
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
The trend in the increasing co-occurrence of type 2 diabetes mellitus, obesity and Chronic Kidney Disease (CKD) is a significant clinical dilemma because of the relational effects on cardiovascular and renal health. Stage 3 CKD patients are especially susceptible, as deteriorating kidney performance leads to a higher risk of adverse cardiorenal outcomes. Over the last few years, Glucagon-Like Peptide-1 (GLP-1) receptor agonists have proved to be promising therapeutic agents that have the potential to have beyond glycaemic control benefits. The paper will discuss the cardiovascular and renal outcomes in patients with type 2 diabetes and stage 3 CKD who are receiving GLP-1 receptor agonists. The databases utilized included Google Scholar and PubMed to carry out a systematic review of recent clinical trials and peer-reviewed studies. Data indicate that GLP-1 receptor agonists are likely to have a distinct role in major adverse cardiovascular events, such as myocardial infarction and stroke and provide protective renal function in terms of decreased albuminuria and a slower rate of decline in estimated Glomerular Filtration Rate (eGFR). The overall implications of the findings are that the GLP-1 receptor agonists can provide significant cardiorenal benefits to this high-risk patient population. Their inclusion in treatment approaches can enhance the approaches in the long term, though more studies are required before long-term safety and effectiveness can be guaranteed.
The increased prevalence of Type 2 Diabetes mellitus (T2DM), obesity and Chronic Kidney Disease (CKD) throughout the globe has become one of the major issues in public health that are often comorbid and reinforce each other, complicating the other conditions. In its turn, obesity is the main driving force behind the emergence and progression of T2DM due to its impact on the development of insulin resistance, persistence of inflammation and metabolic imbalances [1,2]. Obesity has also been on the increase in the global community, hence making a direct contribution towards the global rise in the burden of mortality from diabetes and its complications [3].
T2DM is a multifaceted metabolic condition, which is also marked by the impairment of insulin secretion and resistance, resulting in chronic hyperglycaemia and vascular complications over the long term [4,5]. One of the most significant of these complications is CKD, which impacts a significant percentage of diabetic patients. It has been shown that many patients with T2DM develop stage 3 CKD when kidney clearance is stable, but when there is moderate loss of kidney function, it becomes obvious and the risks involved are more pronounced [6]. At this level, patients are more susceptible to renal disease as well as cardiovascular occurrences.
The cardiovascular disease, cardio-renal interrelation has been frequently referred to as a cardiorenal continuum in which the dysfunction of either organ system promotes dysfunction of the other [7]. This bilateral load considerably elevates the morbidity and mortality of the affected people. Conventional treatment methods have largely concentrated upon glycaemic control; nevertheless, new developments show that more metabolic and cardiorenal pathways must be tackled to enhance patient outcomes [8,9].
In this regard, Glucagon-Like Peptide-1 (GLP-1) receptor agonists are eliciting more and more attention because of their multiple therapeutic effects. Other than the glucose-reducing action, these agents have been shown to be potentially useful in weight reduction, cardiovascular protective and renal protective roles [10,11]. They play their role in increasing insulin release, reducing glucagon suppression and addressing the appetite, which makes them especially effective in the presence of T2DM in obese patients [12].
Problem Statement
Although there is progress in the management of diabetes, individuals who have co-occurring obesity and stage 3 CKD are still reporting poor clinical outcomes. Traditional treatments fail to sufficiently meet the cardiovascular and renal risk problems, which occur in this group. Although newer classes of drugs like Sodium-Glucose Co-Transporter 2 (SGLT2) inhibitors have been promising, it is still necessary to consider other or additional therapies that can offer overall cardiorenal protection [8].
Aim of the Study
This paper seeks to define the effect of GLP-1 receptor agonists on cardiovascular and renal outcomes among obese individuals with type 2 diabetes mellitus and chronic kidney disease (stage 3).
Research Questions
This research intends to answer important questions on the therapeutic value of GLP-1 receptor agonists in a high-risk patient group. In particular, it reviews the question of whether these agents may enhance cardiovascular outcomes in obese patients with Type 2 Diabetes Mellitus (T2DM) and stage 3 Chronic Kidney Disease (CKD). Also, the research delves into how far GLP-1 receptor agonists affect renal performance and the development of kidney disease. Lastly, it also assesses the suitability of these medications as a feasible and effective solution to integrated cardiorenal risk management in practice.
Significance of the Study
Research into the even wider impacts of GLP-1 receptor agonists is essential to facilitating the best treatment approaches for populations at high risk. The present study will help to make a more global assessment of therapeutic efficacy, not based on glycaemic control but on cardiorenal outcomes. The results could inform clinical decision-making processes and lead to future studies to enhance long-term outcomes of T2DM patients with obesity and CKD.
Overview of Type 2 Diabetes Mellitus and Obesity: Type 2 Diabetes Mellitus (T2DM) and obesity are two metabolic diseases that are tightly linked with each other and that have become epidemic worldwide. The prevalence of obesity, which is an excessive buildup of body fat, plays a significant role in the development of insulin resistance, one of the main underlying factors in the occurrence of T2DM [2,13]. It is a complicated pathophysiological connection between these disorders, including chronic, low-grade inflammation, secretion of adipokines and an imbalance in energy metabolism [14]. All these aspects damage the insulin signal transduction, resulting in chronic hyperglycaemia and systemic metabolic failure.
Over the last few years, the rate of obesity has grown exponentially and this further increases the burden of T2DM and complications thereof [3]. Clinical practice has highlighted the significance of weight control towards minimizing risks associated with diabetes, but permanent weight loss is not easily attained by most patients [15]. Additionally, lifestyle measures, like diet and exercise, though effective, tend to have inconsistent responses in terms of their effects on patients, contingent on the adherence of patients and metabolic aspects [16]. The importance of pharmacological treatments needed to address glycaemic regulation and weight loss as two domains has therefore been on the increase.
T2DM in itself is a multifactorial disease with progressive 2-cell dysfunction as well as insulin resistance [4]. The disease is associated with a combination of microvascular and macrovascular complications, such as nephropathy, retinopathy and cardiovascular disease. There are also new findings that have brought to focus the differences in disease development in relation to demographic and biological aspects, including sex differences and early-onset diabetes, which could affect treatment results [5,17].
Chronic Kidney Disease (Stage 3) in T2DM
One of the most severe complications of T2DM is Chronic Kidney Disease (CKD) and stage 3 CKD is a crucial stage of the disease. The decrease in kidney functional capacity is moderate at this stage and is usually manifested by a fall in estimated Glomerular Filtration Rate (eGFR) and by albuminuria. According to epidemiological data, a significant percentage of T2DM patients develop CKD stages 3-5, implying the prevalence of this complication [6].
Various factors, such as ineffective glycaemic control, hypertension and obesity, have an impact on the development of CKD in diabetic patients. These are associated with structural and functional alterations of the kidneys, which include glomerular hyperfiltration, fibrosis and inflammation. The changes with time result in irreversible kidney damage and increased End-Stage Renal Disease (ESRD).
Besides renal impairment, patients with stage 3 CKD have a high risk of cardiovascular complications. This is, in part, because of common risk factors such as high blood pressure and dysfunction in metabolism and the direct impacts of kidney disease on vascular conditions [7]. Dietary modifications and pharmacological therapies have proven to be more or less effective in slowing down the progression of CKD [18]. Nevertheless, there is still a necessity to have interventions that would eradicate renal and cardiovascular risks.
The Cardiorenal Connection
The cardiorenal syndrome idea highlights the bidirectional interrelations between heart and kidney performance. In T2DM and CKD patients, dysfunction in either organ may tend to worsen dysfunction in the other one in a loop of continuous progression of dysfunction. This connected pathophysiology is also caused by hemodynamic alterations, neurohormonal stimulation and systemic inflammation [7].
Recent research has made it clear that this cardiorenal axis should be targeted in the treatment. To illustrate, blood pressure-lowering interventions and enhanced metabolic control have demonstrated that they have positive effects on cardiovascular and renal outcomes. Moreover, new pharmacological agents, such as SGLT2 inhibitors, have been shown to provide considerable benefits to decrease cardiorenal risk and thereby clinically justify the combined treatment method [8,9].
GLP-1 Receptor Agonists: Mechanism and Clinical Relevance
Agonists of the Glucagon-Like Peptide-1 (GLP-1) receptor are a fairly recent group of antidiabetic agents that have demonstrated potential to deal with several issues related to T2DM. These agents replicate the activity of endogenous GLP-1, which is a hormone that is used to regulate glucose. They act by causing insulin secretion, glucagon release inhibition, slowing of the gastric emptying rate and decreasing appetite [12].
The weight loss that the GLP-1 receptor agonists develop is one of their differentiating characteristics and is important, especially among obese patients with T2DM [11]. To a great extent, this is mediated by the control of central appetite and lower caloric consumption. Moreover, there is also growing evidence that these agents could have anti-inflammatory and cardioprotective effects, which only increases their clinical utility.
The recent studies have widened the scope of GLP-1 receptor agonists that are not only focused on controlling glycaemic levels. Research has examined their possible application in fields like cognitive activity and cancer prevention, with an increased therapeutic effect suggested [1,19]. These findings are still in development, but they point to the convenience of this type of drug.
Cardiovascular Outcomes Evidence
There is growing clinical evidence of the cardiovascular benefits of GLP-1 receptor agonists in patients with T2DM. Tasks related to cardiovascular outcomes (large-scale) have been indicated to reduce the major adverse cardiovascular events, such as myocardial infarction, stroke and cardiovascular mortality rates significantly [10]. These advantages are especially applicable to patients who have inter-morphic risks like obesity and CKD.
These cardiovascular actions involve complex mechanisms, which can involve enhancement of endothelial functioning, inflammatory responses and lipid metabolism. Moreover, the body mass reduction related to the use of GLP-1 receptor agonists serves as an added benefit in promoting great cardiovascular health, which further substantiates the fact that GLP-1 receptor agonists are a universal treatment choice.
Renal Outcomes Evidence.
Besides heart improvements, GLP-1 receptor agonists have had encouraging results as far as kidney outcomes are concerned. Clinical trials show that these agents have the potential to lower the rate of albuminuria and decrease the rate of eGFR worsening, implying that they have a prophylactic effect on renal function [10]. The implications of such findings lie especially with patients who have stage 3 CKD, where early intervention can greatly affect the progression of the disease.
The renoprotective effects of GLP-1 receptor agonists are still not well understood but are believed to include increases in glycaemic regulation, decreases in oxidative stress and inflammatory pathways. GLP-1 receptor agonist can have some complementary advantages in comparison with other therapies, including SGLT2 inhibitors, which in turn could justify their combination therapy usage [8].
Summary of Key Studies
To better understand the current evidence, Table 1 summarizes selected studies relevant to obesity, T2DM, CKD and GLP-1 receptor agonists.
Table 1: Summary of Selected Literature on Cardiorenal Outcomes
| Author(s) | Year | Study Focus | Key Findings |
| Ali et al. [8] | 2024 | SGLT2 inhibitors and cardiorenal outcomes | Significant reduction in cardiovascular and renal risks |
| Barquera et al. [13] | 2024 | Obesity prevalence | Obesity is strongly linked to metabolic disorders |
| Demir et al. [4] | 2021 | T2DM mechanisms | Identified key metabolic pathways in diabetes progression |
| Giugliano et al. [10] | 2021 | GLP-1 and cardiorenal outcomes | Reduced major cardiovascular events and renal decline |
| Kampmann et al. [6] | 2023 | CKD prevalence | High incidence of CKD in diabetic populations |
| Ruilope et al. [7] | 2022 | Cardiorenal outcomes in CKD | Strong link between kidney disease and cardiovascular risk |
| Thota-Kammil et al. [11] | 2024 | GLP-1 in obesity | Demonstrated weight loss and metabolic benefits |
Research Gaps
Nevertheless, even with the increasing literature, there are a number of gaps within the literature. The majority of the behavioral researchers studied general T2DM groups and specific attention was paid to patients with stage 3 CKD. Also, there is not enough long-term safety data about GLP-1 receptor agonists in this subgroup. Comparative studies of the effectiveness of GLP-1 receptor agonists and other interventions, including SGLT2 inhibitors, on cardiorenal outcomes are also needed.
Altogether, the literature proves that GLP-1 receptor agonists have a high potential to improve cardiovascular and renal outcomes, as well as in patients with T2DM and obesity. Nevertheless, we still need further research to completely determine their place in patients with stage 3 CKD and optimize treatment programs in this high-risk group of patients.
Study Design
This paper uses a systematic narrative review method to critically analyze the current literature about the effect of GLP-1 receptor agonists on cardiorenal outcomes in obese patients with Type 2 Diabetes Mellitus (T2DM) and stage 3 Chronic Kidney Disease (CKD). Because of the diversity of study designs, populations and outcome measures of the existing literature, a narrative synthesis approach was deemed to be suitable. Such an approach is conducive to a detailed interpretation of evidence at the same time as there is the option of being flexible and incorporating evidence of clinical trials, meta-analysis of evidence and observational studies.
Data Sources and Search Strategy
Major academic databases, such as Google Scholar, PubMed and Scopus, were searched using the relevant literature to achieve a full coverage of peer-reviewed research. The search strategy included key Medical Subject Headings (MeSH) and keywords that included: GLP-1 receptor agonists, type 2 diabetes, obesity, chronic kidney disease and cardiorenal outcomes.
Refinement of the search and promotion of relevance was done using Boolean operators (AND, OR). As an example, the search for targeted studies could be done with a combination of terms like GLP-1 receptor agonists AND CKD AND cardiovascular outcomes. The search was restricted to articles written between 2020 and 2026 with the aim of including the most up-to-date and clinically applicable evidence, especially due to the dynamic nature of diabetes pharmacotherapy [8,11].
Inclusion and Exclusion Criteria
To ensure methodological rigor, clear inclusion and exclusion criteria were established (Table 2).
Criteria Type | Description |
Inclusion Criteria | Peer-reviewed journal articles published between 2020 and 2026 |
Studies involving patients with T2DM | |
Studies including obese populations | |
Research addressing stage 3 CKD or relevant renal outcomes | |
Clinical trials, meta-analyses and observational studies | |
Exclusion Criteria | Non-peer-reviewed articles and opinion papers |
Animal-only studies without clinical relevance | |
Studies not reporting cardiovascular or renal outcomes. | |
Duplicate publications |
This structured selection process ensured that only high-quality and relevant studies were included in the analysis, thereby enhancing the reliability of the findings.
Study Selection Process
The processes of study selection were done stepwise. At the beginning, there was a screening of titles and abstracts to determine possible research-relevant studies. The full-text review was applied to the articles that passed preliminary criteria. In this step, the studies were filtered as relevant to research objectives and compliance with inclusion criteria.
The duplication of the studies was excluded and only the most extensive or recent version was kept. This method minimized bias and further made sure that the review included the strongest evidence available. Commonly applied systematic methods in cardiorenal outcome research include similar meta-analyses that review diabetes research [8].
Data Extraction
The systematic and structured methodology of data extraction was pursued in order to maintain consistency, accuracy and reliability of data collection across all the chosen studies. Critical information was then noted regarding every study, like the author(s) and the year when the study was published, or the use of study design, whether randomized controlled trials or meta-analyses. Moreover, beneficial population characteristics were recorded, especially the presence of obesity and of Chronic Kidney Disease (CKD), to ensure that it is not disjointed from what this review is focused on.
In addition, information about the nature of the intervention, namely the use of GLP-1 receptor agonists, was also elicited together with important outcome measures. These were the cardiovascular ones, including myocardial infarction and stroke, as well as the renal ones, assessing the alterations of the estimated Glomerular Filtration Rate (eGFR) and the protein levels of albuminuria. The resulting coherent thematic synthesis was aided by this detailed and systematic data extraction method that allowed making meaningful comparisons across the studies and facilitated the emergence of the cohesive synthesis of the information. The data extracted was tabulated into summary tables to improve the understanding and interpretation of the data.
Data Analysis and Synthesis
The chosen studies were analyzed in terms of the thematic approach, due to which it was possible to systematize and interpret the results of the various sources. The results obtained were classified into major thematic themes, whereby they were cardiovascular outcomes, renal outcomes, metabolic effects and safety or adverse effects. This approach gave a systematic approach to the identification of relationships and trends in the literature.
Under each theme, the findings of various studies were meticulously analyzed, compared and contrasted in order to discover patterns, similarities and differences. It is important to note that the results of various meta-analyses indicated that the incidence of major cardiovascular events was correlated with a consistent decrease In Glucagon-Like Protein-1 (GLP-1) receptor agonists, whereas renal outcome was less significant, but still showed improvement in a clinically significant manner [10]. These results identify the two approaches of these agents as helpful in treating cardiovascular and renal risks.
Moreover, the comparative approach was also implemented, which entailed the investigation of the performance of GLP-1 receptor agonists against other treatment options, especially Sodium-Glucose Co-Transporter 2 (SGLT2) inhibitors. Available data point to SGLT2 inhibitors also having substantial cardiorenal effects, implying that these two types of drug could be used to produce a complementary effect [8,9]. Such a wider approach to analysis helps to better comprehend the existing treatment approaches and optimize them.
Quality Assessment
A qualitative evaluation of the quality of the methodology in the studies included was conducted to ensure the reliability and validity of the findings. The degree to which each study was critically appraised was on a number of main criteria such as the strength of study design, sufficiency of sample size, explanatory power and consistency of outcome measures and the risk of bias.
More focus was on randomized controlled trials and meta-analyses since such types of studies are usually deemed to have the best level of evidence, given the level of methodological rigor and potential to reduce bias. But the observational studies were also incorporated and the findings were appropriately taken as they presented more real-life insights, but results were construed with caution as there were chances of confounding factors. This moderation in gauging quality is consistent with a set of research-based principles and supports the overall validity of the review [4] (Figure 1).
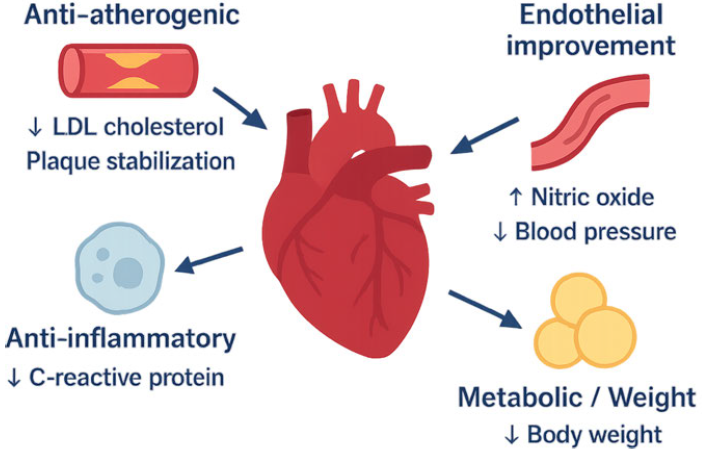
Figure 1: Flow Diagram of Study Selection Process (Adapted from PRISMA Guidelines)
This figure illustrates the systematic process of literature identification, screening, eligibility assessment and final inclusion of studies used in the review. It highlights the stepwise filtering of articles to ensure relevance and quality in the analysis of GLP-1 receptor agonists and cardiorenal outcomes.
The methodology employed in this study ensures a structured and comprehensive evaluation of existing literature on GLP-1 receptor agonists and their impact on cardiorenal outcomes. By combining systematic search strategies, clear selection criteria and thematic analysis, this approach provides a reliable foundation for interpreting the findings. The next section presents the results derived from this methodological framework.
Study Selection and Characteristics
After the systematic search and screening procedure, a list of the relevant peer-reviewed articles was added to this review. These papers consisted of randomized controlled studies, meta-analyses and observational studies that examine the impacts of GLP-1 receptor agonists in individuals with Type 2 Diabetes Mellitus (T2DM), obesity and Chronic Kidney Disease (CKD). The chosen references served as an overall foundation to assess cardiovascular and renal outcomes.
The majority of the studies included a population of adults with T2DM and many of the studies also involved populations with obesity and stage 3 CKD. The studies were mainly on various GLP-1 receptor agonists, with some studies having comparisons against other therapeutic agents, including Sodium-Glucose Co-Transporter 2 (SGLT2) inhibitors. All in all, a balanced evaluation of clinical outcomes was made possible through the diversity of study designs and populations.
Cardiovascular Outcomes
The results of several studies have consistently shown that GLP-1 receptor agonists have been effective in enhancing the cardiovascular outcomes of T2DM patients. Large-scale meta-analyses have shown evidence of major adverse cardiovascular events being significantly reduced, such as myocardial infarction, stroke and cardiovascular mortality [10]. The obtained benefits are especially applicable in obese patients, who are already at a high cardiovascular risk as a result of metabolic dysfunction.
Besides decreasing major events, GLP-1 receptor agonist studies have linked a decrease in various cardiovascular risk factors. They also comprise slight decreases in blood pressure, better lipid results and major weight loss, which helps to improve cardiovascular well-being. The overall impact of these achievements underlays the purpose of GLP-1 receptor agonists as a complex treatment choice.
Comparative analyses also make it very clear that although SGLT2 inhibitors offer an excellent cardiovascular protective effect, the GLP-1 receptor agonists are beneficial to supplement these primary effects, especially in the case of atherosclerotic events [8,9]. This implies that incorporation of these therapies could have optimum results among high-risk groups.
Renal Outcomes
By renal outcomes, the literature reviewed suggests that the effect of GLP-1 receptor agonists, overall, is positive, albeit moderate, on kidney function. A number of studies noted decreases in albuminuria, a major indicator of kidney injury and a change in the rate of estimated Glomerular Filtration Rate (eGFR) [109]. The findings are of particular significance to patients with stage CKD 3 since early intervention can help delay the development of the disease.
GLP-1 receptor agonists have been identified to exert renoprotective effects, which are thought to occur through several mechanisms such as better glycaemic regulation, anti-inflammatory and anti-hypertensive effects. Although these agents do not necessarily have as strong an effect on renal outcomes as SGLT2 inhibitors, their combined metabolic and cardiovascular effects qualify them as important in disease-wide treatment [8].
Other positive findings related to CKD-based studies underline the necessity of timely intervention in the context of slowing down the evolution of kidney diseases and minimizing the burden of complications [18,20]. This adds to the fact that there is a possibility of the GLP-1 receptor agonists being used in the treatment of patients with combined metabolic and renal issues.
Metabolic and Weight-Related Outcomes.
One of the benefits of GLP-1 receptor agonists is their influence on body weight and overall metabolic outcome. The literature reviewed indicates that they induce considerable weight loss, mainly by mouth suppression and sluggish gastric emptying [11]. This comes in especially handy in obese patients, where losing weight is a vital consideration in enhancing insulin hypersensitivity and disease burden.
Besides weight loss, GLP-1 receptor agonists help to achieve a better glycaemic control, which is a key aspect of preventing both microvascular and macrovascular complications of T2DM. These added metabolic advantages add to their usefulness as a universal option for the treatment of patients with complicated clinical histories.
Safety and Adverse Effects
GLP-1 receptor agonists have a good safety profile and adverse effects are mild/moderate in most cases. The side effects most experienced are gastrointestinal in nature, with nausea, vomiting and diarrhea, although this may decrease with time as patients get used to the medication [11].
Notably, no notable safety issues were found in patients with stage 3 CKD in the reviewed studies, but the long-term data are still scarce. It is also emerging that there are other systemic effects of GLP-1 receptor agonists, although more research is necessary to ascertain their safety issues over the long run [21] (Table 3).
Table 3: Summary of Clinical Outcomes of GLP-1 Receptor Agonists
| Outcome Category | Key Findings | Supporting Evidence |
| Cardiovascular Outcomes | Reduced risk of myocardial infarction, stroke, and mortality | [10] |
| Renal Outcomes | Reduced albuminuria and slower eGFR decline | [10,20] |
| Metabolic Effects | Significant weight loss and improved glycaemic control | [11] |
| Comparative Effectiveness | Complementary benefits with SGLT2 inhibitors | [8,9] |
| Safety Profile | Generally well tolerated with mild gastrointestinal effects | [11] |
Summary of Key Findings
Visual Summary of Findings: This Figure 2 illustrates the multidimensional impact of GLP-1 receptor agonists, highlighting their effects on cardiovascular risk reduction, renal protection, weight loss and glycaemic control. The diagram emphasizes the interconnected nature of these outcomes and their relevance in managing patients with type 2 diabetes, obesity and chronic kidney disease.
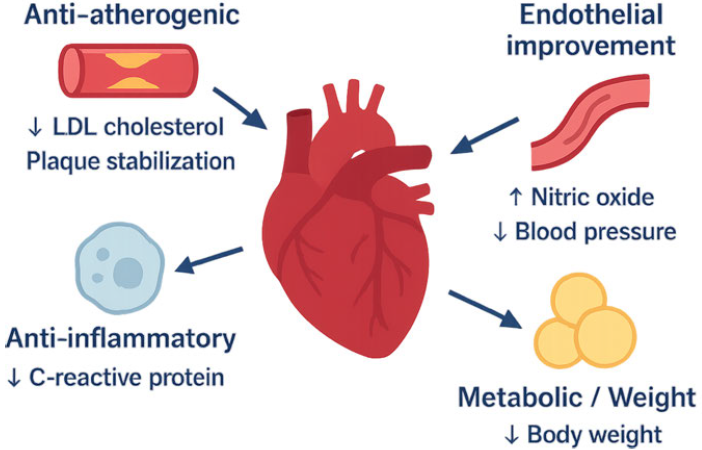
Figure 2: Effects of GLP-1 Receptor Agonists on Cardiorenal and Metabolic Outcomes
Conclusion of Results
The results of this review show that the GLP-1 receptor agonists have substantial advantages in various clinical areas, especially the enhancement of cardiovascular outcomes and renal functionality. Their moderate renoprotective properties are not as strong as some other therapeutic modalities, but the synergistic metabolic, cardiovascular and safety benefits combine to make them an important part of the multi-modality therapeutic approach in patients at high risk.
Interpretation of Findings
The results of the paper suggest the increased relevance of GLP-1 receptor agonists as a versatile treatment opportunity to treat obese individuals with type 2 Diabetes Mellitus (T2DM) and stage 3 Chronic Kidney Disease (CKD). The evidence discussed illustrates that the given agents offer valuable additional effects that go beyond glycaemic control, especially the use of cardiovascular protection and use to address renal needs. This is in line with the emerging insights suggesting that T2DM is not just a glucose metabolic disorder, but a multifaceted disorder that is characterized by interlinking metabolic, cardiovascular and renal processes [4].
Among the most notable findings is the reduction in the occurrence of major adverse cardiovascular events, which is consistent in relation to GLP-1 receptor agonists. These results are indicated by massive meta-analyses, which depict decreases in the results, including myocardial infarction, stroke and cardiovascular mortality [10]. These benefits are very clinically relevant, considering that cardiovascular disease is the primary cause of death amongst patients with T2DM and CKD. Improvements in heart activity can be related to glycaemic control, but also weight loss, better endothelial activity and anti-inflammatory.
The study results have shown that, other than cardiovascular effects, the GLP-1 receptor agonists have a protective effect on renal functioning. Though the size of renal advantage may seem to be less significant than that of cardiovascular results, the decrease of albuminuria and slower decline in the estimated Glomerular Filtration Rate (eGFR) are clinically significant, especially in patients with stage 3 CKD [10]. These impacts indicate that the introduction of GLP-1 receptor agonists at the right stage in the disease progression can prevent disease progression and the increased risk of acute kidney failure.
Comparison with Existing Literature
The result of this review shows a great deal of compatibility with the current literature on the effects of GLP-1 receptor agonists on the heart and kidneys. These results are also confirmed by other previous studies recorded to have significant cardiovascular benefits [10]. Some of the differences, however, when contrasted with other therapeutic agents, especially Sodium-Glucose Co-Transporter 2 (SGLT2) inhibitors, are evident.
The renal effect of SGLT2 inhibitors has been demonstrated to result in greater benefits, especially as relates to CKD progression reduction and the likelihood of HF hospitalization [8,9]. Conversely, GLP-1 receptor agonists seem to be more powerful in relation to atherosclerotic cardiovascular disease. The difference implies that the two drug classes might have different points of attack in the cardiorenal continuum. Consequently, the integration of the therapies may show synergies to explore a more holistic approach to disease management.
Moreover, the weight-lowering aspect of GLP-1 receptor agonists makes them exceptionally different from most other antidiabetic drugs. One of the key contributors to T2DM and CKD progression is obesity and weight loss interventions may lead to substantial changes in patient outcomes [11,13]. This is an added advantage that adds value to GLP-1 receptor agonists, especially in groups of people where obesity is an issue of concern.
Clinical Implications
The results of this research have significant clinical practice implications. To begin with, they endorse the incorporation of GLP-1 receptor agonists within an integrated approach to treating patients with T2DM, obesity and stage 3 CKD. Clinicians should not emphasize only glycaemic control; instead, they should look at therapies that cover a wider range of cardiorenal risk.
Second, there is a hypothesis that GLP-1 receptor agonists can be used earlier as a measure to delay the progression of the disease and complicated morbidities. Treatment at stage 3 CKD, instead of letting it progress to higher stages, could serve to maintain kidney function and improve the long-term outcomes. This is aligned with the existing trends in preventive and personalized medicine.
Also, complementary effects of SGLT2 inhibitors and GLP-1 receptor agonists indicate the presence of combination therapy. These agents could offer increased safeguarding against renal and cardiovascular complications by acting on various pathways. Nevertheless, more studies should be conducted to identify the best timing, dosage and patient choice of such combinations.
Strengths and Limitations
The present research has a number of strengths that increase the validity of the results. The systematic approach in literature selection made sure that its use included only relevant and high-quality studies. Furthermore, the existence of various study designs, such as randomized controlled trials and meta-analyses, was included, which gave a comprehensive picture of the evidence at hand.
Nevertheless, some limitations should also be recognized. The heterogeneity of the included studies is one of the key limitations in that different studies differed in terms of population characteristics, study design and outcome measures. Such variability can have an impact on the comparability of results and constrain the possibility of making decisive conclusions.
The other limitation is that the number of studies that targeted exclusively patients with stage 3 CKD is also relatively small. Although there were several studies that involved patients with different kidney functions, few studies presented detailed subgroup analysis on this particular group. Consequently, the results might not be sufficiently representative of the distinct clinical features of stage 3 CKD patients.
Lastly, there are limited long-term safety data available on GLP-1 receptor agonists in CKD patients. Despite its favorable safety profile, as indicated in short- to medium-term research, more studies have to be carried out in order to determine the possible long-term risks and outcomes [21].
Future Research Directions
Further studies are required to fill the gaps in the present literature. Specifically, large-scale, longitudinal and Procter and Gamble trials that include patients with stage 3 CKD in particular should be conducted to gain a clearer comprehension of the efficacy and safety of GLP-1 receptor agonists in that patient population. Also, the research on the use of combination therapy using GLP-1 agonist and SGLT2 inhibitor requirements may offer an insight into the optimal ways of managing the treatment.
How these renoprotective effects of GLP-1 receptor agonists occur should also be investigated further. A better understanding of such mechanisms can result in creating more specific treatment interventions and improved outcomes.
Conclusion of Discussion
Overall, the discussion shows that GLP-1 receptor agonists have great potential in enhancing cardiovascular and renal patient outcomes in T2DM, obese patients and patients with stage 3 CKD conditions. Their benefits have demonstrated strong evidence, although additional studies are necessary to completely determine their role in this group of high-risk persons and to maximise their clinical application.
This study aimed to assess the effects of GLP-1 receptor agonists in patients with TYPE 2 DIABETES MELLITUS (T2DM) and Chronic Kidney Disease (CKD) at stage 3 on cardiovascular and renal outcomes. According to the evidence examined, these agents have tremendous therapeutic advantages, which are not limited to conventional glycaemic control. Specifically, GLP-1 receptor agonists have been shown to uniformly lower major adverse cardiovascular incidents, such as myocardial infarction and stroke that are contributors to morbidity and mortality in this high-risk group [10].
These agents, besides their cardiovascular effects, demonstrate moderately encouraging, but promising renal protective effects. The decreases in albuminuria and the decreasing estimated Glomerular Filtration Rate (eGFR) imply that GLP-1 receptor agonists can help to slow the progression of kidney disease, particularly when used earlier in disease progression, such as at stage 3 CKD [10]. Such effects might not be as effective as those produced with certain alternative medicines, but their overall clinical implications for integrated cardiorenal management have clinical significance.
A second key conclusion is that GLP-1 receptor agonists have the potential to promote weight loss and also enhance metabolic health. This is a bonus as it improves the value of using it as a comprehensive treatment option since the three conditions are closely linked (obesity, T2DM and CKD development) [11,13]. Moreover, in most patients, they have a relatively favorable safety profile and this is why their usage should be conducted in a broad spectrum of patients, but further monitoring and long-term research should be carried out in order to establish their safety in patients with compromised kidney function [21].
In general, the results of this paper can be used to advocate for the increasing awareness of GLP-1 receptor agonists to become a significant element of contemporary diabetes treatment. The capacity of dealing with several disease pathologies, e.g., cardiovascular risk, kidney and metabolic well-being, makes them an important instrument in enhancing the long-term patient outcomes in those with complex clinical processes. Nonetheless, they need to be further studied to better establish their role, especially in patients who do not have stage 3 CKD and to determine how these facilities can be incorporated into clinical practice.
Recommendations
Depending on the results of this research, it is possible to make a number of recommendations concerning the practice and future research. To begin with, GLP-1 receptor agonists should be implemented into the treatment strategy of T2DM and stage 3 CKD obese individuals, where cardiovascular risk is a significant issue. They have been demonstrated to have numerous advantages in terms of mitigating cardiovascular events and thus are worthy of consideration in enhancing patient outcomes.
Second, early intervention must be pointed out. The use of GLP-1 receptor agonists in younger patients with CKD can delay the disease onset and minimise the risks of complications. This preventive strategy is in line with recent tendencies in preventive medicine and could have improved long-term health effects.
Third, there should be further research on combination therapy. Since agonists of GLP-1 receptors and agents of SGLT2 have complementary effects, clinicians might consider combining the agents in order to obtain a greater cardio-renal protection. Nevertheless, patient care should be carefully selected and monitored to be safe and beneficial [8,9].
Research-wise, more specific research studies on patients with stage 3 CKD are required. The pursuit of future studies should focus on both long-term estimates of efficacy and safety, in addition to attempting to delve into the mechanisms underlying the renal action of GLP-1 receptor agonists. Moreover, comparative research would also help determine the best treatment modalities by conducting comparative studies that compare various treatment combinations.
To conclude, even though the GLP-1 receptor agonists have gained significant potential, more studies and clinical trials are necessary to maximize the potential of the therapy in the treatment of T2DM, obesity and CKD.
Jones, C. et al. “GLP-1 receptor agonist Vs aspirin for primary prevention of colorectal cancer: Evidence from a real-world head-to-head comparison.” Journal of Clinical Oncology, vol. 44, no. 2 Suppl, 2026, pp. 18-18. https://doi.org/10.1200/jco.2026.44.2_suppl.18
Lara, F.V.O.de et al. “Obesity and overweight.” Medicine (Spain), vol. 14, no. 15, 2024, pp. 845-854. https://doi.org/10.1016/j.med.2024.08.001
Cross, L. “Management of obesity.” American Journal of Health-System Pharmacy, January 2025. https://doi.org/10.1093/ajhp/zxae273
Demir, S. et al. “Emerging targets in type 2 diabetes and diabetic complications.” Advanced Science, September 2021. https://doi.org/10.1002/advs.202100275
Strati, M. et al. “Early onset type 2 diabetes mellitus: an update.” Endocrine, September 2024. https://doi.org/10.1007/s12020-024-03772-w
Kampmann, J.D. et al. “Prevalence and incidence of chronic kidney disease stage 3–5 – results from KidDiCo.” BMC Nephrology, vol. 24, no. 1, 2023. https://doi.org/10.1186/s12882-023-03056-x
Ruilope, L.M. et al. “Blood pressure and cardiorenal outcomes with finerenone in chronic kidney disease in type 2 diabetes.” Hypertension, vol. 79, no. 12, 2022, pp. 2685-2695. https://doi.org/10.1161/HYPERTENSIONAHA.122.19744
Ali, M.U. et al. “The effectiveness of sodium-glucose co-transporter 2 inhibitors on cardiorenal outcomes: An updated systematic review and meta-analysis.” Cardiovascular Diabetology, December 2024. https://doi.org/10.1186/s12933-024-02154-w
Schechter, M. et al. “Cardiorenal outcomes with sodium/glucose cotransporter-2 inhibitors in patients with type 2 diabetes and low kidney risk: Real-world evidence.” Cardiovascular Diabetology, vol. 20, no. 1, 2021. https://doi.org/10.1186/s12933-021-01362-y
Giugliano, D. et al. “GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: An updated meta-analysis of eight CVOTs.” Cardiovascular Diabetology, vol. 20, no. 1, 2021. https://doi.org/10.1186/s12933-021-01366-8
Thota-Kammili, S. et al. “Glucagon-like peptide 1 receptor agonists for obesity: Efficacy, side effects and risks.” Current Treatment Options in Gastroenterology, vol. 22, no. 3, 2024, pp. 145-154. https://doi.org/10.1007/s11938-024-00452-6
Jin, F.X. et al. “Intestinal glucagon-like peptide-1: A new player associated with impaired counterregulatory responses to hypoglycaemia in type 1 diabetic mice.” World Journal of Diabetes, vol. 15, no. 8, 2024, pp. 1764-1777. https://doi.org/10.4239/wjd.v15.i8.1764
Barquera, S. et al. “Obesity in adults.” Salud Pública de México, vol. 66, no. 4, 2024, pp. 414-424. https://doi.org/10.21149/15863
Geng, J. et al. “The links between gut microbiota and obesity and obesity related diseases.” Biomedicine and Pharmacotherapy, March 2022. https://doi.org/10.1016/j.biopha.2022.112678
Haam, J.H. et al. “Diagnosis of obesity: 2022 update of clinical practice guidelines for obesity by the Korean Society for the Study of Obesity.” Journal of Obesity and Metabolic Syndrome, June 2023. https://doi.org/10.7570/jomes23031
Kanaley, J.A. et al. “Exercise/physical activity in individuals with type 2 diabetes: A consensus statement from the American College of Sports Medicine.” Medicine and Science in Sports and Exercise, vol. 54, no. 2, 2022, pp. 353-368. https://doi.org/10.1249/MSS.0000000000002800
Kautzky-Willer, A. et al. “Sex differences in type 2 diabetes.” Diabetologia, June 2023. https://doi.org/10.1007/s00125-023-05891-x
Wongmanit, P. et al. “Safety assessment of supplementation with Cymbopogon citratus Stapf. (lemongrass) extract in patients with chronic kidney disease stage 3: A preliminary 90-day prospective study.” Pharmacognosy Journal, vol. 15, no. 6, 2023, pp. 976-986. https://doi.org/10.5530/pj.2023.15.181
Ito, M. et al. “1963-LB: Prenatal treatment of glucagon-like peptide 1 agonist mitigates cognitive deficits in offspring of mothers with diabetes by modulating placental development mediated by ADGRL3.” Diabetes, vol. 73, Supplement 1, 2024. https://doi.org/10.2337/db24-1963-lb
Sarhan, I.I. et al. “Renoprotective effect of febuxostat on contrast-induced acute kidney injury in chronic kidney disease patient’s stage 3: Randomized controlled trial.” BMC Nephrology, vol. 24, no. 1, 2023. https://doi.org/10.1186/s12882-023-03114-4
Lee, I.O. et al. “Outcomes of maternal periconceptional exposure to glucagon-like peptide-1 receptor agonists: A scoping review of evidence and reporting trends.” Journal of Obstetrics and Gynaecology Canada, January 2026. https://doi.org/10.1016/j.jogc.2025.103191
