+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6056
ISSN (Online) : 2789-6064
The rate of obesity in the world has grown significantly over the past decades, becoming one of the most urgent issues of global public health. The escalating prevalence in all age groups and geographies has been strongly associated with heightened risks of metabolic illnesses, cardiovascular disorders, and premature deaths, and high social and economic expenses. It is estimated that, without effective preventive measures, the prevalence rates of obesity will rise due to the lack of preventive measures [1-3]. This article aims to discuss the idea of prevention and policy-based interventions to decrease the burden of obesity in the whole world, and not to concentrate on the interventions at the individual level (behavioral ones). The article synthesizes evidence-based views on obesity prevention in various areas, primarily focusing on food systems, promoting physical activity, health equity, and governance structures that influence obesity outcomes. Some of the major areas of prevention that have been discussed are food and nutrition policies to enhance dietary conditions, physical activity-conducive policies integrated into urban planning and health systems, and equity-based policies that deal with disproportionate effects of obesity among socioeconomically disadvantaged groups. Another issue that the article raises, which is important to note, is the principle of multisectoral governance and the coordinated policy action to combat the multifaceted and interrelated causes of obesity on the national and global fronts. The policy implications highlight the necessity of holistic, evidence-based, and equity-focused policies that go beyond individual blame and response and focus on structural factors that cause obesity. It is necessary to strengthen preventive policies at the food systems level, physical activity environment, and social protection to end up with sustainable reductions in obesity prevalence. To sum up, prevention and policy interventions must be considered as the key means to enhance the health of people in the global community: therefore, addressing the global obesity epidemic needs an urgent, coordinated, public health response.
Global Scope and Significance of Obesity
Obesity is a significant international health issue with the prevalence steadily increasing and becoming common in almost all parts of the world and cutting across children, adolescents, and even adults. Worldwide, there is evidence of an overall growing trend in overweight and obesity over the last few decades, which shows that there is a significant trend of dietary changes, physical activity, and general social and economic conditions. These tendencies can be observed in the high-income and the low- and middle-income countries, in which the rapid urbanization and changes in nutrition have stimulated the rapid growth of obesity and the presence of undernutrition [2,4].
Obesity has long-term health effects that are very profound. There is a significant risk of various non-communicable diseases associated with obesity, such as type 2 diabetes, heart disease, some types of cancers, and skeletal diseases. At the population level, the escalating morbidity, poor quality of life, and early mortality are due to the high burden of obesity. In addition to health outcomes, obesity is very economically expensive to individuals, health systems, and society in terms of high expenditure on healthcare, lost productivity, and long-term disability. Recent international reports suggest the strong connection between the increasing rate of obesity and the growing population of metabolic disease across the globe [2-3].
Obesity is being identified as a primary cause of metabolic disease and chronic disease on the global front. Excessive body weight is directly related to dysfunction of the metabolic system, such as insulin resistance, dyslipidemia, and systemic inflammation, which all form the basis of numerous chronic diseases. As the world trends of obesity keep changing, the consequent burden of metabolic and chronic illnesses is bound to escalate, and this puts a further burden on already overburdened health systems [3-4].
Prevention and Policy-Based Approach Rationale
The conventional methods of dealing with obesity have tended to focus more on individual blame, where the emphasis is laid on behavioral modification at the personal level through diet and exercise. Although these interventions can help very few people, they have not had a significant effect on population trends in obesity. Concrete obstacles, such as poor food and nutrition conditions, financial limitations, and lack of physical exercise, often sabotage individual intentions to keep the body at a healthy weight. Consequently, the use of interventions at the individual level has not been adequate in reversing or stopping the worldwide prevalence of obesity [5].
Conversely, prevention and policy-based methods have the potential to have greater and more long-term effects by influencing the people living, working, and eating environments. Policies at the population level, like food and nutrition policies, urban planning efforts, fiscal policy, and regulations, can impact the populations as a whole, minimizing their exposure to obesogenic situations. There is a growing push among obesity-related policy-making and research to emphasize a pivot to policy-based remedies benefiting the social, economic, and environmental factors that cause obesity and include the equity and fairness aspects [6]. These strategies view obesity as a systemic problem that needs to be addressed through the concerted efforts of various sectors other than the health system.
Objectives of the Article
This article has threefold objectives. First, it tries to analyze important prevention measures that can alleviate the worldwide obesity burden at various life stages. Second, it aims at examining policy strategies that can respond to structural and systemic factors of obesity, specifically focusing on food systems, physical activity environments, and governance. Lastly, the article presents the problem of health equity and implementation and investigates issues and opportunities that may emerge when national and global prevention and policy strategies are translated into effective and sustainable action.
Obesity as a Complex Global Public Health Challenge
Multifactorial Drivers of Obesity: It is a well-known fact that obesity is a complicated issue that develops due to the interplay of various biological, social, economic, and environmental factors, as opposed to behavior alone. Genetic predisposition, metabolic regulation, and physiological reactions to food and physical activity are at the biological level of factors that affect susceptibility to weight gain. The biological factors, however, exist in a wider social and environmental context that influences the day-to-day behaviors and health outcomes [7].
Income, education, occupation, and social norms are social determinants that are very critical in influencing dietary practices and physical activity patterns. People in worse socioeconomic conditions usually experience low access to nutritious foods, secure locations of physical exercise, and health-enhancing materials. Economic aspects, which include the prices of foods, the employment levels, and income inequality, also contribute towards the differences in prevalence of obesity among and within the population. Opportunities for healthy living can be facilitated by environmental determinants such as the built environment, the transportation system, and the neighborhood design, or restricted in these opportunities. These interrelated drivers combine to highlight why it is necessary to frame obesity as a systemic social health issue, and that is entrenched in larger social systems [7-8] (Figure 1).
Food Systems and Globalization
Over the past decades, global food systems have been experiencing radical changes, which have been one of the causes of the increased obesity burden. One of the main aspects of this change is the nutrition transition, which is the shift to the higher intake of nutrient-poor foods of high energy content, such as fat, sugar, and refined carbohydrates. This shift has occurred especially quickly in the low- and middle-income nations, where shifts in income, urbanization, and availability of food have redefined the population's dietary patterns [9].
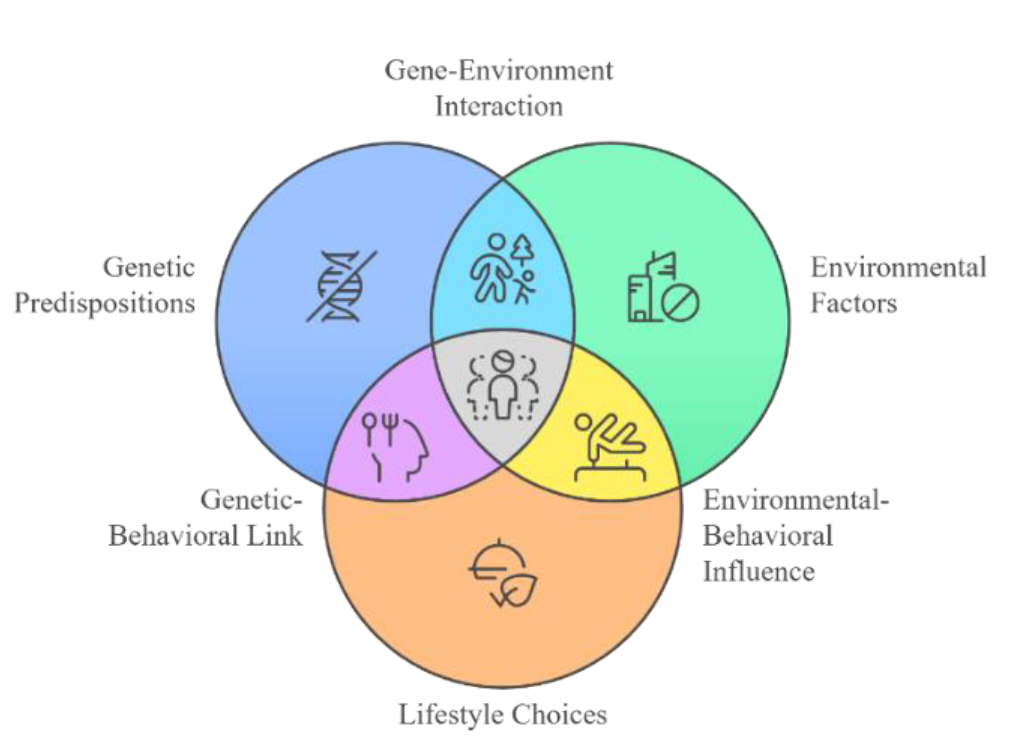
Figure 1: Multifactorial Drivers of Obesity
Table 1: Multilevel Determinants of Obesity
| Level | Key Determinants | Analytical Interpretation |
| Individual | Dietary patterns, physical activity, biological susceptibility | Individual behaviors are shaped by upstream social and environmental constraints, limiting the effectiveness of purely behavior-focused interventions |
| Household and Community | Built environment, food access, social norms | Community contexts structure daily choices by enabling or constraining access to healthy foods and opportunities for physical activity. |
| Food System | Food processing, pricing, marketing, supply chains | Industrialized food systems promote energy-dense, ultra-processed foods, driving population-level excess calorie intake |
| Policy and Governance | Regulation, taxation, urban planning, social protection | Policy environments determine the availability, affordability, and desirability of healthy choices, making governance central to obesity prevention |
The broad accessibility and intensive marketing of ultra-processed foods are a central process by which the contemporary food systems could have an impact on risk factors of obesity. They tend to be cheap, well-flavored, and extremely marketed, which are particularly attractive in situations when time, money, and availability of fresh foods are short. The overcrowding of ultra-processed food in the global markets has contributed to higher caloric intake and low-quality diet, which confirms the presence of the obesogenic food environment [10].
Another factor that influences the national food environment is the agricultural policies, trade agreements, and global supply chains. The subsidies, trade liberalization, and food safety regulations affect the production, distribution, and consumption of foods, with a tendency to put more emphasis on efficiency and profitability, at the expense of nutritional quality. The inclusion of nutrition in the food systems policy has hence become a key urgent concern in the prevention of obesity, which demands concerted efforts across agriculture, trade, health, and environmental sectors [11] (Table1).
Interpretive Commentary
Individually, obesity risk cannot be entirely attributed to personal choice, but also to exposure to obesogenic environments, thus presenting limitations to interventions based purely on personal responsibility [7].
Systematic neighborhood design and food access differences at the community level influence health behaviors, which support socioeconomic gradients in obesity prevalence [8].
In the food system, the prevalence of ultra-processed foods is a structural incentive to prioritize profit over nutrition, which leads to extensive dietary risk on the population level [9].
Government controls, and other mechanisms involved in policy like tax, regulation, and urban planning have the highest leverage to population-wide impact by altering environments rather than acting on an individual basis [5].
Prevention Approaches across the Life Course
Early-Life and Maternal Prevention: Avoidance of obesity in infancy and, more importantly, during pregnancy is a very crucial measure in curbing the burden of obesity in the world. Maternal obesity is also found to be a major risk factor in causing obesity in children, and in the long run, maternal and child health are affected. Research indicates that maternal obesity and too much weight gain during pregnancy are linked to an increased risk of gestational diabetes, preeclampsia, and complications during childbirth, as well as being a cause of the increased prevalence of childhood obesity [12].
There are several complex mechanisms between maternal obesity and childhood obesity. Genetic and epigenetic conditions, and intrauterine environmental conditions, may modify the mechanism of metabolism and appetite control in a child, thus making them prone to obesity during adulthood. As an example, maternal under-/overnutrition can impact the fat storage and insulin sensitivity of the infant and make them susceptible to obesity and metabolic disorders during the adult years [12].
The interventions, which can be applied to address the intergenerational obesity cycle, are improving maternal nutrition, healthy weight gain in pregnancy, and prenatal care. These risks can be alleviated by providing nutritional advice aimed at maintaining a balanced diet high in fruits, vegetables, and whole grains and avoiding overcaloric and fatty foods. In addition, obesity and the associated conditions can be screened during pregnancy, thereby enabling early interventions, thereby minimizing the chances of having bad health outcomes for the mother and the child. Early prevention of obesity is one of the most cost-effective and effective approaches to improving the health of the population, is prevents it at this stage of life, because many early interventions have a long-term effect on the future population [12].
Childhood and Adolescent Prevention
The prevention of obesity among children and adolescents is especially of concern because this is the period of childhood and adolescence when the child develops habits with regard to diet, physical activity, and lifestyle. These habits are usually formed in adulthood when formed and as such, childhood is a crucial time to prevent obesity. Interventions in schools have been identified as one of the best techniques in combating obesity at this age because they cut across a large population of children. Schools are the most suitable environment where dietary habits, physical exercise, and nutritional education may be encouraged. These interventions can be used to reverse the prevalence of obesity and promote healthier lifestyle habits by offering healthier food in schools, introducing physical education (PE) into the student timetable, and educating students about the nutritional value of a balanced diet [13].
Nutrition education can be very significant in influencing the knowledge of children about food and its effects on their health. Intervention programs on nutrition based on curriculum can be implemented to educate children about the nutritional content of food and the benefits of portion control, as well as the value of a healthy diet, which can be applied to encouraging students to eat healthier foods in and out of school. Efforts to promote healthier lifestyles are further facilitated by school-based programs that would improve physical activity, like mandatory PE classes, recess, and active transportation programs. Such programs not only contribute to the prevention of childhood obesity but also enhance the physical fitness, cognitive growth, and social health in general [13].
Yet, the effective implementation of these school-based interventions is possible only in the case of several important challenges. As an example, in most places, resources are not enough to offer proper nutrition or PE programs. Such initiatives may fail because of poor financial support and untrained staff. Also, the cultural preferences, socioeconomic barriers, and the inability to find healthy food choices in certain communities may complicate the process of implementing meaningful change. The intervention in schools should consequently be flexible to the local contexts, involve all the stakeholders (parents, teachers, and policymakers), and be institutionalized to be effective. Interventions in the areas with Indigenous people should also be culturally sensitive and involve the voices and cultures of the communities in order to make the programs relevant to children and families [14-15].
Table 2: Life-Course Prevention Strategies for Obesity
| Life Stage | Key Interventions | Analytical Interpretation |
Prenatal and Early Life | Maternal nutrition support, gestational weight management, breastfeeding promotion | Early-life interventions modify biological programming and reduce intergenerational transmission of obesity risk, offering high long-term population returns |
| Childhood | School meal standards, nutrition education, physical education, family engagement | School-based strategies influence dietary and activity norms during critical developmental periods, shaping lifelong behaviors and reducing early obesity onset |
| Adolescence | Active transport initiatives, regulation of food marketing, peer-based programs | Adolescent-focused interventions address increasing autonomy and exposure to obesogenic environments, mitigating risk during a high-vulnerability transition stage |
| Adulthood | Workplace wellness programs, primary care counseling, community-based activity promotion | Adult interventions emphasize weight maintenance and metabolic risk reduction, though their effectiveness depends on supportive policy and environmental contexts |
Adult and Workplace Prevention
The prevention of obesity as people grow up moves more towards healthy lifestyles, which are in the clinical, workplace, and community-based settings. Adulthood is one of the stages when most people encounter various stressors, such as work-related factors, family issues, and financial factors, and all these factors may affect food consumption and exercise rates. Obesity prevention programs based in the workplace are especially promising since they are able to reach a considerable number of adults in an environment where they spend a considerable amount of time. Physical exercise (e.g., gym access, walking meetings, and similar), healthy eating (e.g., healthy snacks or subsidizing healthy lunch options), and stress management strategies [16] are common components of a wellness program at the workplace.
It has been proven that health programs in the workplace can help a lot in enhancing employee health, decreasing the number of absenteeism, and even saving on health insurance. These programs are not only useful in ensuring people have healthy weights but also create a healthy culture in organizations, which translates into long-term positive results for both the individuals and the employers [17].
There is also a role of clinical intervention in the prevention of obesity among adult populations. Healthcare providers, especially those in primary care units, can prevent and control obesity through providing nutritional, physical, and behavioral change counseling. In spite of the established advantages, most healthcare practitioners document the obstacles to the integration of physical activity promotion in standard practice, including time, training, and the absence of healthcare system support [16]. In order to overcome these barriers, health systems must strive to demonstrate that providers get sufficient training on how to deal with obesity and provide resources to assist patients in changing their lifestyles.
Another key obesity preventive intervention among adults is community-based interventions. They can consist of local programs promoting walking, biking, or active transportation, and programs promoting the availability of healthy foods at the farmers' market or community gardens. These programs will increase physical activity and healthy eating among adults, particularly those who live in low-income communities and have more obstacles to living healthier lifestyles [17] (Table 2).
Interpretive Commentary
The prenatal and early-life intervention is one of the most cost-effective prevention methods of obesity, as it has an impact on metabolic processes and behavioral patterns before the risk is internalized [12].
In the context of childhood, schools serve as important policy gateways, enabling fair access among the groups of people and promoting healthy norms regardless of the socioeconomic standing of households [13,15].
During the phase of adolescent development, the focus of preventive efforts should consider the increasing independence and vulnerability to marketing, and in this respect, the regulation and environmental strategy prove to be especially essential [14].
In adults, prevention of sustained obesity can only be achieved by uniting efforts on healthcare, workplaces, and communities since individual-level interventions are too limited in their long-term effects without the support of structures [16-17].
Policy Approaches to Reducing Obesity
Food and Nutrition Policies: Food and nutrition policies are the core in population-level activities to prevent obesity. These are the policies aimed at improving the food environment, making healthier diets easier, more affordable, and more available whereas they discourage the use of food products with a high amount of calories and low nutrient content. Taxation of sugar-sweetened beverages (SSBs) is one of the most frequent areas of research. Recent research, such as modeling in California, has shown that the excise taxes on SSBs may be highly effective to both reduce consumption and have positive health outcomes at the population level by decreasing the prevalence of obesity and associated metabolic diseases [18]. The positive equity outcomes can also be linked to SSB taxes when created to advantage the lower-income groups as it can both decrease consumption by the high-risk populations and also raise revenue to fund health promotion programs.
The other important strategy is nutrition labeling. Traffic light system, front-of-pack labelling and health star rating avail the consumer with accessible information on the nutritional value of foods and enable them to make informed decisions regarding their diets. It has been found that this labeling can affect buying behavior and eventually create a change in the preference of the consumers towards healthier foods [19].
Another policy approach that is a critical one is food marketing regulation especially the marketing targeted at children. Children are very prone to marketing effects and watching adverts on vitamin rich foods with low nutritional content has been associated with the high intake and consumption of these food materials. One solution to alleviating obesogenic influences in the environment of children is to implement regulations that curb or even ban promoting unhealthy foods to children, which would promote healthier dietary choices, and reduce the risk of obesity in the long run [19]. These food and nutrition policies combined together result in the conditions of structure that will promote healthier eating behaviors at the population level (Figure2).
Table 3: Policy Instruments and Obesity-Related Outcomes
| Policy Type | Policy Instrument | Analytical Interpretation of Obesity-Related Outcomes |
| Fiscal | Sugar-sweetened beverage taxation | Alters price signals to discourage consumption of high-sugar products, leading to measurable reductions in intake and potential long-term declines in obesity prevalence |
| Regulatory | Front-of-pack nutrition labeling | Improves consumer awareness and accountability among manufacturers, shifting purchasing behavior toward healthier options when labels are clear and standardized |
| Regulatory | Restrictions on food marketing to children | Reduces early-life exposure to obesogenic messaging, supporting healthier preference formation and lowering childhood obesity risk |
| Environmental | Active transport infrastructure | Embeds physical activity into daily routines, producing sustained increases in population-level energy expenditure |
| Environmental | Urban design and land-use planning | Reshapes built environments to support active living, particularly in dense urban settings where behavioral change is otherwise constrained |
| Behavioral (Nudge) | Healthy default options in public institutions | Influences choice without restricting autonomy, increasing uptake of healthier foods through low-cost, scalable interventions |
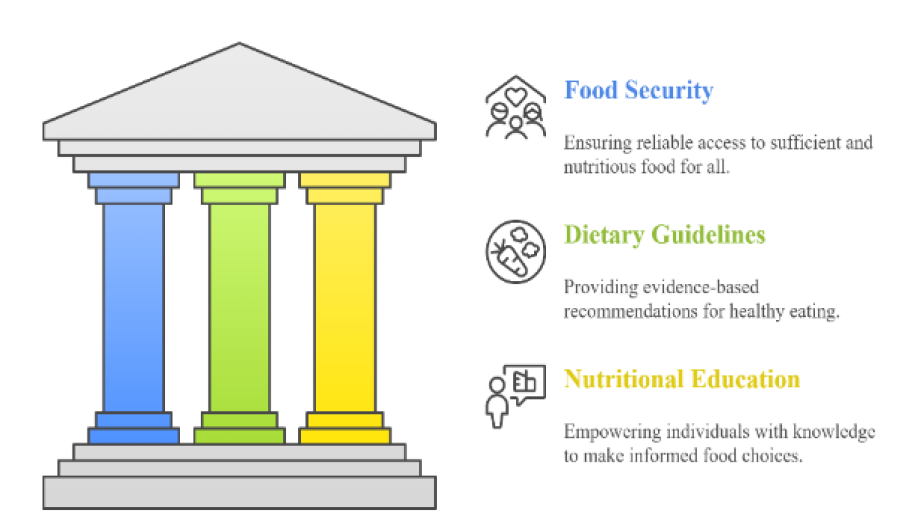
Figure 2: Food and Nutrition Policies
Physical Activity and Built Environment Policies
Environmental and urban design policies that encourage physical activity are beginning to be seen as a necessary part in the prevention of obesity. The policies that are actively implemented in a community can boost the daily physical activity of the population and decrease the use of transport options that are inactive, like the establishment of safe walking and cycling routes, bonuses to walk or ride to work, and the development of public transportation, among others [20].
The design of the built environment and urban planning are also important factors of influence in the development of activity pattern. Green spaces, parks, recreation and walking friendly areas allow people to move regularly and live healthier lives. Community level Obesity rates would be significantly impacted at the community-level by the urban design that incorporates physical activity into everyday life physical activity through mixed-use development, improved connectivity, and the proposed safety environment [21].
The promotion of physical activities needs a multisectoral approach, including city planners, transportation authorities, schools, and healthcare systems, to be scaled up. Programs, which incorporate both community involvement, environmental change and policy reinforcement, will have a better chance of generating sustainable behavior change. It has been indicated that infrastructure modification can be used in tandem with educational and behavioral interventions to increase the efficacy of population-level physical activity policies [20-21].
Behavioral and Nudge-Based Policies
New policy instruments such as behavioral economics and nudge strategies have become possible tools of obesity prevention. The objective of nudges is to indirectly make people make better health decisions without limiting their freedom of choice using knowledge of psychology and behavioral science. An example is the application of choice architecture in the cafeteria or retail place, like stocking healthier food at the eye level, making the proportion of different food items smaller by default, or using prompts to motivate exercise [22].
Regulations and incentives can also be implemented at bigger scales and applied in policy nudges to influence the behavior indirectly. As an example, governments may impose incentives on supermarkets to stock healthier products, provide tax incentives to take up activities that are active transportation, or promote workplace initiatives that can help people move around on a daily basis. The above methods are inexpensive, can be expanded, and may be more palatable to the population than restrictive measures since they maintain independence but promote better health [22] (Table 3).
Interpretive Commentary
Sugar-sweetened beverage taxes are viewed as a potent form of population-wide instrument because of their capacity to alter consumption habits via economic incentives and not personal persuasion [18].
Information asymmetries are addressed by regulatory actions such as food labeling and marketing prohibitions that guard vulnerable populations against the commercial causes of obesity, particularly children [19].
The environmental policies are able to tackle the structural barriers to physical activity by ensuring that movement becomes part of the daily environment, and they provide a lasting impact compared to behavior change interventions [20].
Nudge-based solutions are consistent with conventional regulation in that they can influence the decisions made without limiting freedom of choice, thereby being politically acceptable and ethically justified inclusions in the obesity policy portfolios [22].
Global and Regional Perspectives
High-Income vs Low- and Middle-Income Countries: Obesity is no longer the province of high-income nations, but it has become a health problem facing the world. Nevertheless, there is often a variation between the context, drivers, and consequences of obesity in high-income countries (HIC) and low- and middle-income countries (LMIC). The prevailing causes of obesity in HICs are usually sedentary lifestyles, excessive consumption of food rich in calories, and multifaceted social determinants, but in LMICs, it is economic progression, urbanization, and changes in nutrition that lead to a dual burden of malnutrition, i.e., undernutrition and obesity coexist in the same population or even in the same home [9,23].
A combination of malnutrition and obesity offers special challenges posed by LMICs. Although the current public health policies should not ignore the issues of undernutrition, they should also ensure that the rate of overweight and obesity among children and young adults is not increasing. Nutrition changes in these nations can be characterized by a change in dietary habits of people consuming large amounts of whole grains, fruits, and vegetables, to the foods that are energy-dense, ultra-processed, and high in sugar, salt, and bad fats. Such eating habits, along with a decreased physical activity level caused by urbanization and sedentary jobs, add to the rise in the number of obese people [9].
The issue is aggravated by rapid urbanization in LMICs that changes lifestyles and food environments. In cities, there is usually easier access to cheap, high-calorie processed foods, and at the same time, a partial lack of exercise in the form of poor infrastructure, unsafe streets, or a lack of green areas. Conversely, interventions aiming to combine urban planning, active transport, and public health policies to reduce the effects of sedentary lifestyles are in the spotlight of the majority of HICs addressing obesity in the world, making context-specific interventions a highly important issue [23].
Therefore, the prevention of obesity interventions should be adapted to the specific epidemiological and socioeconomic situations of specific nations. Although HICs might focus more on changing the status quo of existing obesogenic environments and preventive healthy behavior, LMICs still have to find the balance between undernutrition and obesity prevention, often with limited resources and a high pace of social transformation.
Global Governance and Policy Coordination
The obesity epidemic is complex and requires a coordinated global response and participation of various sectors. The World Health Organization (WHO), the Food and Agriculture Organization (FAO), and the United Nations Children Fund (UNICEF are international organizations that are essential in forming policies, offering technical advice, and developing international standards on obesity prevention and nutrition. These organizations assist the countries in the use of evidence-based interventions, progress monitoring, and best practice exchange. Policy development and multisectoral cooperation are outlined by such global efforts as the WHO Global Action Plan on the Prevention and Control of Noncommunicable Diseases [23].
The collaboration across the sectors is required since obesity is not only a health sector determinant, but also affects agriculture, trade, urban planning, education, and finance. The impacts of policies in one sector are either direct or indirect on the outcomes of obesity- i.e., agricultural subsidies can have an effect on the affordability and availability of unhealthy foods, whereas urban planning policies can have an effect on the availability of physical activity. Good governance necessitates the incorporation of the public health goals in various sectors of policy, stakeholder coordination across different levels, and the culture and economy of the interventions [9].
In addition, international coordination can assist LMICs in using HIC technical know-how, financial resources, and policies, and reflect the solutions to local needs. The collaboration at the cross-border level is supported by the efforts of regional food policy networks, knowledge-sharing, and international cooperation, which help countries to make evidence-based interventions to prevent obesity at the national level. Global governance mechanisms can be effective in improving the effectiveness, sustainability, and equity of the prevention of obesity all around the world by encouraging the use of a common strategy.
Health Equity, Ethics, and Social Justice
Obesity Inequities: Obesity is not simply an issue of personal lifestyle behaviors, but rather it is strongly connected with social determinants of health, and thus it creates severe inequity among the population groups. Not only across the world, but also in the United States, socioeconomic gradients in obesity exist, with people on the lower income or marginalized side of the population experiencing a disproportionately greater disposition to overweight and obesity than people on the more affluent side of the population. These differences are a product of a set of environmental, economic, and social factors that limit access to healthy food and physical exercise. As an example, low-income areas usually lack access to fresh fruits and vegetables, have a higher concentration of fast-food restaurants, and safe physical activity areas, which together produce obesogenic environments [6,24].
There are particularly vulnerable populations. The disadvantaged children have higher chances of eating poor nutrient rich calorie rich diets because of affordability and accessibility limitations, and are prone to obesity in their lives. Historical inequities that impact food security, cultural eating habits, and access to medical care are usually subjected to the ethnic minorities and Indigenous populations. Women, especially in low-income environments, can encounter more obstacles because of taking care of children, lack of control, and social practices that deny them the opportunity to engage in physical activities [25].
Besides, the consequences of the inequity of obesity are not confined to physical well-being. Disproportionate levels of obesity among the disadvantaged population facilitate social stigmatization, decreased educational and employment chances, and heightened mental distress, which subsequently support health inequalities. To overcome such inequities, the approach that focuses on particular individuals is insufficient to apply structural solutions. There should be policies on the never-ending determinants, which include food affordability, meal quality at schools, urban design and social protection initiatives to develop the environment to empower everyone, especially individuals in high-risk groups, to adopt healthier lifestyles. Policies that are ethically driven, but maximally effective at the population level, are driven by equity concerns but also focus on populations that are disadvantaged because such interventions have high potential to increase the disparities instead of minimizing them.
Ethical Considerations in Obesity Policy
Besides the issue of inequities, effective policies on obesity should also take into consideration ethical principles so as to make sure that interventions are just, equitable, and acceptable in society. The prevention of stigma and discrimination is one of the significant ethical issues. Implicitly blaming people as the cause of obesity in a public health campaign or policy measure may create and maintain harmful stereotypes, decrease self-efficacy, and deteriorate mental health outcomes. Indicatively, a message that puts obesity as individual failure instead of a social and environmental phenomenon may drive away even the people, to whom interventions are meant to reach. Instead, the policies must aim at developing favorable environments that assist in resolving structural causes of obesity, including by enhancing access to healthy foods, active living, and unhealthy marketing habits [6].
The other major factor is respecting autonomy. Although the policies of the public health can be used to coerce people into healthier behavior, they must not be used to inhibit choice. An example is that fiscal policies, such as the taxation of sugar-sweetened beverages or subsidies of more nutritious foods, do not force people to purchase something, but instead, give them a chance to make a rational choice in favor of the larger health common goals. Equally, the marketing of unhealthy foods to children can be controlled by the creation of laws that will safeguard the susceptible group without infringing on the freedom of choice by adults. Through a mixture of directions, encouragements, and modifications of the environment, the policymakers will be able to strike a balance between health objectives of the population and the consideration of individual rights.
The allocation of benefits and burdens should also be taken into account with the equity-oriented policies. Policies that impact the poor in a disproportionate manner without offering compensatory mechanisms may unwillingly create inequalities. As an example, although unhealthy food can be made less appealing by taxing it, this will create an increased financial strain on the low-income households unless accompanied by subsidies or healthy options. Ethical policies are hence made to incorporate equity issues at an early stage making interventions effective and fair (Figure 3).
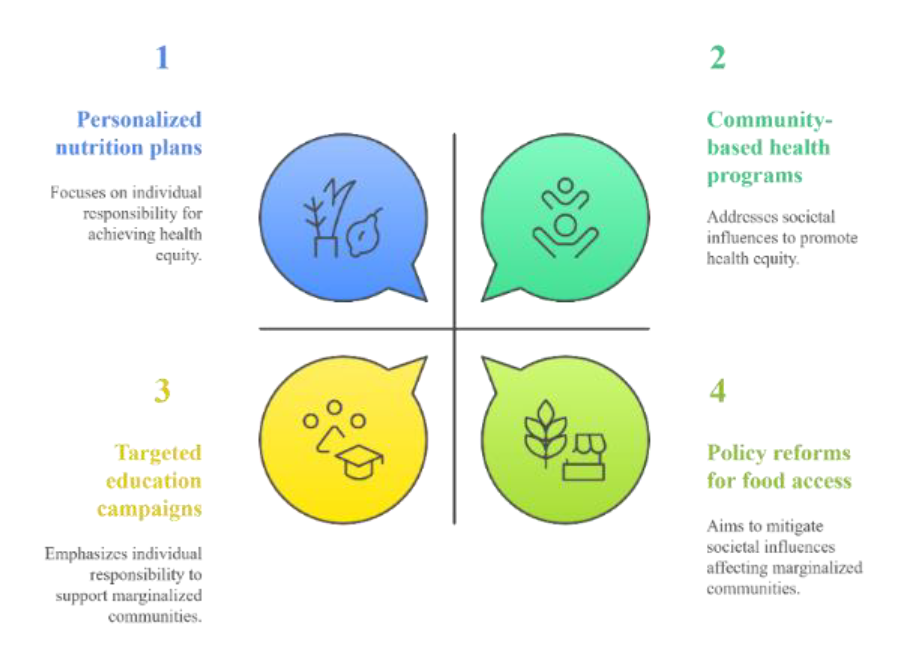
Figure 3: Ethical Considerations in Obesity Policy
Integrating Equity and Ethics into Policy Design
To adopt a holistic attitude towards the issue of obesity it is necessary to ensure that equity and ethics are incorporated in the policy cycle: in terms of design, implementation and evaluation. Policymakers should:
Determine at-risk groups and determine the impact that proposed interventions could have on them
Involve communities in policy formulation to make the policies culturally appropriate and sensitive to community needs
Integrate both structural and behavioral interventions, including healthy food subsidies, and safe recreational areas and nudges in the retail and school environment
Track to make sure that the interventions narrow gaps instead of expanding them unintentionally
Combining these principles would enable the strategies applied in the area of obesity prevention to be more effective and inclusiveness, fairness, and social justice
Table 4: Equity-Oriented Policy Considerations
| Equity Issue | Policy Response | Analytical Interpretation of Expected Impact |
| Low-income populations | Food subsidies for fruits and vegetables | Reduces economic barriers to healthy diets, improving nutritional quality and narrowing socioeconomic obesity gaps |
| Children and adolescents | Restrictions on unhealthy food marketing | Limits exposure to persuasive marketing during critical developmental periods, supporting healthier preference formation and long-term obesity prevention |
| Marginalized communities | Investment in safe recreational spaces | Addresses environmental inequities by enabling physical activity in underserved neighborhoods |
| Racial and ethnic minorities | Culturally tailored nutrition policies | Enhances policy relevance and effectiveness by aligning interventions with cultural food practices and community norms |
| Rural populations | Improved food retail and transport access | Mitigates geographic isolation that restricts access to affordable, healthy foods, reducing structural obesity risk |
Interpretive Commentary
Table 4 points out the key position of policies based on equity in compensating for the imbalanced distribution of the risk of obesity among the populations. The table illustrates that the best way to prevent obesity is through structural interventions instead of focusing mostly on individual intervention by behavior change.
An example of policies that deal explicitly with accessibility barriers, which are a major cause of dietary inequalities and obesity disparities, is food subsidies for low-income populations. These measures can reduce socioeconomic levels of obesity occurrence by enhancing access to healthy foods.
Several marketing bans targeting children and teenagers are most effective since they can target the life course at an earlier stage and lower the exposure of children to commercial determinants of obesity at critical stages of preference and habit formation. This type of policy promotes long-term population health improvement and guards vulnerable populations.
The provision of secure recreational areas in marginalized neighborhoods is a method of mitigating environmental disparities that constrain physical exercise. These interventions recognize that people often physically do not do so because of unsafe or under-resourced neighborhoods, and not as a choice.
Lastly, culturally relevant nutrition policies and rural population access to improved food make prevention of obesity relevant, acceptable, and sustainable. Collectively, these equity-based strategies affirm the value of the argument that lessening the global burden of obesity cannot be achieved without the promotion of social justice and health equity.
Implementation Challenges and Policy Barriers
The increasing worldwide obesity epidemic places a lot of emphasis on the pressing necessity of a progressive approach that is not only holistic but also sustainable. Although much has been done to find effective interventions, the multifactorial complexity of obesity requires combined strategies that tackle the structural, environmental and social factors underlying this problem. Based on the evidence available and lessons learnt in the successful interventions, there are various directions that can be identified that the policy can be developed in future.
Integrated Food System Reform
An attempt to reform food systems to enable healthier eating patterns on a large scale should be a priority of future obesity prevention work. This involves transformation of agricultural production, food distribution and retail settings to render nutritious foods more affordable, accessible, and culturally ready. The population dietary patterns can be changed to more nutritious options through such strategies as incentivizing the production of fruits, vegetables, and whole grains and regulations on the availability of ultra-processed food [9,11].
Moreover, nutrition should be taken into consideration when developing trade and agricultural policies: this will help to make sure that the economic incentives correspond with the public health goals. As an illustration, the subsidies given to high-energy crops like commodity foods at the expense of nutritious foods can be redesigned to promote healthy eating. Marketing practices especially those that target children should also be dealt with by policy measures in order to curb exposure to unhealthy food advertisements. To fully reform the food system, there is a need to have cross-sector coordination between agriculture, trade, health, and education sectors to establish sustainable and conducive conditions of healthy eating (Figure 4).
Figure 4: Integrated Food System Reform
Stronger Governance and Multisectoral Coordination
Obesity prevention is a complicated issue that requires effective governance body and concerted efforts at various levels and spheres of the state. Policymakers must be able to formulate combined policies connecting health and urban planning policies, education policies, transport policies, as well as fiscal policies, which have consistent and complementary interventions. Policy coherence, resource efficiency, and accountability may be achieved with the help of multisectoral task forces, interagency committees, and public-private partnerships [23].
Good governance also entails strong monitoring and evaluation systems to follow through implementation process, measure results and inform repetitive changes in policies. Long-term impact can only be maintained by transparency in decision-making, involvement of stakeholders and legal frameworks to protect the best interests of the population to prevent commercial or political interests.
Equity-Centered Prevention Strategies
Such inequity of obesity reduction should be the core of future prevention. The vulnerable populations targeted in policies should explicitly address low-income groups, children, ethnic minorities, and other socially marginalized groups in order to make interventions not contribute to widening the disparities [6,24].
The strategies that can be equity-oriented are the selective subsidies to healthy foods, the increased availability of safe sport areas in the impoverished communities, and culturally sensitive programs in schools. Moreover, the interventions must consider the community involvement and local knowledge to make it relevant, acceptable and sustainable. The inclusion of equity concerns in the design phase to the assessment stage enables policymakers to achieve optimal health outcomes and social justice to develop a more inclusive approach to obesity prevention.
Evidence-Informed Policy Making
The strict scientific evidence and the adaption to the local contexts should inform the future policies. Evidence-informed policymaking involves conducting systematic reviews of research on effective interventions by taking into account their feasibility and scalability and incorporating the experiences of other past efforts. Potentially beneficial insights regarding the effects of interventions on the population health and equity can be developed through modeling studies, natural experiments, and pilot programs [26].
Notably, the policies must be dynamic and adaptable to the changing trends, dietary habits, physical activity, and economic status. By combining real-time information, surveillance systems, and participatory assessment structures, policymakers can improve interventions and respond to unforeseen results, as well as make interventions pertinent and workable over a period of time. Also, policymakers, health workers, and community leaders should be invested in capacity building to enhance the development of evidence into actionable policies.
Summary of Policy Recommendations
To conclude, the future of obesity prevention is one with a holistic, multifaceted, and equity-based model. The main recommendations will be:
Integrated Food System Reform: Respond to public health by aligning agricultural, trade and marketing policies with their aims and purposes
Greater Governance: Multisectoral coordination, transparency in decision-making and effective monitoring should be launched to make policies more coherent and sustainable
Equity-Centered Prevention: Develop programs that put vulnerable communities at the focal point, integrate communities and minimize health disparities
Evidence-Based Policymaking: Found policies on high-quality research, tailor the strategies to the local conditions, and provide a continuous system of monitoring and evaluating the results to maximize the outcomes
These suggestions can enhance the efficiency of obesity prevention activities, decrease the world burden of disease, and ensure health equity by governments, international organizations, and other stakeholders. These progressive plans would be necessary in creating robust health systems of the population that would overcome the complexities of obesity in the XXI century.
Obesity is a global issue that is on the increase and presents a great threat to the population's health, economic development, and social justice. This paper has revealed the complexity of obesity, and it is of great significance due to the life-course preventive measures alongside policy-based interventions and equity-based measures that can reduce its incidence. Interventions in early life and by the mother, programs in schools and adolescence, workplaces, and community promotion, are all indicative that preventive interventions need to be implemented throughout the lifespan to be sustainable. Such complementary policy measures as food and nutrition policies, physical activity and built environment policies, and behavioral nudges also support the individual and population-level measures, providing an environment where healthier options are more likely to be taken.
The need to deal with the problem of obesity cannot be overemphasized. The increasing prevalence in both high-income and low- and middle-income countries, the twin burden of malnutrition and rising healthcare expenditures, demonstrate the urgency of the issue and the use of evidence-based measures to address the problem. The deficiencies of implementation, like political opposition, industry pressure, resource limitation, and sustainability of the policy used, emphasize the fact that the problem of obesity cannot be solved by isolated actions: it needs a multisectoral and integrated approach.
An international response is thus justified. The development of an integrated food system reform, a stronger governance system, equity-based approaches, and evidence-based policymaking are key to effective obesity prevention that is facilitated by international cooperation and adaptation at the local level. Countries can address the health, social, and economic impacts of obesity by harmonizing policies in the health, education, agriculture, and urban planning sectors and focusing on the most vulnerable populations. Finally, in addition to being a public health imperative, the need to reduce the global burden of obesity is a vital move towards other more important objectives of health equity, social justice, and sustainable development.
Kelly T. et al. “Global burden of obesity in 2005 and projections to 2030.” International Journal of Obesity, vol. 32, no. 9, 2008, pp. 1431–1437.
Chong B. et al. “Trends and predictions of malnutrition and obesity in 204 countries and territories: An analysis of the Global Burden of Disease Study 2019.” EClinicalMedicine, vol. 57, 2023.
Chew N.W.S. et al. “The global burden of metabolic disease: Data from 2000 to 2019.” Cell Metabolism, vol. 35, no. 3, 2023, pp. 414–428.
Seidell J.C. and Halberstadt J. “The global burden of obesity and the challenges of prevention.” Annals of Nutrition and Metabolism, vol. 66, 2015, pp. 7–12.
Ramos Salas X. et al. “A critical analysis of obesity prevention policies and strategies.” Canadian Journal of Public Health, vol. 108, nos. 5–6, 2017, pp. e598–e608.
Kumanyika S.K. “Advancing health equity efforts to reduce obesity: Changing the course.” Annual Review of Nutrition, August 2022.
Sobal J. et al. “A conceptual model of the food and nutrition system.” Social Science and Medicine, vol. 47, no. 7, 1998, pp. 853–863.
Mao W. and Agyapong V.I.O. “The role of social determinants in mental health and resilience after disasters: Implications for public health policy and practice.” Frontiers in Public Health, May 2021.
Pingali P. and Sunder N. “Transitioning toward nutrition-sensitive food systems in developing countries.” Annual Review of Resource Economics, October 2017.
Gillespie S. and van den Bold M. “Agriculture, food systems, and nutrition: Meeting the challenge.” Global Challenges, April 2017.
Nordhagen S. et al. “Integrating nutrition and food safety in food systems policy and programming.” Global Food Security, March 2022.
Chen C. et al. “Estimated global overweight and obesity burden in pregnant women based on panel data model.” PLoS ONE, vol. 13, no. 8, 2018.
Totura C.M.W. et al. “Assessing implementation of evidence-based childhood obesity prevention strategies in schools.” Preventive Medicine Reports, vol. 2, 2015, pp. 347–354.
Almutairi N. et al. “Barriers and enablers to the implementation of school-based obesity prevention strategies in Jeddah, KSA.” International Journal of Qualitative Studies on Health and Well-Being, vol. 17, no. 1, 2022.
Pigford A.A.E. et al. “Using First Nations children’s perceptions of food and activity to inform an obesity prevention strategy.” Qualitative Health Research, vol. 22, no. 7, 2012, pp. 986–996.
Albert F.A. et al. “Physical activity promotion: A systematic review of the perceptions of healthcare professionals.” International Journal of Environmental Research and Public Health, June 2020.
Silva C.S. et al. “Predictors of physical activity promotion in clinical practice: A cross-sectional study among medical doctors.” BMC Medical Education, vol. 22, no. 1, 2022.
Lee M.M. et al. “A sugar-sweetened beverage excise tax in California: Projected benefits for population obesity and health equity.” American Journal of Preventive Medicine, vol. 66, no. 1, 2024, pp. 94–103.
Levi R. et al. “Nutrition standards for the charitable food system: Challenges and opportunities.” BMC Public Health, vol. 22, no. 1, 2022.
Koorts H. et al. “Tensions and paradoxes of scaling up: A critical reflection on physical activity promotion.” International Journal of Environmental Research and Public Health, vol. 19, no. 21, 2022.
Swann C. et al. “Updating goal-setting theory in physical activity promotion: A critical conceptual review.” Health Psychology Review, vol. 15, no. 1, 2021, pp. 34–50.
Murayama H. et al. “Applying nudge to public health policy: Practical examples and tips for designing nudge interventions.” International Journal of Environmental Research and Public Health, March 2023.
Cominato L. et al. “Obesity prevention: Strategies and challenges in Latin America.” Current Obesity Reports, June 2018.
Vargas C.M. et al. “Health-equity issues related to childhood obesity: A scoping review.” Journal of Public Health Dentistry, vol. 77, 2017, pp. S32–S42.
Herbozo S. et al. “A call to reconceptualize obesity treatment in service of health equity: Review of evidence and future directions.” Current Obesity Reports, March 2023.
Ding S. et al. “Commodity market stability and sustainable development: The effect of public health policies.” Research in International Business and Finance, vol. 70, 2024.
