+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-603X
ISSN (Online) : 2789-6048
Background: The study was conducted to evaluate the correlation between Central Macular Thickness (CMT) & Clinically Significant Macular Edema (CSME) in Patients of Type 2 Diabetes Mellitus present at Ophthalmology OPD of Tertiary Care center. Material & methods: This was a cross-sectional study on type 2 diabetes patients conducted in the department of ophthalmology, Indira Gandhi Medical College Shimla (H.P) for a period of one year. Patients who fulfilled the inclusion criteria were interviewed regarding the duration of diabetes mellitus and treatment history. A complete ophthalmologic examination including Central Macular Thickness (CMT) and were performed to all patients. Results: A total of 260 eyes from 130 patients (87 males, 43 females; mean age 56.88±8.26 years) were included in this study. The mean duration of DM was 8.87±2.34 years (range, 1-25 years). In the present study, CMT in right eye ranged from 189–751 μm with mean value of 260.41±101.66. CMT in left eye ranged from 180–561 μm with mean value of 255.69±88.89. Among 130 subjects, clinically significant macular edema (CSME) was present in 30% (n=39). CMT was found to be significantly raised in CSME group with a mean of 355.02±126.68 μm compared to no CSME group with a mean CMT value of 216.48±19.72 μm (p= <0.001). Conclusion: Present study concluded that Increased Central Macular Thickness (CMT) was significantly correlated with clinically significant macular edema (CSME) among Patients of Type 2 Diabetes Mellitus present at Ophthalmology OPD.
The eyes can be impacted by chronic Diabetes Mellitus issues along with other organs and systems. Cataracts, glaucoma, macular edoema, iris rubeosis, non-proliferative or proliferative diabetic retinopathy, and unstable refraction are some of the ophthalmologic effect [1],
The most common cause of visual impairment in diabetics, especially type 2 people, is diabetic maculopathy (fovealedema, exudates, or ischaemia). Traditional methods for determining macular edoema include slit-lamp biomicroscopy, stereoscopic photography, and fluorescein angiography. These methods are, at best, qualitative and relatively insensitive to minute variations in retinal thickness. Since the invention of optical coherence tomography (OCT), medical professionals have been able to objectively evaluate the efficacy of various treatment methods and reliably spot and quantify slight variations in retinal thickness [2,3].
Clinically Significant Macular Edema (CSME), as defined by the ETDRS study is “thickening of the retina at / within 500 µm of the centre of the macula (or) hard exudates at / within 500 µm of the centre of macula, if associated with thickening of the adjacent retina or one or more zones of retinal thickening, 1 disc area or larger, any part of which is within 1 disc diameter of the centre of the macula”. CSME is a common occurrence in many cases of diabetic retinopathy. Up to 75,000 new cases of diabetic macular edema develop each year, and about 30% of patients with clinically significant macular edema develop moderate visual loss. CSME is the commonest cause of moderate visual loss in diabetic retinopathy cases [4-7].
We conducted this study in our setup to evaluate the Correlation between Central Macular Thickness (CMT) and Clinically Significant Macular Edema (CSME) in Patients of Type 2 Diabetes Mellitus Present at Ophthalmology OPD of Tertiary Care centre due to the conflicting reports in the literature and paucity of studies relative to the existing case load in the Indian population.
Aims and Objectives
The aim of this study was to evaluate the Correlation between Central Macular Thickness (CMT) & Clinically Significant Macular Edema (CSME) in Patients of Type 2 Diabetes Mellitus present at Ophthalmology OPD of Tertiary Care center.
Study Area
The study was conducted in Department of Ophthalmology, Indira Gandhi Medical College, Shimla, Himachal Pradesh.
Study Period
The study was conducted for 12 months after approval from Institutional Ethics Committee from July 2018 to June 2019.
Study Design
It was a cross-sectional descriptive study of diagnosed patients of Diabetes mellitus attending eye OPD of Indira Gandhi Medical College, Shimla, Himachal Pradesh.
Study Population
Patients with Type II diabetes mellitus with and without fundus changes of Non-Proliferative Diabetic Retinopathy (NPDR) of any severity.
Selection Criteria
Inclusion Criteria
Patients with Type II Diabetes Mellitus on or off treatment within age group of 40-70 years reporting in the OPD after the start of the study.
Patients who gave their consent for participation in the study.
Exclusion Criteria
Patient with pre-existing macular pathology such as ARMD, hereditary maculopathy.
Patient who have undergone any laser surgery in retina.
Hypertensive retinopathy more than grade II.
Uveitis.
Media haze grade 3 or 4.
Patient who have undergone cataract surgery.
Patients with history of ocular trauma.
Patients with proliferative diabetic retinopathy.
Patients taking retino toxic drugs.
Type I Diabetes Mellitus.
Not willing for study.
Materials
After taking history each patient underwent ophthalmic examination as given below:
For Visual Acuity
Snellen’s chart for distant vision.
Jaeger’s chart for near vision.
Refraction
To rule out any refractive error.
For Complete Anterior Segment Examination
Slit Lamp Biomicroscopy (HAAG STREIT-BQ 900 WITH IMAGING MODULE IM 900 made in Switzerland) examination to see anyopacity in the media, lens for evidence of cataract, pseudophakia, aphakia and anterior vitreous for pigment and cells.
For Intra Ocular Pressure
Schiotz tonometer/Goldmann’s applanation tonometer/NCT.
For Colour Vision
Ishihara’s pseudo isochromatic plates
Amsler’s Grid Test for Both Eyes
For Fundus Examination: The pupil was dilated by instilling one to two drops of 5% Phenylephrine Hydrochloride with 0.8% Tropicamide, in patients with normal IOP and normal anterior chamber depth. After 45 minutes when the pupil was fully dilated, the patient was examined with:
Direct ophthalmoscope (HEINE Beta 200S)
Volk’s +90 D aspheric lens under slit lamp
Indirect ophthalmoscope (AAIO WIRELESS)
For Central Macular Thickness
SD-OCT volume scan with TOPCON 3D OCT-1 Maestro (Version 8.42) under dilation with 5% Phenylephrine Hydrochloride with 0.8% Tropicamide in every patient. Using the retinal thickness map analysis protocol, macular thickness was determined and compared with normative data. It consists of a macular cube 512 × 128 (vertical × horizontal) axial scans covering an area of 6 × 6 mm in the macular region. The macula was divided into 3 concentric circles centered at the fovea. This division is a superimposition of the ETDRS map over the OCT map of the macula. It consists of 3 zones; the fovea (less than 1 mm diameter), the inner macula (1 to 3 mm) and the outer macula (3 to 6 mm). Foveal or central macular thickness is defined as the average thickness in the central 1 mm diameter. The central macular thickness was measured thrice and average was calculated.
Investigations
The results of glycosylated haemoglobin (HbA1c) test, lipid profile and other relevant investigations done were recorded for each patient.
Methodology
This study was started after clearance from protocol review committee and the ethical committee. Pretesting of the study proforma was carried out and appropriate changes were done.
For the selection of study population, all the patients who reported in the Eye OPD of Department of Ophthalmology, Indira Gandhi Medical College, Shimla, Himachal Pradesh were included in the study who qualified for the inclusion and exclusion criteria as stated above and who gave their consent.
•The presence of DM in all patients had been confirmed by the corresponding Internal Medicine Department.
As per study proforma, each patient were asked history regarding demographic variables like age, gender, occupation, address. The patients were subjected to various biochemical investigations and detailed ophthalmological examination as per proforma enclosed.
The informed consent was taken from all patients taken up for study.
Defining Criteria
American Diabetes Association (ADA) recommends that diagnosis of diabetes be made when the person is symptomatic with polydipsia, polyphagia, polyuria or weight loss with:
RBS ≥ 200mg/dl
FBS ≥126 mg/dl.
RBS is defined as blood glucose level at any time of day without regard to time since last meal.
FBS is defined as blood glucose with no caloric intake for at least 8 hrs.
If patient is asymptomatic ,then 2 blood glucose value are mandatory, preferably 1 including FBS value.
HbA1c ≥ 6.5%
Hypertension
BP values of ≥140/90 mm of Hg (JNC-VII criteria)
Obesity
BMI of ≥25 (JAPI criteria)
Retinopathy
ETDRS criteria was used and retinopathy was classified according to the most severe changes in the worse eye.
Dyslipidemia
According to NCEP-ATP III guidelines, hypercholesterolemia is defined as:
TC >200mg/dl
LDL-C as >100mg/dl
Hypertriglyceridemia as TG >150mg/dl and
HDL-C <40mg/dl.
Dyslipidemia is defined by presence of one or more than one abnormal serum lipid concentration.
Patients were assessed for the presence of clinically significant macular edema (CSME) using slit-lamp biomicroscopy assessment with a 90D lens. The definition utilized in diagnosing CSME was the presence of one or more of the following (Early Treatment Diabetic Retinopathy Study Research Group 1991):
Retinal thickening at or within 500 micron of center of macula.
Hard exudates at or within 500 micron of center of the macula if associated with adjacent retinal thickening.
Zone or zones of retinal thickening 1 disc area in size, at least part of which is within one disc diameter of center of macula.
Statistical Analysis
The collected data was entered in Microsoft Excel and then analysed and statistically evaluated using SPSS-PC-20 version. Quantitative data was expressed by mean, standard deviation and while qualitative data was expressed in percentage. Difference between the proportions was tested by chi square test or Fisher’s exact test while difference between quantitative variable between two group were tested by Student ‘t’ test or Fisher Exact test. For comparison of quantitative data between more than two groups, ANOVA or Kruskal Wallis ‘H’ test followed by posthoc test was used. The correlation between Clinically Significant Macular Edema (CSME) and CMT was analysed using Karl Pearson’s correlation coefficients. A ‘p’ value less than 0.05 was considered statistically significant.
The present study was conducted in the Department of Ophthalmology, Indira Gandhi Medical College, Shimla H.P. It was a cross-sectional study of diagnosed patients of type 2 diabetes mellitus attending eye OPD of Indira Gandhi Medical College Shimla from July 2018 to June 2019.
Both eyes (260 eyes) of one hundred thirty (130) patients diagnosed with type 2 diabetes with or without diabetic retinopathy within age group of 40-70 years and diabetes duration of at least 1 year served as the study group on the basis of predefined inclusion and exclusion criteria.
Total of 130 patients were taken of which 66.9% were male (n=87) and 33.1% were females (n=43). The age of the patients in the study ranged from 40 - 70 years. Mean age of study subjects was 56.88±8.26 years. Duration of diabetes in study subjects ranged from 1- 25 years (Mean 8.87±2.34). There were 34.6% (n=45) of patients who had duration of diabetes equal to or less than 5yrs. There were 34.6% (n=45) of patients who had duration of diabetes between 6-10 years, 20% (n=26) patients had duration of diabetes between 11-15 years and 10.8% (n=14) patients had duration of diabetes >15 years.
In the present study, CMT in right eye ranged from 189–751 μm with mean value of 260.41±101.66. CMT in left eye ranged from 180–561 μm with mean value of 255.69±88.89.
Among 130 subjects, clinically significant macular edema (CSME) was present in 30% (n=39).
CMT was found to be significantly raised in CSME group with a mean of 355.02±126.68 μm compared to no CSME group with a mean CMT value of 216.48±19.72 μm (p= <0.001).
Table 1: Distribution of Age, Gender & duration of diabetes among study subjects (n=130)
Age (in years) | ||
≤45 years | 10 | 7.7 |
46-55 years | 49 | 37.7 |
56-65 years | 52 | 40.0 |
>65 years | 19 | 14.6 |
Gender | ||
Male | 87 | 66.9 |
Female | 43 | 33.1 |
Duration of diabetes | ||
≤5 years | 45 | 34.6 |
6-10 years | 45 | 34.6 |
11-15 years | 26 | 20.0 |
>15 years | 14 | 10.8 |
Table 2: Descriptive characteristics of study subjects
| Mean | CMT-R | CMT-L |
260.41 | 255.69 | |
SD | 101.66 | 88.89 |
Median | 223.00 | 222.50 |
IQR | 204.75-250 | 208-251 |
Minimum | 189 | 180 |
Maximum | 751 | 561 |
Table 3: CSME in study subjects
CSME | No. | % |
Present | 39 | 30.0 |
Absent | 91 | 70.0 |
Table 4: Association of CSME with different parameters
| Parameter | CSME Present | CSME Absent | p-value | ||
Mean | SD | Mean | SD | ||
CMT-Right eye | 362.77 | 137.16 | 216.54 | 19.59 | <0.001 |
CMT-left eye | 347.28 | 116.55 | 216.44 | 19.96 | <0.001 |
CMT-average | 355.02 | 126.68 | 216.48 | 19.72 | <0.001 |
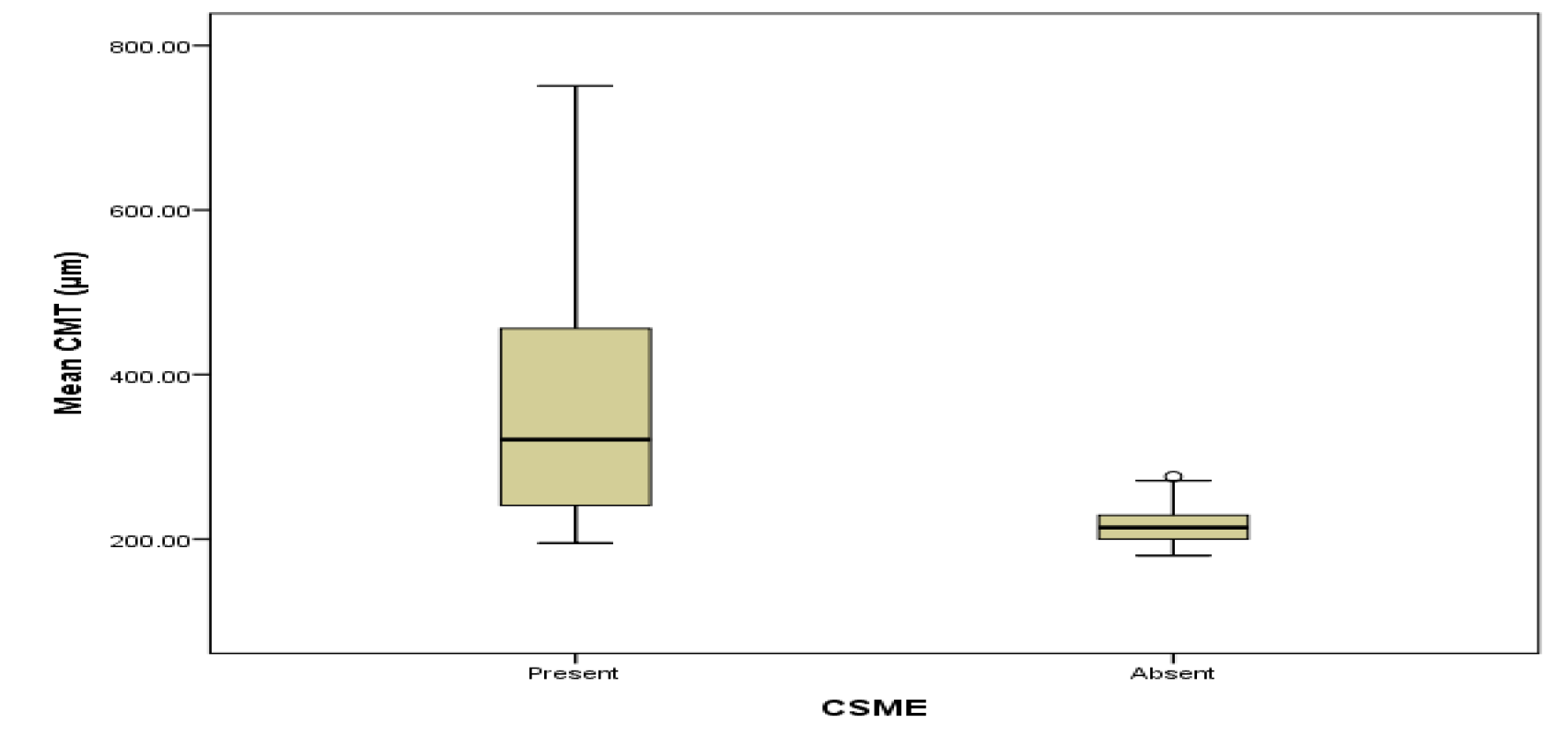
Figure 1: Boxplot showing association of CMT with CSME
Present study was done to evaluate the Correlation between Central Macular Thickness (CMT) & Clinically Significant Macular Edema (CSME) in Patients of Type 2 Diabetes Mellitus present at Ophthalmology OPD of Tertiary Care center. Among 130 subjects, clinically significant macular edema (CSME) was present in 30% (n=39). CMT was found to be significantly raised in CSME group with a mean of 355.02±126.68 μm compared to no CSME group with a mean CMT value of 216.48±19.72 μm (p= <0.001). This is in concordance with the study done by Chung et al8 who found a positive correlation with development of diabetic macular edema and with increased central retinal thickness in DM patients.
Present study concluded that Increased Central Macular Thickness (CMT) was significantly correlated with clinically significant macular edema (CSME) among Patients of Type 2 Diabetes Mellitus present at Ophthalmology OPD.
Fauci, A. et al. Harrison’s Manual of Medicine. 19th ed., McGraw-Hill Education LLC, 2016.
Raman, R. et al. “Influence of Glycosylated Hemoglobin on Sight-Threatening Diabetic Retinopathy: A Population-Based Study.” Diabetes Research and Clinical Practice, vol. 92, no. 2, 2011, pp. 168–173.
Bowling, B. “Retinal Vascular Diseases.” Kanski’s Clinical Ophthalmology, edited by B. Bowling, 8th ed., Elsevier Health Sciences, 2016, pp. 520–528.
Raman, R. et al. “Influence of Serum Lipids on Clinically Significant Versus Nonclinically Significant Macular Edema: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetic Study Report.” Ophthalmology, vol. 13, no. 10, 2010, pp. 1–7.
Narang, S. et al. “Atorvastatin in Clinically Significant Macular Edema in Diabetics.” Nepal Journal of Ophthalmology, vol. 4, no. 7, 2012, pp. 23–28.
Jew, O. et al. “Risk Factors for Clinically Significant Macular Edema in a Multi-Ethnic Population with Type 2 Diabetes.” International Journal of Ophthalmology, vol. 5, no. 4, 2012, pp. 499–504.
Deepa, C.K. et al. “Influence of Serum Lipids on Clinically Significant Macular Edema in Type 2 Diabetic Retinopathy Cases.” IP International Journal of Ocular Oncology and Oculoplasty, vol. 7, no. 1, 2021, pp. 82–88.
Chung, Y. et al. “Association of Statin Use and Hypertriglyceridemia with Diabetic Macular Edema in Patients with Type 2 Diabetes and Diabetic Retinopathy.” Cardiovascular Diabetology, vol. 16, no. 1, 2017, pp. 23–28.
