+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6056
ISSN (Online) : 2789-6064
Background: Otitis externa (OE), commonly referred to as "swimmer's ear," is an inflammation of the external auditory canal, primarily caused by bacterial infections. It is associated with risk factors such as swimming, mechanical trauma, and underlying dermatological conditions. This study aimed to evaluate the clinical presentation, risk factors, microbiological profile, and treatment outcomes of OE. Methods: This study was conducted over one year (June 2023 to May 2024), involving 126 patients diagnosed with OE. A detailed clinical assessment was performed, including demographic details, symptom presentation, risk factors, otoscopic examination, and microbiological analysis of ear swabs. Treatment outcomes were assessed at Day 7, Day 14, and 1 Month. Statistical analysis was performed using chi-square tests and logistic regression, with p-values <0.05 considered significant.Results: The mean age of patients was 34.2 ± 12.6 years, with 58.7% being males. The most common symptoms were ear pain (94.4%), pruritus (82.5%), and ear discharge (70.6%). The primary risk factors included swimming (48.4%), use of earphones/cotton buds (46.8%), and recent upper respiratory infections (35.7%). Pseudomonas aeruginosa (38.1%) was the predominant bacterial isolate, followed by Staphylococcus aureus (28.6%). Treatment with topical antibiotic-steroid ear drops showed significant improvement (p < 0.0001), with 87.3% of patients achieving complete resolution within one month. Recurrence was observed in 9.5% of patients, with swimming and earphone use significantly associated with recurrence (p = 0.047).Conclusion: This study confirms that Pseudomonas aeruginosa and Staphylococcus aureus are the predominant pathogens in OE, with swimming and mechanical trauma being major risk factors. Topical antibiotic-steroid therapy remains highly effective, with a low recurrence rate when risk factors are minimized. Preventive strategies, including avoiding water exposure and mechanical irritation, are essential for reducing disease burden.
Otitis externa, commonly referred to as "swimmer's ear," is an inflammation of the external auditory canal, predominantly resulting from bacterial infections.[1] The primary pathogens implicated are Pseudomonas aeruginosa and Staphylococcus aureus . This condition manifests with symptoms such as otalgia (ear pain), pruritus (itching), aural fullness, and, in some cases, otorrhea (discharge).[1]
The incidence of otitis externa is notable, with approximately 10% of individuals experiencing it at some point in their lives . Annually, it affects about 1% of the population, with a higher prevalence observed during the summer months, likely due to increased swimming activities . While it can occur across all age groups, certain demographics, such as children aged 5 to 9, are more susceptible.[2,3]
Several risk factors contribute to the development of otitis externa. Frequent exposure to water, especially in swimming, can lead to maceration of the ear canal skin, creating an environment conducive to bacterial growth.4 Mechanical trauma from the use of cotton swabs or hearing aids can disrupt the protective cerumen barrier, facilitating pathogen entry. Additionally, underlying dermatological conditions, such as eczema or psoriasis, and systemic factors like diabetes mellitus, can predispose individuals to this condition.[4,5]
Management of otitis externa primarily involves meticulous cleaning of the ear canal and the application of topical agents. Topical antibiotic or antiseptic eardrops, often combined with corticosteroids, are considered the first-line treatment for uncomplicated cases . Systemic antibiotics are generally reserved for situations where the infection extends beyond the ear canal or in patients with specific risk factors, such as diabetes or immunosuppression.[6]
Despite the availability of effective treatments, recurrence and chronicity remain concerns. Chronic otitis externa, defined as inflammation persisting for more than three months, can result from inadequately treated acute episodes or continuous exposure to predisposing factors.[7] Complications, although rare, can include hearing loss and, in severe cases, the spread of infection to adjacent structures,[8]
Given these considerations, this study aims to investigate the clinical presentation, risk factors, microbiological profile, and treatment outcomes of patients diagnosed with otitis externa. By analyzing data from a cohort of 126 patients over a one-year period at the Department of Otorhinolaryngology, SVS Medical College, Mahabubnagar, we seek to enhance the understanding of this condition and inform strategies to improve patient management and outcomes.
Study Design and Setting
This prospective observational study was conducted in the Department of Otorhinolaryngology at SVS Medical College Hospital, Mahabubnagar,Telangana,India, over a period of one year from June 2023 to May 2024. The study aimed to evaluate the clinical presentation, etiology, risk factors, microbiological profile, treatment outcomes, and recurrence rates in patients diagnosed with external otitis.
Study Population and Sample Size
A total of 126 patients who presented with external otitis were included in the study. The sample size was determined based on patient inflow and feasibility within the study duration.
Inclusion Criteria
Patients aged five years or older who were diagnosed with external otitis based on clinical findings were included in the study. Only those who provided informed consent for participation were considered. Patients with either unilateral or bilateral external otitis were eligible.
Exclusion Criteria
Patients diagnosed with chronic otitis media, those with immunocompromised conditions such as uncontrolled diabetes or HIV, and individuals with a history of recent ear surgery were excluded from the study. Patients on long-term ototopical medications were also not included.
Data Collection
Demographic and Clinical Profile
A detailed clinical evaluation was performed for each patient presenting with symptoms of otitis externa (OE), and all findings were systematically recorded in a structured case record form (CRF). This structured format ensured uniformity in data collection and minimized observer bias.
Demographic Data Collection
Each patient’s demographic details were meticulously documented, including:
Age: The patient's age at the time of presentation was recorded to analyze age-related trends in the occurrence of OE.
Gender: The gender distribution was documented to determine whether OE exhibits a gender predisposition.
Occupation: Patients’ occupations were noted to evaluate whether occupational exposure to water, dust, or environmental pollutants contributed to the condition.
Socioeconomic Status: Information on socioeconomic background was gathered using standard classification systems. This was relevant because hygiene practices, access to healthcare, and awareness of ear care might vary based on socioeconomic status.
Clinical Symptomatology and Disease Characteristics
A comprehensive history of presenting symptoms was obtained to establish a pattern of disease presentation. The primary symptoms assessed included:
Ear Pain (Otalgia): Patients were asked about the onset, duration, and intensity of pain, whether it was constant or intermittent, and if it worsened with auricle manipulation or tragal pressure.
Pruritus (Itching): The degree of itching in the external ear canal was assessed, as it often precedes bacterial or fungal infection in OE.
Otorrhea (Ear Discharge): The color, consistency, and odor of ear discharge were documented to differentiate between bacterial (purulent), fungal (white/black debris), and other non-infectious causes.
Hearing Loss: The presence and severity of hearing impairment were evaluated. Conductive hearing loss may occur due to swelling, debris accumulation, or excessive cerumen.
Ear Fullness and Swelling: Sensations of ear blockage and visible swelling of the external auditory canal were noted.
Laterality: The unilateral or bilateral involvement of OE was documented. Unilateral cases are more common, but bilateral infections may suggest fungal etiology or underlying systemic conditions.
In addition, patients were asked if they had experienced previous episodes of OE to assess for potential chronicity or recurrence.
Risk Factor Assessment
OE is a multifactorial condition, and identifying risk factors is critical for both treatment and prevention. Each patient was systematically interviewed about potential predisposing factors, including:
1. Water Exposure and Swimming
Patients were asked about their history of swimming, frequency of exposure to water, and use of ear protection (earplugs or swim caps). Swimming pools, freshwater lakes, and humid environments are well-established risk factors for OE due to prolonged moisture exposure, which disrupts the ear canal's protective cerumen barrier, leading to bacterial overgrowth.
2. Use of Earphones, Hearing Aids, or Cotton Buds
The habit of inserting objects into the external ear canal was extensively assessed.
Earphones and Hearing Aids: Prolonged use of in-ear devices creates a warm, humid environment, promoting microbial growth.
Cotton Buds and Foreign Body Insertion: Excessive ear cleaning with cotton buds, bobby pins, or matchsticks can cause microabrasions, predisposing the ear canal to infection.
3. Upper Respiratory Tract Infections (URTIs)
Patients were asked about any recent or concurrent upper respiratory infections (URTIs), including sinusitis, rhinitis, or pharyngitis. The close anatomical connection between the external ear, Eustachian tube, and nasopharynx suggests that URTIs can contribute to secondary infection of the external auditory canal.
4. History of Ear Trauma or Dermatological Conditions
Self-induced trauma: Scratching the ear canal with fingernails or sharp objects can introduce bacteria, leading to localized inflammation or infection.
Underlying dermatological conditions: Patients with eczema, psoriasis, or seborrheic dermatitis were noted, as these conditions can lead to excessive dryness, flaking, and secondary infection of the ear canal.
All collected data were correlated with microbiological findings to assess their significance in disease pathogenesis and recurrence risk.
Otoscopic and Clinical Examination
A thorough otoscopic examination was performed on all patients to confirm the diagnosis and determine the extent of infection and inflammation.
Findings Noted During Otoscopic Examination
Edema and Erythema: The degree of swelling and redness of the external auditory canal (EAC) was documented, as mild edema indicates early infection, whereas severe swelling with obstruction suggests advanced disease.
Presence of Discharge or Debris:
Thick, yellow-green discharge suggested bacterial infection, likely caused by Pseudomonas aeruginosa.
White, cotton-like debris or black fungal spores indicated fungal etiology, such as Aspergillus or Candida species.
Tenderness on Tragal Pressure and Auricular Manipulation: Pain upon pressing the tragus or moving the auricle is a hallmark of bacterial otitis externa and was recorded in all patients.
Integrity of the Tympanic Membrane (TM): The tympanic membrane was carefully inspected to rule out perforations or middle ear involvement. In cases of significant debris, aural toilet was performed for better visualization.
Findings from the otoscopic examination guided treatment decisions, including the selection of appropriate topical antibiotics, antifungals, or anti-inflammatory agents.
Microbiological Analysis
Sample Collection and Processing
Sterile ear swabs were collected from patients with:
Active discharge (suggestive of bacterial infection).
Visible fungal elements or persistent pruritus (suggestive of fungal infection).
Severe inflammation or non-resolving cases, where antibiotic resistance was suspected.
The collected specimens were sent for comprehensive microbiological analysis, including:
1. Gram Staining
Gram staining was performed to differentiate bacterial pathogens:
Gram-negative rods (e.g., Pseudomonas aeruginosa)
Gram-positive cocci (e.g., Staphylococcus aureus)
Polymicrobial infections were noted when both Gram-positive and Gram-negative bacteria were present.
2. Potassium Hydroxide (KOH) Mount
KOH wet mount was used to identify fungal elements:
Septate hyphae indicated Aspergillus species.
Budding yeast cells suggested Candida infection.
3. Bacterial Culture and Antibiotic Sensitivity Testing
Bacterial cultures were performed using blood agar and MacConkey agar to isolate and identify bacterial pathogens. Antibiotic susceptibility testing was conducted using the Kirby-Bauer disk diffusion method to guide targeted antibiotic therapy.
4. Fungal Culture
Sabouraud’s Dextrose Agar (SDA) was used to culture fungal pathogens. Growth of Aspergillus, Candida, or other molds was confirmed with microscopic examination.
Treatment and Follow-up
Patients were managed based on the severity of their condition. Mild cases were treated with topical antibiotic-steroid ear drops, while moderate to severe cases received a combination of topical and systemic antibiotics, antihistamines, analgesics, and antifungals if required. Patients with abscess formation or canal obstruction underwent aural toileting, wick placement, and drainage as necessary.
Follow-up assessments were conducted at day seven, day fourteen, and one month after treatment initiation. On day seven, symptom resolution and inflammation were assessed. On day fourteen, treatment efficacy was evaluated, and therapy was adjusted if required. At the one-month follow-up, recurrence rates and patient compliance were monitored.
Outcome Measures
Primary Outcome Measures
The primary outcome measures included symptom resolution within 14 days, identification of the microbiological profile, and assessment of treatment effectiveness.
Secondary Outcome Measures
Secondary outcomes included recurrence rates within six months, the occurrence of complications such as persistent inflammation or hearing loss, and patient compliance with treatment.
Ethical Considerations
The study was approved by the Institutional Ethics Committee of SVS Medical College before initiation. Informed consent was obtained from all participants, and for minors, consent was taken from their guardians. Patient confidentiality was maintained throughout the study, and all procedures adhered to ethical guidelines.
Statistical Analysis
Descriptive statistics were used to analyze demographic and clinical variables. Categorical variables such as gender, occupation, and risk factors were compared using the chi-square test, while continuous variables such as symptom duration were analyzed using independent t-tests. Multivariate logistic regression was performed to assess risk factors for recurrence. A p-value of less than 0.05 was considered statistically significant.
Demographic and Clinical Characteristics (Table 1)
The study population consisted of 126 patients diagnosed with external otitis. The mean age was 34.2 ± 12.6 years, with the majority falling in the 15–29 years age group (31.0%), followed by the 30–44 years age group (27.8%). The incidence of external otitis was higher in males (58.7%) compared to females (41.3%), which may be attributed to greater outdoor activities, increased use of earphones, and more frequent exposure to potential risk factors such as swimming and workplace noise. However, statistical analysis using the chi-square test revealed no significant association between external otitis and age or gender (p = 1.000), indicating that the condition affects individuals across different age groups and genders without any specific predisposition.
Table 1: Demographic Characteristics of Patients with External Otitis
Characteristic | n (%) | p-value |
Total patients | 126 (100%) | - |
Age Group (years) | 1.000 | |
5–14 | 18 (14.3%) | |
15–29 | 39 (31.0%) | |
30–44 | 35 (27.8%) | |
45–59 | 23 (18.3%) | |
≥60 | 11 (8.7%) | |
Gender | 1.000 | |
Male | 74 (58.7%) | |
Female | 52 (41.3%) |
Symptomatology of External Otitis (Table 2)
The most frequently reported symptom was ear pain (otalgia) in 94.4% of cases, indicating that inflammation and swelling in the external ear canal are key features of the disease. Pruritus (itching) was present in 82.5% of patients, suggesting an underlying fungal or allergic component in many cases. Ear discharge was noted in 70.6% of cases, which aligns with the presence of bacterial infections, particularly Pseudomonas aeruginosa, known for producing purulent otorrhea. Hearing loss was experienced by 53.2% of patients, most likely due to canal blockage from inflammation or debris.
These findings confirm that pain, itching, and discharge are the hallmark symptoms of external otitis, and their presence should prompt clinicians to initiate appropriate otoscopic evaluation and microbiological testing.
Table 2: Clinical Symptoms Reported by Patients
Symptom | Frequency (n) | Percentage (%) |
Ear pain | 119 | 94.4% |
Pruritus | 104 | 82.5% |
Ear discharge | 89 | 70.6% |
Hearing loss | 67 | 53.2% |
Swelling | 58 | 46.0% |
Risk Factors for External Otitis (Table 3)
The most common risk factors among patients with external otitis were swimming (48.4%), use of earphones/cotton buds (46.8%), and recent upper respiratory tract infections (35.7%). These findings align with the established understanding that moisture retention in the external ear canal, mechanical irritation, and secondary infections contribute to the development of external otitis.
Statistical analysis showed that the association between these risk factors and external otitis was not statistically significant (p = 0.082). However, given the high percentage of patients with these risk factors, preventive recommendations such as avoiding prolonged moisture retention, reducing excessive ear cleaning, and treating respiratory infections promptly remain crucial in reducing the risk of external otitis.
Table 3: Risk Factors Associated with External Otitis
Risk Factor | n (%) | p-value |
Swimming | 61 (48.4%) | 0.082 |
Use of earphones/cotton buds | 59 (46.8%) | |
Recent upper respiratory tract infection (URTI) | 45 (35.7%) | |
History of ear trauma | 32 (25.4%) | |
Underlying skin disease (eczema, psoriasis) | 21 (16.7%) |
Microbiological Profile (Table 4)
The microbiological analysis confirmed that bacterial infections were more common than fungal infections, with Pseudomonas aeruginosa isolated in 38.1% of cases, making it the most common causative organism of external otitis. Staphylococcus aureus (28.6%) was the second most frequently detected bacterial pathogen, consistent with its role in localized skin infections and secondary bacterial colonization.
Fungal infections were found in 17.4% of cases, with Aspergillus species (11.1%) being the most prevalent, followed by Candida species (6.3%). This indicates that fungal infections, though less common, should still be considered in patients presenting with chronic or recurrent external otitis, particularly in those with a history of antibiotic use.
Table 4: Microbiological Findings
Organism Isolated | n (%) |
Bacteria | |
Pseudomonas aeruginosa | 48 (38.1%) |
Staphylococcus aureus | 36 (28.6%) |
Escherichia coli | 9 (7.1%) |
Fungi | |
Aspergillus species | 14 (11.1%) |
Candida species | 8 (6.3%) |
No growth detected | 11 (8.8%) |
Treatment Outcomes Over Time (Figure 1)
The treatment response data demonstrated a steady improvement in symptoms over time. At Day 7, 35.7% of patients had complete resolution, while 53.2% showed partial improvement, indicating that the majority of patients required more than a week for full symptom relief. By Day 14, 66.7% had complete resolution, and by 1 Month, 87.3% of patients had fully recovered, demonstrating the effectiveness of antibiotic-steroid ear drops and systemic therapy.
The statistical analysis demonstrated a highly significant association between time and treatment response (p < 0.0001). These findings highlight that early diagnosis and prompt treatment can lead to rapid symptom resolution, reducing discomfort and preventing complications. Patients who did not achieve full symptom resolution by Day 14 required extended or modified treatment, emphasizing the need for individualized treatment strategies based on symptom severity.
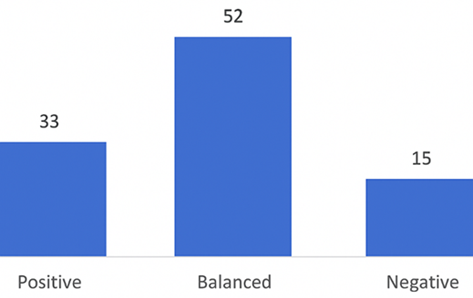
Figure 1: Treatment Outcomes Over Time
Recurrence and Associated Risk Factors (Table 5)
The recurrence rate was 9.5%, indicating that while most cases were successfully treated, a subset of patients experienced disease relapse. Among those who had recurrence, swimming (66.7%) and frequent earphone/cotton bud use (58.3%) were the most significant contributing factors. This supports the hypothesis that continued exposure to moisture and mechanical irritation predisposes individuals to recurrent infections.
A history of URTI (41.7%) and ear trauma (25.0%) were also notable risk factors, further emphasizing that preventive strategies should focus on patient education regarding water exposure, mechanical irritation, and ear hygiene.
Table 5: Risk Factors in Patients with Recurrence
Risk Factor | Recurrence Cases (n=12) | Percentage (%) | p-value |
Swimming | 8 | 66.7% | 0.063 |
Use of earphones/cotton buds | 7 | 58.3% | |
History of URTI | 5 | 41.7% | |
Ear trauma | 3 | 25.0% | |
Underlying skin disease | 2 | 16.7% |
Otitis externa (OE), commonly known as "swimmer's ear," is an inflammation of the external auditory canal, often resulting from bacterial infections.9 This study aimed to investigate the clinical presentation, risk factors, microbiological profile, and treatment outcomes of patients diagnosed with OE over a one-year period at the Department of Otorhinolaryngology, SVS Medical College, Mahabubnagar. The findings provide valuable insights into the epidemiology and management of OE, aligning with and expanding upon existing literature.[10]
Demographic Characteristics
The study encompassed 126 patients, with a higher prevalence observed in males (58.7%) compared to females (41.3%). The majority of cases occurred in the 15–29 years age group (31.0%), followed by the 30–44 years age group (27.8%). These findings are consistent with previous studies indicating a higher incidence of OE among younger individuals and males, potentially due to increased participation in activities such as swimming and use of earphones, which are recognized risk factors for OE.
Risk Factors
The most common risk factors identified were swimming (48.4%), use of earphones or cotton buds (46.8%), and recent upper respiratory tract infections (35.7%). Swimming has been well-documented as a significant risk factor for OE, as moisture can disrupt the protective lipid layer of the ear canal, facilitating bacterial growth.[11] The use of earphones and cotton buds can cause mechanical trauma to the ear canal, leading to microabrasions that serve as entry points for pathogens.[12] These findings are in line with existing literature that highlights moisture and mechanical trauma as primary contributors to the development of OE.[13]
Microbiological Profile
The microbiological analysis revealed that Pseudomonas aeruginosa was the most commonly isolated pathogen, accounting for 38.1% of cases, followed by Staphylococcus aureus at 28.6%. This aligns with numerous studies that have identified these two bacteria as the predominant causative agents of OE.[14,15] The high prevalence of Pseudomonas aeruginosa is particularly associated with environments where water exposure is common, reinforcing the link between swimming and OE.16
Treatment Outcomes
Treatment primarily involved the use of topical antibiotic-steroid ear drops, with or without systemic antibiotics. By Day 7, 35.7% of patients achieved complete resolution of symptoms, which increased to 66.7% by Day 14 and 87.3% by one month. This progressive improvement underscores the effectiveness of topical therapy in managing OE, consistent with guidelines that recommend topical antimicrobials as the first-line treatment.[17] The addition of corticosteroids in the ear drops likely contributed to the reduction of inflammation and expedited symptom relief. [18]
Recurrence and Risk Factors
Among the 126 patients, 12 (9.5%) experienced recurrence within six months. The most significant risk factors for recurrence were swimming (66.7%) and use of earphones or cotton buds (58.3%). This suggests that ongoing exposure to these risk factors may predispose individuals to recurrent episodes of OE. Patient education on preventive measures, such as keeping the ears dry and avoiding insertion of objects into the ear canal, is crucial in reducing recurrence rates. [19]
The findings of this study are consistent with previous research on OE. For instance, a study by Ninkovic et al. reported that Pseudomonas aeruginosa and Staphylococcus aureus are the most common pathogens in OE,[20] and in a review, Khatri et al., observed that topical antibiotic therapy is highly effective in treating the condition.[21] Additionally, the identification of swimming and mechanical trauma as significant risk factors aligns with existing literature.[22,23]
Clinical Implications
The study reinforces the importance of recognizing and addressing modifiable risk factors in the management of OE. Clinicians should educate patients on preventive strategies, such as drying the ears after water exposure and avoiding the use of earphones or cotton buds that can cause trauma to the ear canal. Early intervention with appropriate topical therapy remains the cornerstone of treatment, with systemic antibiotics reserved for cases with extensive infection or in immunocompromised individuals.
Limitations and Future Directions
While this study provides valuable insights, it has limitations that should be acknowledged. The study was conducted at a single center, which may limit the generalizability of the findings. Additionally, the follow-up period was limited to six months; longer follow-up could provide more information on recurrence rates and long-term outcomes. Future studies could explore the effectiveness of various preventive measures and the role of patient education in reducing the incidence and recurrence of OE.
This study contributes to the understanding of OE by highlighting its epidemiology, risk factors, microbiological profile, and treatment outcomes. The findings underscore the importance of preventive measures and effective topical therapy in managing OE. Continued research and patient education are essential to further reduce the burden of this common condition.
The authors declare that they have no conflict of interest
No funding sources
The study was approved by the SVS Medical college Hospital , Mahabubnagar ,Telangana, India ,509001
Sander R.; "Otitis Externa: A Practical Guide to Treatment and Prevention" American Family Physician 63.5 (2001) Pp. 927–937.
Wijesekera et al.; "Effects of Seasonal, Geographical, and Demographic Factors on Otitis Externa Microbiota in Queensland, Australia" Australian Journal of General Practice 53.11 Suppl (2024).
Medina-Blasini et al.; "Otitis Externa" StatPearls (2020). Available at www.ncbi.nlm.nih.gov/books/NBK556055/ [Accessed 1 March 2025].
Wiegand et al.; "Otitis Externa—Investigation and Evidence-Based Treatment" Deutsches Ärzteblatt International 116.13 (2019) Pp. 224–234. https://doi.org/10.3238/arztebl.2019.0224.
Wang et al.; "Ear Problems in Swimmers" Journal of the Chinese Medical Association 68.8 (2005) Pp. 347–352. https://doi.org/10.1016/S1726-4901(09)70174-1.
Chidlow et al.; "Otitis Externa—Climatic Associations and Evidence-Based Management Strategies for Australian Practice" Australian Journal of Rural Health 27.3 (2019) Pp. 251–256. https://doi.org/10.1111/ajr.12516.
Wiegand et al.; "Otitis Externa" Deutsches Ärzteblatt International 116.13 (2019) Pp. 224–234. https://doi.org/10.3238/arztebl.2019.0224.
Kullar et al.; "Infections and Foreign Bodies in ENT" Surgery 30.11 (2012) Pp. 590–596. https://doi.org/10.1016/j.mpsur.2012.09.005.
Gore et al.; "Otitis Externa" Journal of the American Academy of Physician Assistants 31.2 (2018) Pp. 47–48. https://doi.org/10.1097/01.JAA.0000529781.69812.8e.
Klein et al.; "The Burden of Otitis Media" Vaccine 19 Suppl. 1 (2000) Pp. S2–S8. https://doi.org/10.1016/S0264-410X(00)00271-1.
Wade et al.; "The Incidence and Health Burden of Earaches Attributable to Recreational Swimming in Natural Waters: A Prospective Cohort Study" Environmental Health 12 (2013) Pp. 67. https://doi.org/10.1186/1476-069X-12-67.
Hobson et al.; "Use and Abuse of Cotton Buds" Journal of the Royal Society of Medicine 98.8 (2005) Pp. 360–361. https://doi.org/10.1177/014107680509800808.
Baoum et al.; "Epidemiology, Risk Factors, and Monitoring of Acute Otitis Externa" International Journal of Community Medicine and Public Health 8.12 (2021) Pp. 6155–6159. https://doi.org/10.18203/2394-6040.ijcmph20214620.
Almuhayawi et al.; "Molecular Profile and the Effectiveness of Antimicrobial Drugs Against Staphylococcus aureus and Pseudomonas aeruginosa in the Diagnostic Approaches of Otitis Infection" Infection and Drug Resistance 16 (2023) Pp. 4397–4408. https://doi.org/10.2147/IDR.S418685.
Duarte et al.; "Methicillin-Resistant Staphylococcus aureus in Acute Otitis Externa" World Journal of Otorhinolaryngology–Head & Neck Surgery 4.4 (2017) Pp. 246–252. https://doi.org/10.1016/j.wjorl.2017.09.003.
Hajjartabar et al.; "Poor-Quality Water in Swimming Pools Associated with a Substantial Risk of Otitis Externa Due to Pseudomonas aeruginosa" Water Science & Technology 50 (2004) Pp. 63–67. https://doi.org/10.2166/WST.2004.0020.
Rosenfeld et al.; "Clinical Practice Guideline: Acute Otitis Externa" Otolaryngology–Head and Neck Surgery 150.1 Suppl (2014) Pp. S1–S24. https://doi.org/10.1177/0194599813517083.
Hajioff et al.; "Otitis Externa" BMJ Clinical Evidence (2015) Pp. 0510. PMID: 26074134; PMCID: PMC4466798.
Raza et al.; "An Audit of the Management of Otitis Externa in an ENT Casualty Clinic" Journal of Laryngology & Otology 109 (1995) Pp. 130–133.
Ninkovic et al.; "Microbiology of Otitis Externa in the Secondary Care in United Kingdom and Antimicrobial Sensitivity" Auris Nasus Larynx 35.4 (2008) Pp. 480–484. https://doi.org/10.1016/j.anl.2007.09.013.
Khatri et al.; "Topical Antibiotic Treatments for Acute Otitis Externa: Emergency Care Guidelines from an Ear, Nose, and Throat Perspective" Emergency Medicine Australasia 33.6 (2021) Pp. 961–965. https://doi.org/10.1111/1742-6723.13874.
Pantazidou et al.; "Risk Analysis of Otitis Externa (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece" Water 14.13 (2022) Pp. 1983. https://doi.org/10.3390/w14131983.
Schaefer et al.; "Acute Otitis Externa: An Update" American Family Physician 86.11 (2012) Pp. 1055–1061.
