+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-328X
ISSN (Online) : 2709-3298
Marfan syndrome (MFS) is a connective tissue disorder leading to multisystem abnormalities mainly skeletal, cardiovascular system and ocular manifestations. It has an autosomal dominant inheritancewhich is why familial cases occur frequently. It is caused by mutations in the fibrillin gene present on chromosome 15.1Ocular manifestations are common. These are increased axial length, decreased corneal curvature, greater corneal astigmatism, myopia, ectopia lentis and retinal detachment. The diagnosis of MFS is clinical, but genetic testing is available.2A significant proportion of the patients of the with MFS are initially seen for an ocular pathology mainly decreased vision and diagnosed by an ophthalmologist. Thus, alertness of the ophthalmologists when examining a patient with suspicious ocular findings can help in the early diagnosis. Early diagnosis and management have significantly increased the life expectancy in these patients. These patients should be examined regularly to identify potential complications.
Marfan syndromeis an autosomal dominant connective tissue disorder, caused by mutations in the fibrillin gene. Fibrillin is a component of elastin. This disease affects all organs of the body. The major manifestations of marfan syndrome are descending aortic root aneurysm/dissection and ectopia lentis.
The diagnosis of MFS is clinical, but genetic testing is available. Diagnostic criteria for Marfan syndrome were updated in 2010 (Ghent 2 criteria) and include ectopia lentisas a major criterion.2Aortic root aneurysm/dissection is also included as another major diagnostic criteria. This increases the importance of a careful ocular examination in these patients. Myopia exceeding 3.0 D is now an ocular criterion if Ectopia lentis is not present, along with the other systemic manifestations.
A twenty-one-year-oldgirl came with progressive diminution of vision. Initially, -2 diopters spherical lenses were prescribed. Anewpair of glasses were prescribed to her at every visit to optometrist due to a rapid progression of the myopia, which reached the value of -6 D when she was seven years old.
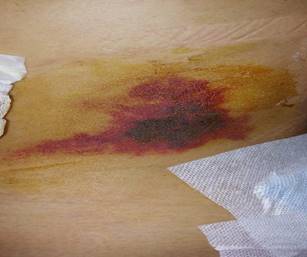
Figure 1: Image showing subluxated lens in the left eye
On Ophthalmological examination, best corrected vision was finger counting one meter in right eye and 6/18 in left eye with -6D spherical lenses i.e. high myopia was documented. The keratometry value of the right eye was 41.00 D and for the left eye it was 41.25 D. Axial lengthwas 25mm in both the eyes. On anterior segment examination, there was supero-nasal subluxationof the clear lens (Figure 1). The fundus was normal in both the eyes. We also notedtall stature, thinness (Size =1.40 m, weight = 25 kg for a Body Mass), arachnodactyly, a longer upper limb (Figure 2 and 3). Further history from parents revealed exceptional flexibility of the joints of this girl, as well as its large size compared to other children of the same age in the family. There was no history of similar complaints in any of the family member.
Figure 2: image showing Arachnodactyly
Patient was referred to physician examination for any systemic manifestations.
The systemic examination was normal. Diagnosis of marfan syndrome was made on the basis of these features.
Vitrectomy with lensectomy and scleral fixated intraocular lens was carried out on the right side. The post-operative period was uneventful. After six months, patient presented with diminution of vision in the right eye which was sudden in onset and was painless. On examination, best corrected vision was hand movement close to face. Anterior segment was normal. On fundus examination, Rhegmatogenous retinal detachment was documented in the right eye and surgerywas done. Patient had raised intraocular pressure after surgery andwas started on antiglaucoma medications (Figure 4). At present, patient does not perceive light in the right eye and the best corrected vision was 6/36 in the left eye. Most recent cardiovascular evaluation was normal.
Figure 3: Dysmorphic facial features
Figure 4: Right eye
Marfan’s syndrome is associated with a mutation in the fibrilln gene (FBN1). This gene is located over chromosome 15.1There is reported incidence of 1 in 3000 to 5000 individuals. It manifests to variable extents of severity among different individuals. The classic symptoms involve three organs i.e. eyes, skeletal and cardiovascular system.3These patients mostly had a tall stature, arachnodactyly with positive wrist and thumb sign.
Clinically, ectopia lentis is bilateral in 80-90% of Marfan patients and is stable from childhood. On examination, patients show refractive instability with myopia and astigmatism, iridodonesis and phacodonesis due to lens subluxation or dislocation. Superotemporal is the most common direction of dislocation on examination. There may be secondary complications such as phacolytic uveitis from posterior subluxation of the lens. Retinal tears and detachments are also common inthese patients. Other ocular manifestations of Marfan syndrome include flattened cornea (causing astigmatism), keratoconus, increased globe length (causing myopia), iris coloboma, cataracts, glaucoma, strabismus, amblyopia, and vascular malformations.4All these findings isdue to the abnormality of fibrillin in the ocular connective tissue of the Marfan patient. There are varied systemic manifestations, the most common of which are the musculoskeletal abnormalities. They exhibit arachnodactyly (spider fingers) with the ability to dramatically encircle the wrist (Walker-Murdoch sign). In addition, they often have pectus excavatum, a high-arched palate, and facial abnormalities. The cardiovascular findings range from mild mitral valve prolapse to severe aortic aneurysm or dissection; these cardiac manifestations are the primary causes of mortality among Marfan patients. Pulmonary diseases include apical blebs or spontaneous pneumothorax. Patients with Marfan syndrome need regular eye examinations to identify potential complications.
The ophthalmological findings are important in the diagnosis of many systemic diseases. Some diseases may present with only eye symptoms and can lead to early diagnosis and treatment of the disease. Thus, the ophthalmologist should always be vigilant about ophthalmological findings like in our case. In these cases, never forget cardiovascular monitoringand assessment is of paramount importance because the mortality of this disease is related to its cardiovascular complications.
Waduthantri, S. "Ocular Manifestations of Marfan’s Syndrome." Medical Journal of DY Patil University, vol. 10, 2017, pp. 118-119.
Salchow, D. J., and P. Gehle. "Ocular Manifestations of Marfan Syndrome in Children and Adolescents." European Journal of Ophthalmology, vol. 29, no. 1, 2019, pp. 38-43. DOI: 10.1177/1120672118761333.
Maumenee, I. H. "The Eye in the Marfan Syndrome." Transactions of the American Ophthalmological Society, vol. 79, 1981, pp. 684-733. PMID: 7043871; PMCID: PMC1312201.
Konradsen, T. R., and C. Zetterström. "A Descriptive Study of Ocular Characteristics in Marfan Syndrome." Acta Ophthalmologica, vol. 91, no. 8, Dec. 2013, pp. 751-755. DOI: 10.1111/aos.12068. Epub 2013 Feb 7. PMID: 23387925.
