
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Labour induction and observation are a vital aspect of obstetric care with an aim of ensuring maternal and fetal outcomes optimisation. There are clinical induction methods of labour, whether pharmacological or mechanical, with indications, advantages and risks of each. Complications can be identified in time and thus interventions can be taken through effective monitoring of labour by continuous or intermittent fetal and maternal assessment. This review will compile the existing evidence related to the methods, guidelines and outcomes related to induction and monitoring of labour, best practices and difficulties in clinical practice. The focus is on the balancing of the benefits of intervention and maternal and neonatal safety. These approaches are vital and clinicians need to understand them to make evidence-based and informed decisions and enhance perinatal outcomes.
Obstetric practice depends on labour induction and observation as they try to maximise maternal and fetal outcomes with the least complications [1-2]. Induction of labour means the intentional stimulation of uterine contractions prior to the natural initiation of labour and it is usually indicated in the post-term pregnancy, premature rupture of membranes, maternal diseases and foetal jeopardy [3-4]. Adequate monitoring of the labour process is also essential, as it will give clinicians real-time evaluation of the health of a mother and a baby and allow them to monitor and treat the possible complications, such as fetal distress, extended delivery, or maternal bleeding [5-6].
There are clinical management practices of induction of labour that include a mixture of pharmacological and mechanical practices. One can find wide use of pharmacological agents (oxytocin and prostaglandins) to enhance uterine contractions, as well as mechanical ones (balloon catheters and membrane sweeping) to enhance cervical ripening [7,8]. Mother's health, fetal condition, gestational age and obstetric history of the mother are some of the factors that influence the choice of an induction method [9]. Recent papers have emphasized the necessity of personalized methods, where inappropriate or violent delivery may predispose adverse maternal eventualities, such as uterine rupture, postpartum bleeding and infection [10-12].
Labour monitoring involves fetal and maternal monitoring. The routine care provided by the maternal monitoring would mainly entail checking of vital signs, pattern of contractions and the labour progress being made with the help of partographs [13]. Fetal monitoring, on the other hand, consists of intermittent Auscultation and constant electronic fetal monitoring (EFM), allowing early detection of fetal hypoxia, acidosis, or other signs of distress [14-15]. It has been shown that structured monitoring protocols have a great impact on perinatal morbidity and mortality, causing a decrease in clinical interventions and ensuring timely ones [16-17].
Furthermore, by incorporating evidence-based recommendations, i.e., the World Health Organization (WHO) and the American College of Obstetricians and Gynecologists (ACOG) ones, the safety and effectiveness of the labour-induction and labour-monitoring practices have been enhanced [18-19]. Regardless of these developments, problems still exist, especially in resource-restricted environments where there might be a lack of access to trained staff, monitoring tools and standardized procedures [20].
This article will examine the clinical methods of induction and monitoring of labour in a comprehensive review of the existing evidence regarding methods, outcomes and best practices in the management of labour. It also emphasizes new technologies, risk management and the necessity to focus on individualized and evidence-based care in order to maximize the maternal and neonatal outcomes.
Table 1: Common Methods of Labour Induction
| Method | Type | Indications | Advantages | Limitations / Risks |
| Oxytocin infusion | Pharmacological | Augmentation of labour, post-term pregnancy | Rapid onset, controllable dose | Uterine hyperstimulation, fetal distress [11] |
| Prostaglandin E2 (PGE2) gel | Pharmacological | Cervical ripening, post-term pregnancy | Effective for an unripe cervix | Nausea, vomiting, uterine hyperstimulation [12] |
| Misoprostol (PGE1 analog) | Pharmacological | Cervical ripening, induction | Oral/vaginal route, inexpensive | Hyperstimulation, fetal heart rate changes [13] |
| Balloon catheter | Mechanical | Unfavorable cervix, contraindications to drugs | Reduced drug-related side effects | Vaginal discomfort, infection risk [14] |
| Membrane sweeping/stripping | Mechanical | Low-risk post-term pregnancy | Minimally invasive, outpatient procedure | Vaginal bleeding, discomfort [15] |
Induction of Labour
Induction of labour, artificial stimulation of uterine contractions before the onset of labour, is aimed at vaginal delivery when the continued pregnancy becomes dangerous to the mother or fetus [1,3]. It is a widespread obstetric procedure and the number varies between 20 and 30 percent in most developed nations [4]. The indications of labour induction may be classified into maternal, fetal and obstetric indications. Maternal indications comprise post-term pregnancy, preeclampsia, gestational diabetes and chorioamnionitis, whereas fetal indicators are intrauterine growth restriction, oligohydramnios, or suspected fetal compromise [5-6].
The mode of induction will be determined by the cervical readiness, maternal and fetal conditions and clinical options. Cervical ripeness is usually measured through the Bishop score, which assesses dilation, effacement, station, consistency and position of the cervix. A favourable score on Bishop is a predictor of successful induction and an unfavourable cervix could need cervical ripening before active induction [7-8].
Labour induction methods are generally classified into pharmacologicaland mechanical approaches. Pharmacological agents include prostaglandins and oxytocin, which stimulate uterine contractions and facilitate cervical ripening. Mechanical methods, such as balloon catheters and membrane sweeping, apply physical pressure to the cervix to encourage dilation [9-10]. Both approaches have proven effective, but their success and safety profiles vary depending on patient characteristics and clinical context (Table 1).
Pharmacological induction should be used in women with an unfavourable cervix (predictable and fast acting), although there is a greater risk of the birth of an underdeveloped infant in case of unmonitored induction [11-12]. In certain groups of patients, i.e., women who have undergone a cesarean section, the use of mechanical techniques is viewed as safer since the presence of prostaglandins can predispose the uterus to rupture [14].
In the recent research, the use of individual induction strategies and cervical status, incorporating both fetal and maternal factors, is important and it should be combined with available clinical resources to achieve the best outcome [16-17].Mechanical and pharmacological means could also enhance the success rate of induction with a low number of complications, especially in women with a poor cervix [18].
Monitoring of Labour
Labour monitoring is essential in the provision of maternal and fetal safety as well as in the management of clinical interventions [8,16]. Labour monitoring that is up to date requires both the regular or frequent monitoring of the mother and the fetus in order to observe any indicators of complications like fetal distress, excessive labour, or maternal bleeding [5-6]. Certain intervention measures, such as the application of partographs and electronic fetal monitoring, have been found to decrease perinatal morbidity, as well as to enhance maternal outcomes [19-20].
Maternal Monitoring
Maternal monitoring involves checking of vital signs (blood pressure, pulse, temperature), contraction of the uterus, pain intensity and progress of labour [7]. A partograph is a common instrument that is used to monitor cervical dilation, descent of the fetus and the patterns of contractions in the long run. Abnormal labour progress can be detected early to enable clinicians to intervene early enough before complications like obstructed labour or postpartum bleeding occur [17].
Table 2: Maternal and Fetal Monitoring Methods
| Monitoring Type | Method | Purpose / Indicator | Advantages | Limitations / Risks |
| Maternal Vital Signs | BP, pulse, temperature | Detect infection, preeclampsia, hemorrhage | Simple, routine, non-invasive | Does not detect fetal compromise [5] |
| Labour Progress | Partograph | Track cervical dilation and fetal descent | Standardized, early warning of abnormal labour | Requires training, manual recording [17] |
| Fetal Heart Rate | Intermittent auscultation | Assess fetal well-being | Simple, low-cost, minimal intervention | Less continuous information [8] |
| Electronic Fetal Monitoring | Continuous CTG / EFM | Detect fetal distress | Continuous data, early intervention | Requires equipment, may increase interventions [16] |
| Advanced Fetal Monitoring | Actograph, fetal scalp electrode | Accurate detection of fetal compromise | High precision, predictive | Invasive (electrode), requires expertise [21] |
Figure 1: Comparative Effectiveness of Maternal and Fetal Monitoring Methods in Detecting Labour Complications [5,8,16,21]
Fetal Monitoring
Fetal monitoring determines fetal well-being and oxygenation. It may be done through intermittent auscultation through a Doppler device or continuous electronic fetal monitoring (EFM). In the case of low-risk pregnancies, intermittent auscultation is appropriate and EFM offers constant data on fetal heart rate as well as the uterine contractions to assist in the early detection of fetal hypoxia or acidosis [8], [16]. Moreover, there are modern methods like actographs, the use of cardiotocography (CTG), which has helped in the accuracy of forecasting fetal compromise [21] Figure 1.
Clinical Guidelines and Best Practices
Evidence-based guidelines have to be followed during the process of labour induction and monitoring to guarantee maternal and fetal safety and enhance clinical outcomes [18-19]. Some professional bodies, such as the World Health Organization (WHO), American College of Obstetricians and Gynecologists (ACOG) and Royal College of Obstetricians and Gynaecologists (RCOG), have extensive recommendations about the indications, methods and monitoring practices [18,19].
Induction Guidelines
Indications for induction are post-term pregnancy (>41 weeks), premature membrane rupture, maternal hypertensive disorders, fetal growth retardation and maternal medical history [5,18]. Assessed with the Bishop score, cervical readiness continues to be a fundamental element in determining when and how the induction will take place[7,8]. Pharmacological treatment should be used when the need to limit complications like uterine hyperstimulation or fetal distress necessitates its usage, using standard protocols to rectify the situation [11,12]. Women who have contraindications to pharmacological agents or have undergone cesarean section before are advised to use mechanical methods [14].
Monitoring Guidelines
Maternal checks should also involve frequent checking of vital signs, labour progress with the partograph and knowledge of possible complication warning signs like hemorrhage or infection [17,20]. Different women have different recommendations of fetal monitoring based on the level of risk: low-risk pregnancies could utilize intermittent auscultation and high-risk pregnancies should implement continuous electronic fetal monitoring (EFM) [8,16]. To avoid poor maternal and neonatal outcomes, early detection is highlighted and early intervention is carried out.
Risk Management and Safety Procedures
Some optional measures, such as standardized induction checklists, ongoing fetal monitoring and complication-escalation channels, have been demonstrated to decrease the negative outcomes [18,20].Healthcare provider-to-healthcare provider training and simulation exercises enhance decision-making and response time in an emergency.
Those recommendations emphasize the individualization of care, the importance of weighing the advantages of timely induction of labour and the dangers of intervention and the need to follow the structured guidelines to manage the results in the most beneficial way [18-20]. Such guidelines have been shown to decrease cases of adverse maternal and neonatal events, such as protracted labour, cesarean delivery and neonatal intensive care admissions, upon implementation in clinical practice [16,20] (Table 3).
Table 3: Summary of Key Clinical Guidelines for Labour Induction and Monitoring
| Organization | Induction Recommendations | Monitoring Recommendations | Safety Considerations |
| WHO [18] | Induce only when medically indicated; use cervical ripening methods; avoid elective induction before 39 weeks. | Partograph for labour monitoring; intermittent auscultation for low-risk, EFM for high-risk | Standard protocols; minimize unnecessary interventions |
| ACOG [19] | Pharmacological (oxytocin, prostaglandins) preferred; mechanical methods for contraindications. | Continuous EFM for high-risk pregnancies; maternal vital signs every 1–2 hours | Monitor for hyperstimulation; timely cesarean if indicated |
| RCOG [19] | Assess Bishop score; combined methods for unfavorable cervix | Intermittent or continuous monitoring based on risk; use of CTG when indicated | Escalation protocols for fetal or maternal compromise |
Table 4: Maternal and Neonatal Outcomes of Labour Induction and Monitoring
Study / Author | Population | Induction Method | Maternal Outcomes | Neonatal Outcomes |
Beyene et al. [4] | 500 women, South Ethiopia | Oxytocin / prostaglandin | Reduced prolonged labour, moderate cesarean rate | Low Apgar <7 in 5%, NICU admission 7% |
Lohova-Matisa et al. [15] | Breech singleton pregnancies | Induction vs spontaneous labour | Increased operative delivery in the induction group | No significant difference in Apgar scores |
Abu Shqara et al. [1] | 350 women, Israel | Midwife-led induction | High maternal satisfaction, low complication rate | Minimal neonatal complications |
Masembe et al. [18] | Advanced maternal age, Uganda | Oxytocin / mechanical induction | Increased risk of hemorrhage and prolonged labour | Higher NICU admissions in the pharmacological group |
Chimwaza et al. [6] | 600 women, multi-center WHO study | Various clinical methods | Severe maternal outcomes <5% with continuous monitoring | Fetal distress was reduced by 12% with monitoring |
Mothers and Babies
The outcomes of the mother and Child: The results of labour induction and surveillance imply a great impact on the health of both the mother and the child and the knowledge of these implications is essential for the best clinical treatment [4-5,8]. Proper induction and constant observation can help mitigate the risks of a long pregnancy, maternal and child complications, but improper use of interventions can lead to even worse consequences.
Maternal Outcomes
Some of the outcomes, such as mode of delivery, duration of labour, postpartum bleeding, infection and maternal satisfaction, are maternal outcomes of induction of labour [4,17]. Research has demonstrated that when an appropriate induction method and monitoring plan are followed, the result can be that prolonged labour and unwarranted cesarean section can be reduced. Nevertheless, maternal complications like uterine hyperstimulation, infection, or operative birth are more probable when induction is done in the absence of sufficient cervical ripeness or when it is not monitored continuously [11-12,20].
Poor monitoring and the lag in the intervention in resource-limited conditions are linked to increased cases of severe maternal events, such as sepsis, hemorrhage and hypertensive disorders [2,6,17,20]. The continuity of care and experience of clinicians is also a critical factor in maternal outcomes. As an illustration, it has been found that midwife-led continuity models are linked to better maternal satisfaction and lower rates of intervention [14].
Neonatal Outcomes
The quality of monitoring during labour and the induction method are also factors that determine the neonatal outcomes. Monitoring assists in the early detection of fetal distress, thus enabling early measures to be applied to the distress, like operative delivery or oxygen replacement [8,16,21]. The negative neonatal outcomes are low Apgar scores, respiratory distress, admission to the neonatal intensive care unit (NICU) and perinatal mortality. There is an indication that the occurrence of severe neonatal complications is less when continuous fetal monitoring is done and this is more so in high-risk pregnancies [8,16].
A number of studies have been comparing neonatal outcomes involving the pharmacological and mechanical induction. Both of these approaches are typically safe, though when used with bad judgment, pharmacological induction has a greater risk of uterine hyperstimulation resulting in temporary abnormalities in the fetal heart rate [11-12,14]. Mechanical techniques, e.g., balloon catheters, are linked with fewer pharmacological side effects, but might not have good effectiveness in women with an undesirable cervix [14-15].
The Table 4 demonstrates that careful selection of induction methods combined with structured monitoring significantly improves maternal and neonatal outcomes. Continuous evaluation, adherence to clinical guidelines and individualized care planning remain crucial to minimizing risks [5-6,8,18].
Challenges and Future Directions
Even with drastic improvements in the labour induction and monitoring, there are still various challenges in achieving optimal maternal and neonatal outcomes. These issues can be found in the high-resource and low-resource environments and tend to be associated with the infrastructure, clinician experience, patient-related factors and compliance with the guidelines [6,17,20].
Challenges in Labour Induction and Monitoring
One of the primary obstacles is the inconsistency of clinical practice and adherence to standardized guidelines. Poor use of protocols, like improper time of induction or insufficient monitoring of the fetus, can result in more maternal and neonatal complications [2,6,18].Resource scarcity, untrained staff, monitoring and emergency intervention facilities also play a role in increased cases of severe maternal events such as sepsis, hemorrhage and hypertensive disorders in the resource-limited settings [17,20] (Figure 2).
The other issue is the problem of whether the positive effects of pharmacological induction and its possible dangers should be balanced. Although oxytocin and prostaglandins are effective in causing uterine contractions, they have the known dangers of uterine hyperstimulation and the abnormal heart rate of the fetus when poorly observed [11,12]. Likewise, mechanical procedures, although less toxic in some groups of people, might not be as effective in women with an unfavorable cervix, which necessitates further procedures [14,15].
The fetal monitoring is another process that has interpretation and implementation challenges. Continuous electronic fetal monitoring (EFM) has the advantage of real-time information, which may result in higher intervention rates, such as unnecessary cesarean section, when misclassified [16,21]. Intermittent auscultation, being safer in low-risk pregnancies, can be used, but may not detect the short-term handicapping of fetal distress [8].
Table 5: Challenges and Proposed Solutions in Labour Induction and Monitoring
| Challenge | Impact | Proposed Solutions / Future Directions |
| Variability in guideline adherence | Increased maternal and neonatal complications | Standardized training, checklists, audit systems [18,20] |
| Resource limitations (equipment, staff) | Higher maternal morbidity, inadequate monitoring | Investment in infrastructure, task-shifting, telemonitoring [6,25] |
| Risks of pharmacological induction | Uterine hyperstimulation, fetal heart rate changes | Individualized induction plans, combined with mechanical methods [11,18] |
| Fetal monitoring interpretation | Unnecessary interventions, missed distress | AI-assisted analysis, continuous training, decision support systems [25] |
Limited access to patient-centered care | Reduced maternal satisfaction, poor adherence | Midwife-led continuity models, education, counseling [1,14] |
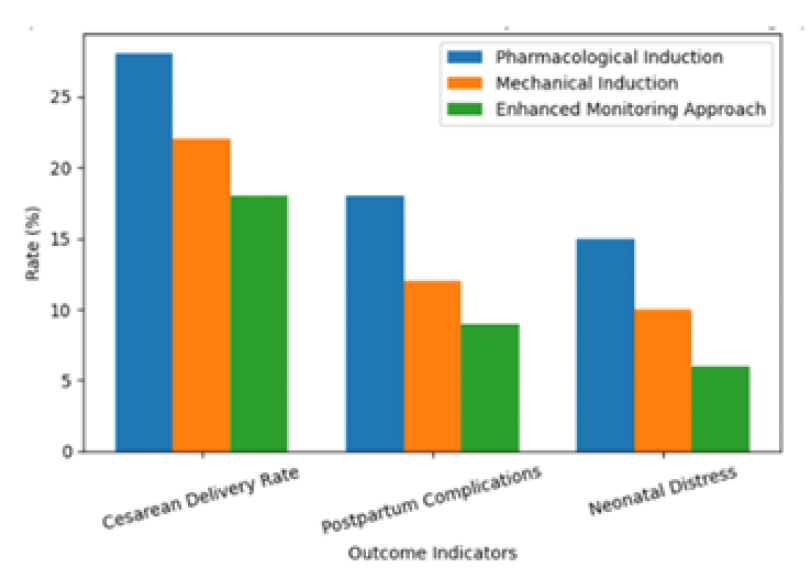
Figure 2: Comparison of Maternal and Neonatal Outcomes Across Labour Induction and Monitoring Approaches [1,4,6,15]
Future Directions and Innovations
These challenges can be solved with the help of emerging technologies. Digital monitoring devices such as wireless fetal monitors, telemetric data analysis and AI-based predictive algorithms could help to improve the early detection of complications and decrease the need to rely on subjective interpretation [25]. The application of these technologies in everyday clinical practice may help address maternal and neonatal outcomes, especially in pregnancies with high risks.
Capacity building and training are also important. There is an indication that midwife-led continuity of care models and specific simulation-based training can enhance decision-making, compliance and patient satisfaction [1], [14]. Moreover, a patient-centered approach, which includes the combination of pharmacological and mechanical induction, could lead to a higher success of labour induction with a minimum of risks [18].
Lastly, there is a need to continually research and enhance risk stratification, undertake optimal monitoring protocols and design minimally invasive cost-effective interventions that are applicable in both high- and low-resource environments [6,20,25].
Labour induction and monitoring are the core elements of contemporary obstetric care and they are instrumental in maintaining maternal and fetal health. As noted in this review, induction of labour can be used to avoid negative cases of prolonged pregnancy, maternal health problems and fetal distress when indicated and well controlled [4], [5], [18]. Nevertheless, induction, in turn, is associated with the effectiveness and safety that largely rely on the proper selection of patients, cervical examination and compliance with evidence-based clinical practices.
Pharmacological and mechanical ways of inducing labour have proven clinical efficacy, but both have their own advantages and disadvantages. Predictable and efficient pharmacological agents like oxytocin and prostaglandins can be used to stimulate the uterus and they need close observation because of the possibility of uterine hyperstimulation and fetal distress [11-12]. Balloon catheters are safer in the chosen population, especially among women with a previous cesarean section or contraindicators to prostaglandins [14-15]. The facts justify personalized induction measures that take into account maternal condition, fetal status and available clinical resources.
Supervision of labour is also a major necessity and the foundation of early diagnosis and prompt action. Regular or non-regular monitoring of maternal vital parameters, labour and fetal health greatly lowers the morbidity of motherhood, as well as child birth complications in instances where this is done properly [8,16,21]. Structured tools like the partograph and electronic fetal monitoring can improve the process of clinical decision-making, though the right interpretation and the prevention of unneeded interventions are still important issues.
Moreover, uneven prices of access to skilled services, monitoring devices and standard measures still influence the outcomes, especially in the case of low-resource environments [6,17,20]. By bridging these gaps by means of capacity building, implementing guidelines and integrating new digital health technologies, one can make a significant contribution to the perinatal outcomes. New strategies, such as the use of AI to monitor the fetus and telemedicine to monitor a fetus, have the potential to help increase early warning systems and equity in the treatment of mothers [25].
Conclusively, the most effective clinical strategies of inducing labour and monitoring it demand an evidence-based, balanced and patient-centered system. Enhancing compliance with guidelines, enhancing the education of clinicians and the adoption of technological innovations are necessary measures that would allow for the decrease in preventable morbidity and mortality rates in mothers and neonatal care. Further studies and policy reinforcement are essential to achieve beneficial, secure and fair obstetric care throughout the world.
Abu Shqara, R. et al. “Impact of midwife clinical experience and survey-based attitudes towards labor epidural analgesia on utilization rates in pregnant patients: A survey-based cohort study.” International Journal of Obstetric Anesthesia, vol. 65, 2026, https://doi:10.1016/j. ijoa.2025.104809.
Abera, B.T. et al. “Maternal sepsis and factors associated with poor maternal outcomes in a tertiary hospital in Tigray, Ethiopia: A retrospective chart review.” BMC Infectious Diseases, vol. 24, no. 1, 2024, https://doi:10.1 186/s12879-024-09075-9.
Banno, A. et al. “A simple, efficient and scalable method to generate oocyte-like cells in vitro.” Life Science Alliance, vol. 9, no. 2, 2026, https://doi:10.26508/lsa.202503379.
Beyene, T. et al. “Severe maternal outcomes and quality of maternal health care in south Ethiopia.” International Journal of Women’s Health, vol. 14, 2022, pp. 119–130, https://doi:10.2147/IJWH.S341912.
Cruz Cruz, Y. et al. “Endobronchial tumor, diagnosis and clinical and imaging evolution: A case report.” South Health and Policy, vol. 5, 2026, p. 240, https://https://doi:10.5 6294/shp2026240.
Chimwaza, Y. et al. “Early warning systems for identifying severe maternal outcomes: Findings from the WHO global maternal sepsis study.” EClinicalMedicine, vol. 79, 2025, https://doi:10.1016/j.eclinm.2024.102981.
Deng, J. et al. “Shallow-middle-deep feature aware denoiser for low-dose computed tomography.” Digital Signal Processing, vol. 168, 2026, https://doi:10.1016/ j.dsp.2025.105666.
David, A.L. and R.N. Spencer. “Clinical assessment of fetal well-being and fetal safety indicators.” Journal of Clinical Pharmacology, vol. 62, no. S1, 2022, pp. S67–S78, https://doi:10.1002/jcph.2126.
Denizli, R. et al. “Effect of Ramadan fasting in Turkey upon fetal well-being and perinatal outcomes during the last trimester of pregnancy.” Journal of Religion and Health, vol. 62, no. 2, 2023, pp. 879–887, https://doi:10.1007/s1094 3-023-01744-4.
Franiko, R. and E.J. Suhendra. “Determining the optimal timing for surgery in benign prostatic hyperplasia.” European Journal of Medical and Health Sciences, vol. 7, no. 3, 2027, pp. 92–97, https://doi:10.24018/ejmed.2025.7. 3.2289.
Granger Howard, M.E. et al. “Planned community birth and birth outcomes.” JAMA Pediatrics, 2026, https://doi:10.1 001/jam apediatrics.2025.4840.
Guan, H. et al. “Enhancing radiology report interpretation through modality-specific RadGraph fine-tuning.” Lecture Notes in Computer Science, vol. 15966, 2026, pp. 216–225. Springer Science and Business Media Deutschland GmbH, https://doi:10.1007/978-3-032-04981-0_21.
Hajime, T. et al. “Estimating the length and extension direction of single-shaped burrows formed by benthic crabs using ultrasound.” Measurement, vol. 257, 2026, https://doi:10.1016/j.measurement.2025.118550.
Kuipers, Y. et al. “Midwife continuity of care: a systematic review and meta-analysis of case-control and cohort studies.” International Journal of Nursing Studies, February 2026, https://doi:10.1016/j.ijnurstu.2025.105300.
Lohova-Matisa, E. et al. “Breech singleton labour: induction vs spontaneous.” European Journal of Obstetrics & Gynecology and Reproductive Biology, vol. 313, 2025, p. 114235, https://doi:10.1016/j.ejogrb.2025.114235.
Lai, J. et al. “The use of actograph in the assessment of fetal well-being.” Journal of Maternal-Fetal and Neonatal Medicine, vol. 33, no. 12, 2020, pp. 2116–2121, https://doi:10.1080/14767058.2018.1540584.
Leta, M. et al. “Adverse maternal outcomes among women who gave birth at public hospitals in eastern Ethiopia: a cross-sectional study.” Frontiers in Global Women’s Health, vol. 6, 2025, https://doi:10.3389/fgwh.2025.1569815.
Masembe, S. et al. “Adverse maternal outcomes and associated factors among mothers of advanced age delivering at a tertiary hospital, southwestern Uganda: a cross-sectional study.” BMC Pregnancy and Childbirth, vol. 24, no. 1, 2024, https://doi:10.1186/s12884-024-06557-1.
Muče, A.A. et al. “Effects of gestational diabetes mellitus on risk of adverse maternal outcomes: a prospective cohort study in northwest Ethiopia.” BMC Pregnancy and Childbirth, vol. 20, no. 1, 2020, https://doi:10.1186 /s12884-020-2759-8.
Melesse, M.F. et al. “Maternal outcomes of severe preeclampsia and eclampsia and associated factors among women admitted at referral hospitals of Amhara regional state, institutional-based cross-sectional study, north-west Ethiopia.” Frontiers in Global Women’s Health, vol. 6, 2025, https://doi:10.3389/fgwh.2025.1555778.
Narain, S. and A. McEwan. “Antenatal assessment of fetal well-being.” Obstetrics, Gynaecology and Reproductive Medicine, August 2023, https://doi:10.1016/j.ogrm.20 23.05.002.
Purwati, Y. and A.D. Sari. “Audiovisual effectiveness of independent fetal well-being monitoring on mother–fetus attachment and birth outcomes.” Enfermería Global, vol. 23, no. 1, 2024, pp. 82–94, https://doi:10.6018/eglob al.568371.
Qasim, S. et al. “Clinical spectrum and outcome in children presenting with empyema thoracis in tertiary care hospital: role of intrapleural streptokinase.” Pakistan Journal of Medical and Health Sciences, vol. 17, no. 11, 2027, pp. 458–461, https://doi:10.53350/pjmhs20231711458.
Ramberran, M. et al. “Can foreign datasets help improve plankton classification performance for local data?” Lecture Notes in Networks and Systems, vol. 1676, 2026, pp. 19–37. Springer Science and Business Media Deutschland GmbH, https://doi:10.1007/978-3-032-07989-3_2.
Taviti, S. et al. “Integrated approaches for secure and predictive management of electronic health records: a review.” Lecture Notes in Networks and Systems, vol. 1463, 2026, pp. 97–106. Springer Science and Business Media Deutschland GmbH, https://doi:10.1007/978-981-96-7514-2_8.
