds Ratio | p-value |
| T3<0.8 ng/mL | 22 (92%) | 16 (62%) | 6.875 | 0.030 |
| T3>0.8 ng/mL | 2 (8%) | 10 (38%) | ||
| T4<5.1 µg/dL | 15 (60%) | 9 (35%) | 3.148 | 0.048 |
| T4>5.1 µg/dL | 9 (40%) | 17 (65%) | ||
| TSH <0.27 µIU/mL | 6 (25%) | 0 (0%) | 0.016 | |
| TSH>0.27 µIU/mL | 18 (75%) | 26 (100%) |
Normal values: T3-0.8 to 2 ng/ml, T4-5.1 to 14.1 µg/dl, TSH:0.27 to 4.2 µIU/ml
In the Table 2, patients were divided according to normal or decreased values of thyroid hormones. There was statistically significant correlation between T3 levels and mortality of the patients in present study group (p = 0.03). Odds ratio was 6.875 which suggests that there was 6.875 times more chances of death if T3 level was lower than normal i.e., <0.8 ng/ml (Figure 1).
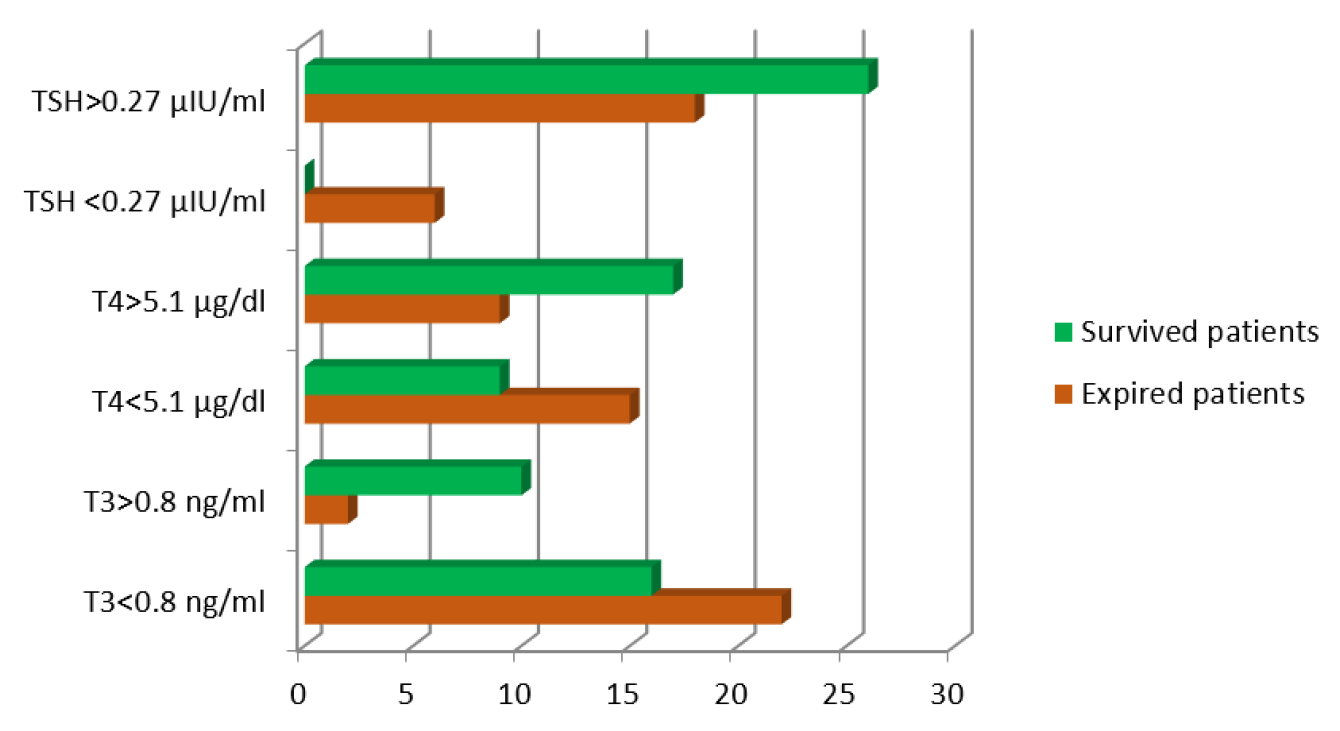
Figure 1: Normal and Low Values of Thyroid Hormone and its Correlation with Mortality
On correlating the T4 levels and mortality of the patients, it was found to be significant (p = 0.04). Odds ratio was 3.148 which suggests that there was 3.148 times more chances of mortality if T4 level was less than normal i.e., <5.1 µg/dL.
Similarly, correlation between TSH levels and mortality was significant in the present study (p = 0.016). Odds ratio was 86.67 which suggests that there was 86.67 times more chances of death if TSH level was less than normal i.e., <0.27 µIU/mL.
Receiver operating characteristic (ROC) curves were constructed and the area under the ROC curve was calculated to assess the usefulness of T3 level for predicting the in-hospital outcome. Best cutoff values were identified by ROC curves with Youden index. The best cut off value for T3 was 0.68 with sensitivity of 87.5% and specificity of 76.9% for predicating mortality.
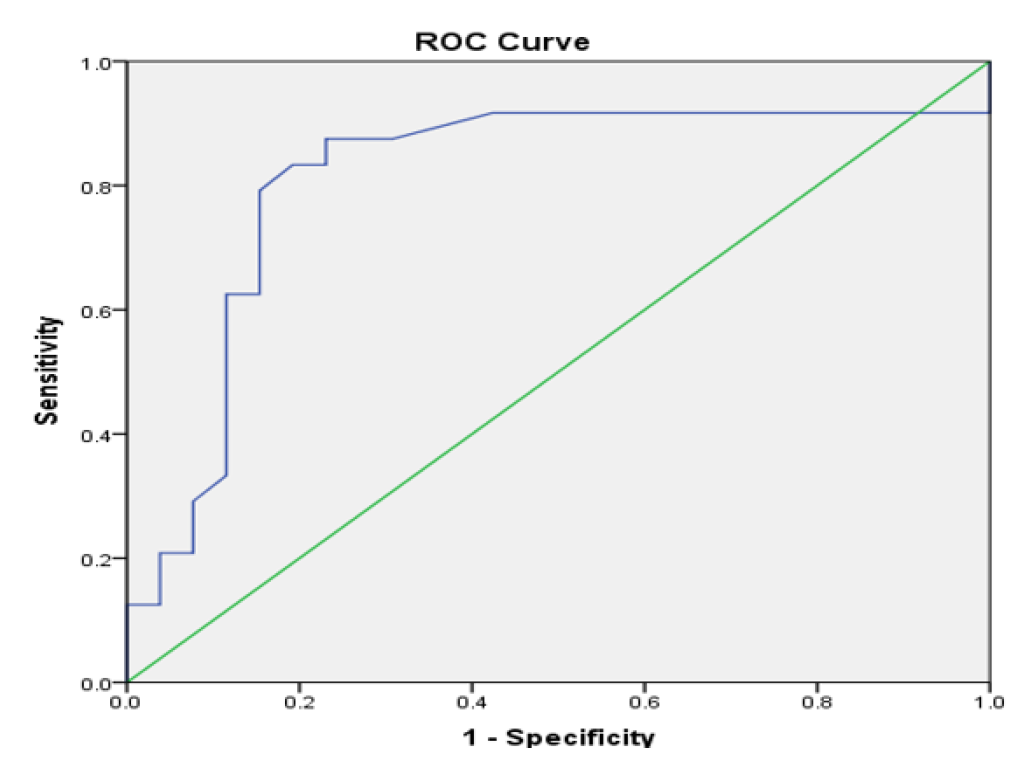
Figure 2: ROC Curve
The Table 3, shows that, median days of ventilator required by the patients with T3<0.8ng/mL and T3>0.8 ng/mL was 3 days. 50% of patients with T3<0.8 ng/mL were having days of ventilator requirement between 1 to 6 days, 25% were having more than 6 and 25% were having less than 1 day. 50 % of the patients having T3>0.8ng/mL were having days of ventilator requirement between 1.75 to 4.5 days, 25% were having more than 4.5 days and 25% were having less than 1.75 days. Mann Whitney test was applied with confidence interval 95 %. This shows that in patients having low T3 levels, the days of ventilator requirement was more (p = 0.001).
Similarly, we tried to correlate levels of T4 and TSH and median days on ventilator but statistically it was not significant (p = 0.243 and p = 0.439).
Table 3: Normal and Low Values of Thyroid Hormone and its Correlation with Days on Ventilator
| Thyroid Hormone Levels | Median Days on ventilator | p value |
| T3 <0.8ng/ml | 3 (1-6) | 0.001 |
| T3 >0.8ng/ml | 3 (1.75-4.5) | |
| T4 < 5.1 µg/dl | 3 (0.75-6.25) | 0.243 |
| T4 >5.1 µg/dl | 3 (1.25-6) | |
| TSH < 0.27 µIU/ml | 2 (1-3) | 0.439 |
| TSH > 0.27 µIU/ml | 3 (1-6) |
Normal values: T3-0.8 to 2 ng/ml, T4-5.1 to 14.1 µg/dl, TSH:0.27 to 4.2 µIU/ml
Table 4 shows that mean days of inotropes in patients with T3 <0.8ng/ml was 2.07 days and those with T3 >0.8ng/ml was 0.67 days (p = 0.004). Independent t test was applied with 95% confidence interval. Similarly, mean days of inotropes in patients with T4 <5.1 µg/dl was higher than that with T4 >5.1 µg/dl which was statistically significant (p = 0.02). Correlation between levels of TSH and mean days of inotropes was statistically not significant (p = 0.64).
When we tried to evaluate correlation between thyroid hormone levels and mean days of ICU stay, there was no significant correlation between T3, T4, TSH levels and days of ICU stay. (p = 0.081, p = 0.536, p = 0.782).
Table 4: Normal and Low Values of Thyroid Hormone and its Correlation with Days of Inotropes
| T3 Levels | Number of patients (n=50) | Mean days of inotropes | SD | p value |
| T3<0.8 ng/ml | 38 (76%) | 2.07 | 2.55 | 0.004 |
| T3>0.8 ng/ml | 12 (34%) | 0.67 | 1.07 | |
| T4< 5.1µg/dl | 24 (48%) | 2.45 | 2.63 | 0.020 |
| T4> 5.1µg/dl | 26 (52%) | 1.08 | 1.95 | |
| TSH<0.27µIU/ml | 6 (12%) | 2.17 | 2.64 | 0.641 |
| TSH>0.27µIU/ml | 44 (88%) | 1.68 | 2.34 |
In the present study low T3 was the commonest abnormality which was seen. It was associated with normal or low T4 and TSH levels which occurs typically in Nonthyroidal Illness Syndrome (NTI). Mean and Low T3 levels well correlated with the mortality in the study group. Patients with low T3 require prolonged ventilation and inotropes compare to the patients with normal T3 levels. As T3 is a metabolically active form of thyroid hormone and it is first to deplete in acute critical illness, that may the reason for its significant correlation with the outcome of the patients. In a study done by Sasi Sekhar TVD et al. [10], the mean T3 levels in patients who expired was 0.40 ng/ml and those who survived was 0.63 ng/ml which was statistically significant (p = 0.0001). In another study done by Kim JG. et al. [11] there was a significant correlation between T3 levels and mortality (p = 0.01) which correlates with the findings of present study.
Mean T4 levels did not significantly correlate (p = 0.161) with mortality in the present study. In a study done by Suresh et al. [12], there was no significant correlation between T4 levels and mortality (p = 0.8091). Similar findings were shown in a study done by Sasi Sekhar TVD et al. (p = 0.65) [10]. In the present study Low T4 level was associated with increase mortality with odds ratio of 3.148 which suggest that there was 3.148 times more chances of death in the patients with low T4 levels than the patients with normal value of T4 (p = 0.48). In the first few days of critical illness T4 level is either normal or mildly decreased [13]. It’s in the chronic phase of the critical illness that T4 level starts decreasing because of which mean T4 level may not be correlating with the mortality but low T4 is correlating significantly with the mortality. Low T4 level well correlated with the days of inotropes requirement (p = 0.20) but was not associated with increase days of ventilation (p = 0.243).
Mean TSH level did not correlate with the mortality in the present study (p = 0.062). But Low TSH level was associated with increase mortality in the present study (p = 0.016). Odds ratio was 86.67 which suggests that there was 86.67 times more chances of death if TSH level was less than normal i.e. <0.27 µIU/ml. In a study done by Wang et al. [14], there was significant correlation between TSH levels and mortality in ICU patients (p = 0.002). In chronic phase of critical illness TRH released by hypothalamus is decreased, which in turn leads to decrease level of TSH and thyroid hormones which may lead to increase mortality in critically ill patients. This decrease in TRH level from hypothalamus is because of certain cytokines like tumor necrosis factor-alpha, interleukin1 and interleukin 6. In the present study low TSH levels did not correlate significantly with the days of ventilation, inotropes support and ICU stay.
In the present study most, common abnormality was low T3 level. Mean T3 level correlated well with the mortality (p = 0.005). Low T3 level was significantly associated with high mortality, longer days of ventilator and inotropic support but did not correlate with duration of ICU stay. Mean T4 level did not correlate with the mortality but low T4 levels significantly correlated with the high mortality (odds ratio = 3.148) and longer duration of inotropic support. There was no correlation between low T4 and days of ventilation and ICU stay. Mean TSH level did not correlate with mortality but low TSH level was associated with 86 times more deaths (odds ratio = 86.67). Low TSH level did not correlate significantly with days of ventilation, inotropes usage or ICU stay.
Limitations of the Study
The sample size of the present study was relatively small. Study did not include free T3 and free T4 levels, which according to few studies have significant correlation with the outcome of the patients. Serial T3 T4 TSH was not done, which can show the prognosis of the patients in case of rising or decreasing trend.
Way Forward
Nonthyroidal illness syndrome is a common occurrence in critically sick patients. In initial days’ decrease level of T3 levels may reduce energy expenditure to reduce catabolism but in late stages it may become maladaptive.
There is a need for good randomized control trial to establish the role of thyroid supplement in NTI in chronic critically sick patients.
Chopra, I. “Thyroid function in non-thyroid illnesses.” Annals of Internal Medicine, vol. 98, 1983, pp. 946–957. https://doi.org/10.7326/0003-4819-98-6-946
Docter, R. et al. “The sick euthyroid syndrome: changes in thyroid hormone serum parameters and hormone metabolism.” Clinical Endocrinology, vol. 39, 1993, pp. 499–518.
Sypniewski, E. “Comparative pharmacology of the thyroid hormones.” Annals of Thoracic Surgery, vol. 56, suppl. 1, 1993, pp. S2–S8.
Chopra, I.J. “Euthyroid sick syndrome: Is It a misnomer?” The Journal of Clinical Endocrinology & Metabolism, vol. 82, no. 2, February 1997, pp. 329–334. https://doi.org/10.1210/jcem.82.2.3745
Michalaki, M. et al. “Dissociation of the early decline in serum t₃ concentration and serum IL-6 rise and TNF-Alpha in non-thyroidal illness syndrome induced by abdominal surgery.” Journal of Clinical Endocrinology & Metabolism, vol. 86, 2001, pp. 4198–4205.
Wong, T.K. and J.M. Hershman. “Changes in thyroid function in nonthyroidal illness.” Trends in Endocrinology & Metabolism, vol. 3, 1992, pp. 8–12.
Chopra, I.J. “Nonthyroidal illness syndrome or Euthyroid sick syndrome?” Endocrine Practice, vol. 2, 1996, pp. 45–52. https://doi.org/10.4158/EP.2.1.45
Hamilton, M. “Prevalence and clinical implications of abnormal thyroid hormone metabolism in advanced heart failure.” Annals of Thoracic Surgery, vol. 56, suppl. 1, 1993, pp. S48–S53.
Shimoyama, N. et al. “Serum thyroid hormone levels correlate with cardiac function and ventricular tachyarrhythmia in patients with chronic heart failure.” Journal of Cardiology, vol. 23, 1993, pp. 205–213.
Sekhar, T.V.D.S. et al. “Thyroid hormone changes in critically ill patients.” International Journal of Research in Medical Sciences, vol. 6, no. 8, August 2018, pp. 2717–2727. https://doi.org/10.18203/2320-6012.ijrms20183257
Kim, J.G. et al. “The value of decreased thyroid hormone for predicting mortality in adult septic patients: A systematic review and meta-analysis.” Scientific Reports, vol. 8, no. 1, September 2018, pp. 14137. https://doi.org/10.1038/s41598-018-32543
Suresh, M. et al. “Thyroid dysfunction in critically ill patients in a tertiary care hospital in Sikkim, India.” Thyroid Research and Practice, vol. 14, 2017, pp. 58–62.
Van den Berghe, G. “Non-thyroidal illness in the ICU: A syndrome with different faces.” Thyroid, vol. 24, no. 10, 2014.
Wang, Y. et al. “Critical Illness-related changes in thyroid hormone levels.” Critical Care, vol. 16, 2012, pp. R11.
