
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
Background: The present study was done to evaluate the diagnostic performance of mp MRI in suspected in Prostate Cancer Patients at tertiary care Hospital. Materials and Methods: Forty-four patients with suspected PCa on clinical assessment and/or raised serum PSA levels (>4ng/ml) were prospectively recruited. Patient who underwent prostatic biopsy prior to 68Ga-PSMA PET/CT and mp MRI, deranged renal function tests or coagulogram and refused consent were excluded. Out of total 44, 33 patients also underwent mp MRI. Out of the total 44 patients, 33 underwent biopsy. Only 22 out of these 33 patients underwent mp MRI. The images were interpreted and mp MRI reporting was done according to PIRADS v.2. Histopathology was taken as gold standard. Results: Mean age of patients was 66.61±9.3 years and Malignancy was detected in 16/33 (48.5%) patients who underwent biopsy. Out of these 22 patients, 9 were interpreted as PIRADS II, 3 patients were PIRADS III and 10 were given PIRADS score of IV/V. No patient was given a PIRADS score of 1. When PIRADS III-V were considered as positive lesions on mp MRI, the sensitivity, specificity, PPV, NPV and accuracy of mp MRI was 100%, 81.82%, 84.62%, 100% and 90.91% respectively to detect the adenocarcinoma PCa. When PIRADS III was considered as negative for malignancy, the sensitivity falls to 81.82%, specificity increases to 90.91%, PPV increased to 90%, NPV decreased to 83.33% and he overall accuracy decreased from 90.91 to 86.36%. Conclusions: Present study concluded that the Majority of the patients with PIRADS IV/V had a diagnosis of malignancy and mp MRI has high sensitivity, specificity, PPV, NPV and accuracy in diagnosis of Prostate Cancer.
Multiparametric MRI (mp MRI) is used to detect and evaluate the clinical significance of prostatic lesions, to assess loco-regional extension (T stage) and metastasis to lymph node or bone marrow in pelvic region. The usage of Diffusion-Weight Imaging (DWI) with Dynamic Contrast Enhanced Imaging (DCE) in mp MRI has shown to improve the sensitivity of MRI to 90%, specificity over 70% with negative predictive value of 95% for more than 3+3 Gleason score tumors [1,2].
Although mp MRI has a structured reporting system called Prostate Imaging Reporting and Data System (PIRADS), its wide clinical application is limited by inter observer variability and lack of reproducibility. Therefore, on account of the moderate specificity, the only way to make diagnosis in case of cancer remains biopsy of the prostate. Due to limitations of MRI, there is need of other imaging modalities which can be in this clinical scenario [3-5].
Aims and Objectives
To evaluate the diagnostic performance of mp MRI in suspected in Prostate Cancer Patients at tertiary care Hospital.
Study Design
Prospective pilot study.
Place of Study
This study has been conducted at the Department of Nuclear Medicine, PGIMER Chandigarh in collaboration with the Department Urology, Radiodiagnosis and Histopathology, PGIMER, Chandigarh.
Period of Study
The study was done during the period between January, 2018 and June, 2019.
Inclusion Criteria
Patients having suspicion of carcinoma prostate on clinical assessment and/or raised serum PSA levels (>4ng/ml)
Patient not suffering from bleeding diathesis or renal failure
Patient consent to participate in the study
Exclusion Criteria
Patient with prior diagnosed PCa or who underwent prostatic biopsy priorto68Ga-PSMA PET/CT and mp MRI
Patients with deranged renal function tests orcoagulogram
Patient refused to participate in the study
Study Population
A total of 44patients suspected for PCa on the basis of clinical assessment and/or raised PSA were recruited for the study.
Patients suspected for prostate adenocarcinoma and/or serum PSA levels >4ng/ml and willing to participate in the study were recruited. Study was approved by Institutional Ethics Committee, PGIMER Chandigarh. Written informed consent was obtained. After clinical assessment, mp MRI and68Ga-PSMA PET/CT were done. Biopsy was done in cases with high clinical suspicion of PCa (Figure 1).
Statistical Analysis
Qualitative variables are described using number and percentages. Normally distributed continuous quantitative data is described using mean and standard deviation. Skewed quantitative data is described using median and interquartile range. The normality of data will be checked by measures of Kolmogorov-Smirnov tests of normality. The sensitivity, specificity, NPV and PPV of mpMRI was estimated using a 2x2 table. The statistical analysis was conducted using the IBM SPSS STATISTICS (version 23.0).
In this prospective study, a total of 44 patients suspected to have PCa were recruited on the basis of clinical assessment and serum PSA levels. Out of total 44, 33 patients also underwent mpMRI. Out of the total 44 patients, 33 underwent biopsy. Only 22 out of these 33 patients underwent mpMRI. The images were interpreted and were categorised based on PIRADS V2.
Out of these 22 patients, 9 were interpreted as PIRADS II, 3 patients were PIRADS III and 10 were given PIRADS score of IV/V (Figure 2). No patient was given a PIRADS score of 1 (Figure 2). The patients with lesion on mp MRI were measured and the size of the lesion varied from ~1 x 1cm to ~4.4 x 4cm.The location of the lesion was also noted. Posterolateral peripheral zone, central zone and some lesions involving almost the entire prostate gland were noted. 11/22 (50%) patients who underwent mp MRI were diagnosed with malignancy. When PIRADS III-V were considered as positive lesions on mp MRI and compared with gold standard, the analysis revealed sensitivity, specificity, PPV, NPV and accuracy of mp MRI to be 100%, 81.82%, 84.62%, 100% and 90.91% respectively to detect the adenocarcinoma PCa. Table 1 and 2 showed the mp MRI results.
However, if we consider PIRADS III as negative for malignancy, the sensitivity falls from 100% to 81.82% and the specificity increases from 81.82% to 90.91%, PPV increased from 84.62% to 90%, NPV decreased from 100 to 83.33%. The overall accuracy decreased from 90.91 to 86.36%.
All the 9 patients who had a PIRADS score of II were negative for malignancy on histopathology. Majority of the patients with PIRADS IV/V (n = 9/10) had a diagnosis of malignancy except one patient who had a diagnosis of granulomatous prostatitis. 68Ga PSMA PET/CT was negative in this case. Out of the 3 patients with PIRADS III, 2 patients had positive finding on PET/CT and were diagnosed as adenocarcinoma on repeat biopsy while the remaining 1 was having no evidence of malignancy on biopsy.
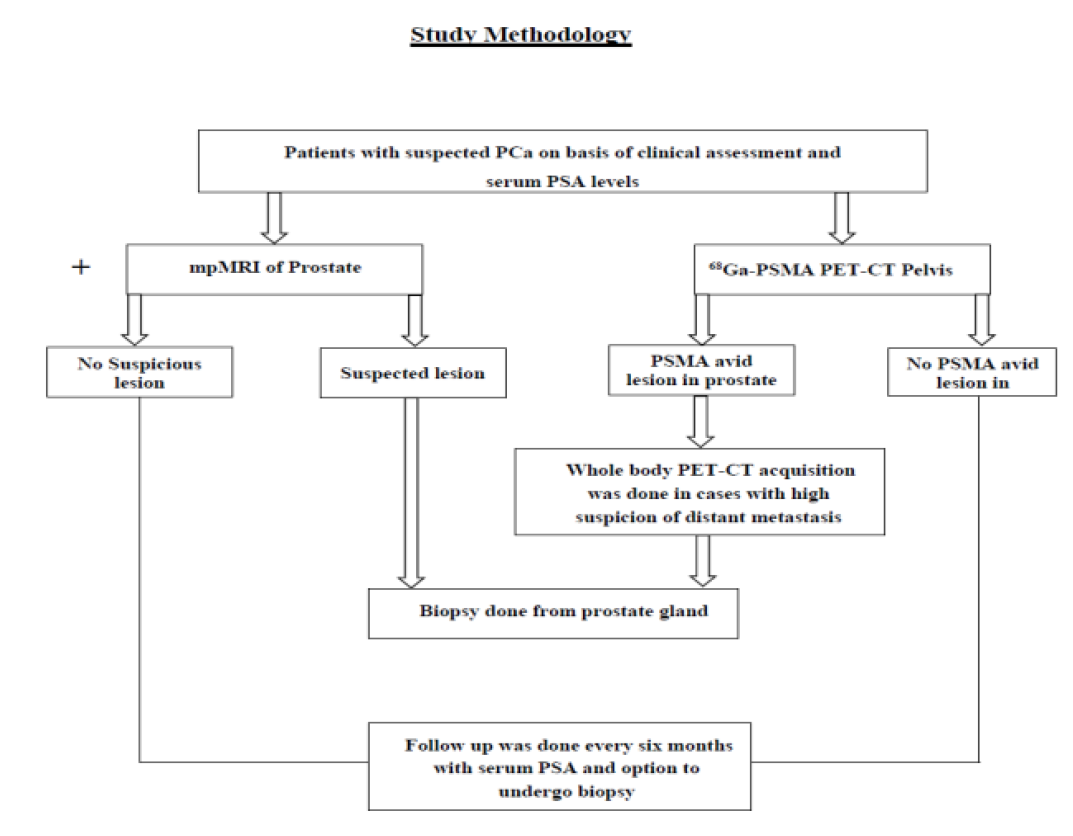
Figure 1: Study Methodology
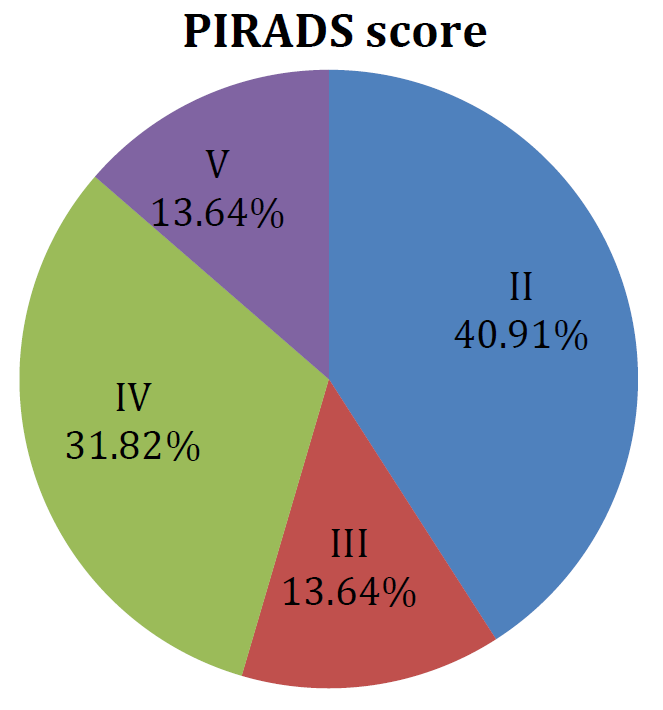
Figure 2: Pie Chart Showing Distribution of Percentage of Patients According to PIRADS (Prostate Imaging Reporting and Data System) Scoring
Table 1: Showing mp MRI (Multiparametric Magnetic Resonance Imaging) Results Compared with Biopsy
| Total Patients Analysed (n = 22) | Reference Standard for Malignancy | ||
Adenocarcinoma (n = 11) | Negative for malignancy (n = 11) | ||
| Mp MRI | Positive (n = 13) | 11 (TP)* | 2 (FP)* |
| Negative (n = 9) | 0 (FN)* | 9 (TN)* | |
*TP (True Positive), TN (True Negative), FP (False Positive) and FN (False Negative)
Table 2: Diagnostic Performance of mp MRI in Suspected PCa
Parameter (with 95% CI) | Mp MRI |
Sensitivity | 100% (71.51%-100%) |
Specificity | 81.82% (48.22%-97.72%) |
Positive Predictive Value | 84.62% (61.09%-95.07%) |
Negative Predictive Value | 100% |
Accuracy | 90.91% (70.84%-98.88%) |
Mp MRI is an established investigation with good diagnostic efficacy in detecting potentially significant PCa cases. Mp MRI reporting has a standardized protocol which is universally followed (PIRADS V2.0). However, there can be false positive interpretations due to complex reporting, inter-observer variability, reproducibility and contraindication in case of metallic implants/renal failure are few of the limitations [3]
In our study, mp MRI showed very high accuracy in our study when PIRADS score ≥3 was considered positive for PCa with sensitivity and specificity of 100 and 81.82% respectively. However, on taking PIRADS III as negative for malignancy the sensitivity falls to 81.82% and the specificity increases to 90.9%. A meta-analysis by Woo et al. [6], showed pooled sensitivity and specificity of mp MRI to be 0.89 and 0.73, respectively.
Present study concluded that the Majority of the patients with PIRADS IV/V had a diagnosis of malignancy and mp MRI has high sensitivity, specificity, PPV, NPV and accuracy in diagnosis of Prostate Cancer.
I. Berger et al. “68 Ga-PSMA PET/CT vs. mp MRI for locoregional prostate cancer staging: correlation with final histopathology.” Prostate Cancer and Prostatic Diseases, vol. 21, no. 2, 2018, pp. 204–211.
H.B. Carter “American Urological Association (AUA) guideline on prostate cancer detection: process and rationale: AUA guideline on prostate cancer detection.” BJU International, vol. 112, no. 5, 2013, pp. 543–547.
E.F. Dola et al. “Assessing the validity of prostate imaging reporting and data system version 2 (PI-RADS v2) scoring system in diagnosis of peripheral zone prostate cancer.” European Journal of Radiology, vol. 21, no. 4, 2017, pp. 19–26.
A. Heidenreich et al. “EAU guidelines on prostate cancer. part 1: Screening, diagnosis and local treatment with curative intent update 2013.” European Urology, vol. 65, no. 1, 2014, pp. 124–137.
C.H. Tan et al. “Dynamic Contrast-Enhanced MRI for the Detection of Prostate Cancer: Meta-Analysis.” AJR American Journal of Roentgenology, vol. 204, no. 4, 2015, pp. W439–W448.
S. Woo et al. “Diagnostic performance of prostate imaging reporting and data system version 2 for detection of prostate cancer: A systematic review and diagnostic meta-analysis.” European Urology, vol. 72, no. 2, 2017, pp. 177–188.
