+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3271
ISSN (Online) : 2709-3263
Background: The goal of the current study was to evaluate the effects of intravenous ferric carboxymaltose and iron sucrose on the mean serum iron level in the treatment of iron deficiency anaemia in pregnancy. Material & Methods: The Kamla Nehru State Hospital for Mother and Child at Indira Gandhi Medical College Shimla conducted this prospective study from June 1 through May 31, 2020. The study involved 86 pregnant women with iron deficiency anaemia. The participants were randomly divided into two equal groups, one of which got iron sucrose intravenously and the other, ferric carboxymaltose. At 2 and 4 weeks of follow-up, the treatment's effectiveness in terms of the mean serum iron value was evaluated. Results: Maximum subjects were in age group 21 – 25 years and belong to lower middle class according to modified Kuppuswamy scale in both groups. In group A the mean value of baseline serum iron was found to be 35.94 ug/dL while in group B, the mean value of baseline serum iron was found to be 36.17 ug/dL. The baseline mean serum iron (p value = 0.881) were comparable in group A and B. The mean serum iron at 2 and 4 weeks in group A was 114.67 ug/dL and 137.95 ug/dL respectively whereas the mean serum iron in group B was 92.75 ug/dL and 111.03 ug/dLat 2 and 4 weeks respectively. The difference between the two groups was statistically significant. Conclusion: The present study concluded that intravenous ferric carboxymaltose is more efficacious in improvement of meanserum iron level and the difference between the two groups was statistically significant.
Throughout pregnancy, total iron requirements increase to meet the major hematologic changes of the mother and the increasing demands the growing fetus. During pregnancy, requirements for absorbed iron increases from 0.8 mg/day in the first trimester to 7.5 mg/day in the third trimester, the average being 4.4 mg/day. The total iron requirement in pregnancy is around 1,240 mg. However, the net iron loss in pregnancy is approximately 630 mg. Sufficient amount of iron is essential for oxygen delivery to the maternal-placental-fetal unit to meet the increased oxygen demand during pregnancy [1,2].
Changes in hemoglobin concentration is considered late indicator of iron deficiency but is important for determining iron deficiency anemia.Intravenous iron preparations like iron sucrose and ferric carboxymaltose are available for the treatment of iron deficiency anemia. Parenteral iron can be used in second and third trimester and during the postpartum period [3].
Iron sucrose was FDA approved in November 2000. Iron sucrose is an iron hydroxide sucrose complex in water with a molecular weight of 34,000 - 60,000 daltons. The drawbacks of iron dextran are overcome by iron sucrose but it’s disadvantage includes multiple infusions to achieve the target hemoglobin concentration and thus prolonged hospital stay. Rapid administration of iron sucrose also leads to over saturation of transferrin leading to transient adverse events in the form of nausea, vomiting, abdominal pain and hypotension [4].
Intravenous ferric carboxymaltose is a parenteral dextran free iron. FCM comprises a macromolecular iron hydroxide complex of polynuclear iron (III) hydroxide in a carbohydrate shell. FCM has a molecular weight of around 150,000 daltons. In FCM, iron hydroxide is tightly bound within a carbohydrate shell which causes gradual release of iron in the body, thus avoiding acute toxicity and allowing large amounts of iron to be delivered. This results in a wider therapeutic window. Whereas incase of less stable complexes, there is rapid release of iron which causes high level of transferrin saturation and increase in non-transferrin bound iron (NTBI) which is toxic to the body [4].
The present study was aimed to compare the Change in the Mean Serum Iron Level after Intravenous Ferric Carboxymaltose and Iron Sucrose in the treatment of Iron Deficiency Anemia in Pregnancy.
Aims and Objectives
To compare the Change in the Mean Serum Iron Level after Intravenous Ferric Carboxymaltose and Iron Sucrose in the treatment of Iron Deficiency Anemia in Pregnancy.
This study was carried out in the Department of Obstetrics and Gynecology, Kamla Nehru State Hospital for Mother and Child, Indira Gandhi Medical College, after approval from hospital ethical committee, from 1st June 2019 to 31st May 2020 for a period of one year.
Study Design
Prospective study
Study Population
The study included 86 antenatal women with iron deficiency anemia.
Inclusion Criteria
Gestational age 12 to 36 weeks
Hemoglobin 7 – 9.9 g/dl
Microcytic hypochromic anemia on peripheral blood smear
Exclusion Criteria
Gestational age < 12 weeks or > 36 weeks
Prior history of blood transfusion
Anemia not caused by iron deficiency
History of disease associated with iron overload (thalassemia, hemochromatosis).
Known hypersensitivity to parenteral iron.
Chronic renal / hepatic or cardiovascular disease.
Not consenting
Methodology:
This was a hospital based randomized prospective interventional study. Enrolled women after fulfilling the inclusion and exclusion criteria were randomly assigned into two equal groups. Randomization in 1:1 ratio was carried out by computer generated simple random tables.
Group A received intravenous FCM.
Group B received intravenous iron sucrose.
The sample size was calculated by taking confidence interval as 95%, power of the study as 80% and mean difference of Hb to be detected between the two groups as 0.5 g/dl. The sample size was calculated using Epi software.
The final sample size was 86.
43 subjects received intravenous FCM in Group A.
43 subjects received intravenous iron sucrose in Group B.
Demographic data like age, educational qualification, socioeconomic status were recorded. Detailed menstrual, obstetrics and dietary history was taken from all the subjects.
Parameters used for the diagnosis of iron deficiency anemia was Serum iron
PARAMETER | NORMAL RANGE | IDA |
Serum Iron (µg/dL) | 50 – 170 | < 50 |
In both the groups, these investigations were done prior to infusion and at 2 and 4 weeks post infusion.
GROUP A: Ferric carboxymaltose (FCM)
The subjects included in this group received single dose of 1000 mg intravenous FCM. 1000 mg FCM was diluted in 250 ml of normal saline and was transfused over a period of 30 minutes.
GROUP B: IRON SUCROSE (ISC)
The total required dose of iron sucrose was calculated by using formula:
Total iron deficit (mg) = Pre pregnancy body weight (kg) × (Target Hb – Actual Hb) × 2.4 + Depot iron (mg)
Target Hb = 11 g/dL
Depot Hb = 15 mg/kg if body weight < 35 Kg and 500 mg if body weight > 35 Kg.
Intravenous iron sucrose was given in a dose of 200 mg diluted in 200ml of normal saline over a period of 30 minutes on alternate days until required dose was administered.
All the subjects included in the study were administered antihelminthic therapy with tablet albendazole 400mg first dose followed by repeat dose after 14 days.
In both the groups the general condition of the patient, blood pressure and pulse rate was examined every 5 minutes during transfusion and fetal heart rate was checked before and after transfusion. Both the groups were observed for adverse reactions for 4 hours post infusion.
Outcomes were assessed by measuring Serum Iron level 2 and 4 weeks post infusion. The rise in Serum Iron was assessed at 2 and 4 weeks post infusion in both the groups and compared at 4 weeks with respect to the baseline estimate.
Complete blood count measurements were done by an automated blood analyser machine, model MSTM 39S.
Statistical Analysis
Data was entered in Microsoft Excel spreadsheet and analysed using Epi Info Software version 7.2.2. Descriptive statistics were presented as proportions and their 95% confidence interval for qualitative variables whereas for quantitative variables means and their standard deviation were calculated. Independent student’s T- test was used for comparison of change in variables between the two groups. A two sided p value <0.005 was considered statistically significant.
Observations
A prospective study comparing the Change in the Mean Serum Iron Level after Intravenous Ferric Carboxymaltose and Iron Sucrose in the treatment of Iron Deficiency Anemia in Pregnancy was conducted in the Department Of Obstetrics and Gynaecology, Kamla Nehru State Hospital For Mother And Child (KNSH for M&C), Shimla, Himachal Pradesh with effect from (w.e.f.). 1st June 2019 to 31st May 2020.
In our study 86 antenatal women fulfilling the inclusion criteria were taken and divided into two equal groups. Group A was labelled for those study participants who received single dose of intravenous ferric carboxymaltose whereas group B were those study participants who received iron sucrose in multiple doses.
In group A, there were 2 participants in 18 - 20 years of age group, 21 participants in 21 - 25 age group, 15 participants in 26 - 30 age group and 5 participants in 31 - 35 age group. In group B, there were 6 participants in 18 - 20 years age group, 18 participants in 21 - 25 years of age group, 14 participants in 26-30 age group, 4 participants in 31 - 35 age group and 1 participant in 35 - 40 age group. It was observed that maximum subjects were in the age group of 21-25 years in both the groups.
In group A, 9 participants were in the period of gestation between 21 to 25+6 weeks, 18 participants between 26 to 30+6 weeks and 16 participants between 31 to 36 weeks. In group B, 5 participants were in the period of gestation 21 to 25+6 weeks, 22 participants between 26 to 30+6 weeks and 16 participants between 31 to 36 weeks. In our study 41.9% of the subjects in group A and 51.2% of the subjects in group B were between the period of gestation 26 to 30+6 weeks.
Among parity distribution, 65.1% belonged to multigravida and 34.9% belonged to primigravida in group A. Whereas 60.5% belonged to multigravida and 39.5% belonged to primigravida in group B.
In group A, only 1 participant belonged to class I, 3 participants belonged to class II, 32 participants belonged to class III, 6 participants belonged to class IV while 1 participant belonged to class V. In group B, 3 participants each belonged to class I and II, 30 participants belonged to class III, 6 participants belonged to class IV whereas only 1 participant belonged to class V. It was observed that maximum subjects in both the groups belonged to class III (lower middle class) according to modified Kuppuswamy scale (74.4% in group A and 69.8% in group B).
In group A all the subjects were having normal BMI (between 18.5 - 24.9 kg/ m2). Whereas in group B, only 1 subject was underweight (BMI < 18.5 kg/m2) and rest of the subjects were having normal BMI.
All the subjects included in group A received a single dose of 1000 mg FCM. Out of 43 participants in group B, 25.6% received dose of ISC between 801 - 850 mg. The mean dose of ISC was 831.26 mg.
In group A the mean value of baseline serum iron was found to be 35.94 ug/dL while in group B, the mean value of baseline serum iron was found to be 36.17 ug/dL. The baseline variables that is mean serum iron (p value = 0.881) were comparable in group A and B. The mean serum iron at 2 and 4 weeks in group A was 114.67 ug/dL and 137.95 ug/dL respectively whereas the mean serum iron in group B was 92.75 ug/dL and 111.03 ug/dL at 2 and 4 weeks respectively. The difference between the two groups was statistically significant.
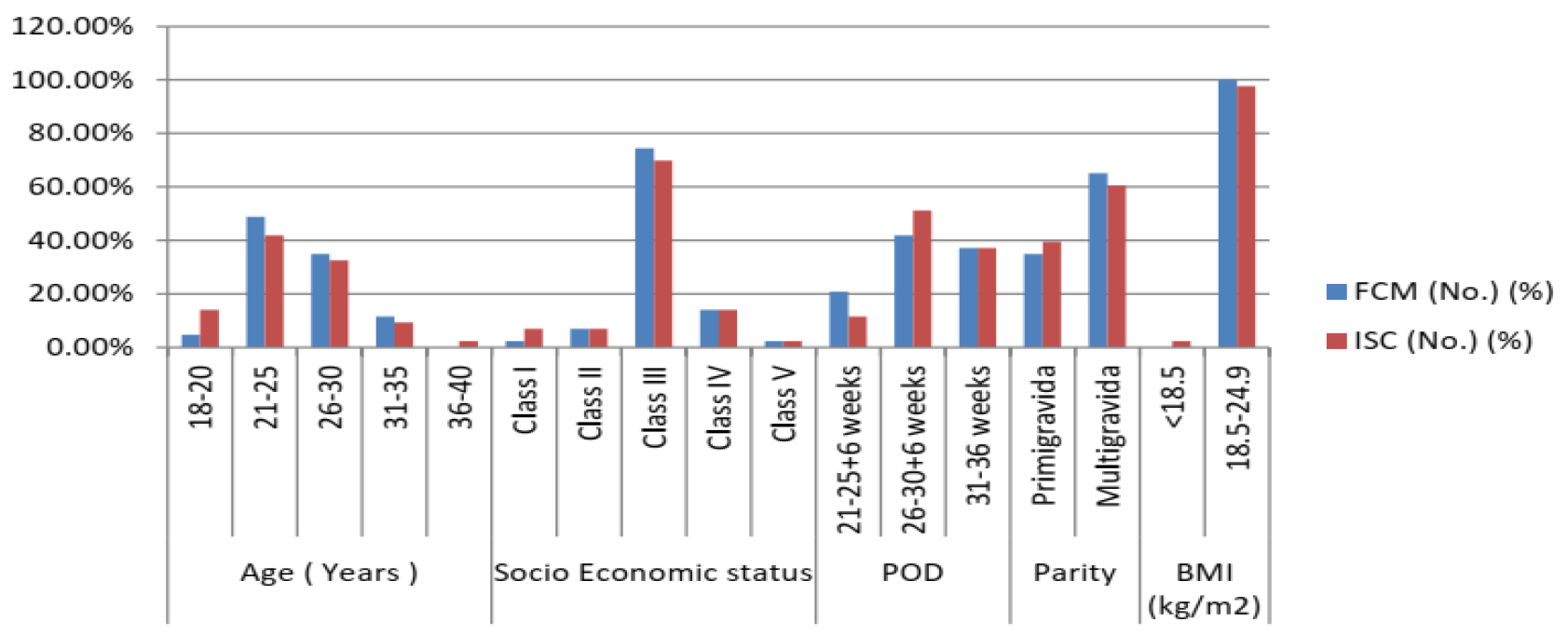
Figure 1: Comparison of Socio-demographic variables in both groups
Table 1: Dose of Ferric Carboxymaltose and Iron Sucrose
Dose of FCM | Frequency (No.) | Proportion |
1000 mg | 43 | 100.0 |
Dose of ISC |
|
|
650 - 700 mg | 1 | 2.3 |
701 - 750 mg | 7 | 16.3 |
751 - 800 mg | 6 | 14.0 |
801 - 850 mg | 11 | 25.6 |
851 - 900 mg | 8 | 18.6 |
901 - 950 mg | 6 | 14.0 |
951 - 1000 mg | 2 | 4.7 |
1001 - 1050 mg | 2 | 4.7 |
Total | 43 | 100.0 |
Mean Dose of ISC | 831.26 mg | |
Table 2: Change in Serum Iron in Group A And B
| Group A (FCM) | Group B (ISC) | P. Value |
Serum Iron at baseline | 35.9±8.1 | 36.1±6.4 | 0.881 |
Serum Iron at 2 weeks | 114.6±12.1 | 92.7±8.4 | <0.001 |
Serum Iron at 4 weeks | 137.9±17.1 | 111.0±11.4 | <0.001 |
p value < 0.001 (significant)
Table 3: Independent T-Test for comparison between two groups
| Gp Code | Mean | Std. Deviation | Std. Error Mean | |||||||
Diff_Iron_4wk | A | 102.01 | 14.023 | 2.138 | |||||||
B | 74.86 | 10.019 | 1.528 | ||||||||
Independent T-Test for comparison between two groups | |||||||||||
Gp A v/s Gp B | F | t | Sig. (2-tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval of the Difference | |||||
Lower | Upper | ||||||||||
Diff_Iron_4wk | 5.035 | 10.331 | <0.001 | 27.151 | 2.628 | 21.925 | 32.378 | ||||
The present study was conducted with the objective to compare the change in the mean serum iron level after intravenous ferric carboxymaltose and iron sucrose in the treatment of iron deficiency anemia in pregnancy. In the present study the subjects after treatment with intravenous ferric carboxymaltose and iron sucrose were followed up at 2 and 4 weeks.
Over 90% of iron deficiency anemia is associated with depleted iron stores. Insufficient supply of iron causes inability to sustain a normal hemoglobin concentration, therefore iron deficiency anemia develops. In our study all the subjects had low serum iron before the start of treatment and baseline value of serum iron was 35.9 ug/dL in the FCM group and 36.1 ug/dL in ISC group which was comparable. The rise in serum iron at 4 weeks was 102.01 ug/dL in group A and 74.86 ug/dL in group B which was observed to be of statistical significance. Whereas Naqash et al., [5] followed up patients at 4 weeks only and documented a significant rise in serum iron in subjects treated with ferric carboxymaltose compared to iron sucrose (59.4 ug/dL versus 54.01 ug/dL respectively) with p value 0.0001. Whereas Jose et al., [6] followed up patients at 3 weeks and found that the difference in serum iron between two groups was not statistically significant (p value 0.30).
The present study concluded that intravenous ferric carboxymaltose is more efficacious in improvement of mean serum iron level and the difference between the two groups was statistically significant.
Milman, N. “Iron and Pregnancy—A Delicate Balance.” Annals of Hematology, vol. 85, no. 9, September 2006, pp. 559–565.
Bothwell, T.H. “Iron Requirements in Pregnancy and Strategies to Meet Them.” The American Journal of Clinical Nutrition, vol. 72, no. 1, July 2000, pp. 257S–264S.
Milman, N. “Serum Ferritin in Healthy Danes: Relation to Marrow Haemosiderin Iron Stores.” Danish Medical Bulletin, vol. 30, 1983, pp. 115–120.
Suchdev, P.S., et al. “Assessment of Iron Status in Settings of Inflammation: Challenges and Potential Approaches.” The American Journal of Clinical Nutrition, vol. 106, suppl. 6, December 2017, pp. 1626S–1633S.
Naqash, A., et al. “Effectiveness and Safety of Ferric Carboxymaltose Compared to Iron Sucrose in Women with Iron Deficiency Anemia: Phase IV Clinical Trials.” BMC Women’s Health, vol. 18, no. 1, December 2018, pp. 1–10.
Jose, A., et al. “Comparison of Ferric Carboxymaltose and Iron Sucrose Complex for Treatment of Iron Deficiency Anemia in Pregnancy—Randomised Controlled Trial.” BMC Pregnancy and Childbirth, vol. 19, no. 1, December 2019, pp. 1–8.
